
From the 1Department of Rehabilitation Medicine, Keio University School of Medicine, Shinjuku, Tokyo, 2Department of Rehabilitation, National Sanatorium Tamazenshoen, Higash-Murayama, 3Department of Rehabilitation, Saisei-kai Kanagawa Prefecture Hospital, Yokohama, 4Division of Health Promotion, Department of Health, Shinjuku Local Government, Shinjuku, 5Department of Rehabilitation, Keio University Hospital, 6Disaster Management Team, Medical Association of Shinjuku, Shinjuku and 7Yamamoto Clinic, Akebono-kai, Shinjuku, Tokyo, Japan
Objective: There are a lack of disaster preparedness measures that target populations with dysphagia. In particular, disaster response plans frequently overlook differences in textures between emergency foods and regularly consumed foods. The aim of this study was to estimate the number of community-dwelling elderly care recipients requiring specific food preparations, including the population at risk of aspiration when solely consuming common emergency foods.
Design: A cross-sectional study.
Patients: Community-dwelling elderly care recipients who were certified by the public long-term care insurance system in Japan and registered at one of 77 care managing offices in Shinjuku city.
Methods: Special needs regarding food intake and risks associated with receiving emergency foods were assessed by government-certified care managers.
Results: Data were acquired from 1,271 care recipients. Notably, 23.1% of the sampled population had special needs regarding food intake at all times (e.g. non-oral intake or need for texture-modified foods). An additional 11.5% were estimated to experience difficulty when ingesting common emergency foods, despite the ability to consume regular foods.
Conclusion: A relatively large portion of community-dwelling elderly people will be at risk of aspiration due to the intake of commonly distributed emergency foods following a disaster. Appropriate preparation based on an assessment of special needs regarding food intake is therefore required when planning for future disasters.
Key words: aspiration; disaster medicine; dysphagia; emergency food; long-term care; shelter-acquired pneumonia; preventive medicine; disaster rehabilitation.
Accepted Feb 8, 2019; Epub ahead of print Mar 6, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Michiyuki Kawakami, Department of Rehabilitation Medicine, Keio University School of Medicine, 35 Shinano-machi, Shinjuku city, Tokyo, Japan. E-mail: michiyukikawakami@hotmail.com
Emergency foods provided following disasters have considerably different textures from regularly consumed foods. This may lead to an increase in the rate of aspiration pneumonia in vulnerable populations after a disaster. However, no studies have focused on this issue. To better estimate the size of the population with swallowing disorders (i.e. dysphagia), a local district-based total population survey of community-dwelling elderly care recipients who were registered in the mandatory long-term care insurance system in Shinjuku city, Tokyo, Japan was performed. Data were collected by government-certified care managers. While 23.1% of the population experienced dysphagia in ordinary settings (i.e. non-oral nutrition intake or daily dependency on texture-modified foods), an additional 11.5% were identified as at-risk solely through a diet consisting of emergency foods. This study indicates the importance of preparedness measures that take this latter population into account.
Disaster rehabilitation aims to provide optimal care for health problems experienced by the affected population, manage various complications, and optimize function, while reducing disabilities in interaction with the environment. The past 20 years have seen a doubling in the number of disasters, which has been attributed to global climate change (1). Thus, this issue has become increasingly important. Prevention of aspiration pneumonia is an important goal of disaster rehabilitation (2). Vulnerable populations are presumed to face an increasing risk of aspiration in post-disaster settings, which is particularly related to a reduced ability to ingest emergency foods, such as pre-gelatinized rice and biscuits/crackers/cereals, which are often unfamiliar and not easily swallowed, particularly when provided in non-ordinary settings, such as temporary shelters (3, 4).
Recent epidemiological studies have revealed a remarkable increase in the prevalence of pneumonia among people displaced after disasters (5, 6). Specifically, elderly people and those with dysphagia related to neurological disorders are more likely to develop pneumonia beyond the first week after a disaster (7). This complication has been attributed to aspiration of emergency foods and is consequent to shortages in stores of texture-modified foods for vulnerable population (8). Notably, an inadaptability to ingest emergency food is not only seen in dysphagic patients, but may also occur in elderly people without symptomatic dysphagia who are able to consume regular food in ordinary settings, but who are experiencing a latent decline in the swallowing function (3, 4). To our knowledge, however, no previous study has investigated and estimated the potential risks associated with consuming emergency foods in a community-dwelling elderly population.
Vulnerable groups should be assessed and considered in public disaster preparedness planning (1). Studies have shown that elderly people are less likely to store items related to household preparedness (9). Comorbidities, such as dementia or functional disorders, together with insufficient social or familial support, restrict the ability of these residents to stockpile sufficient amounts of food for future disasters (5). Therefore, elderly populations are more likely to depend on public food supplies during catastrophes. However, countermeasures for these populations may be overlooked in the development of disaster preparedness and response plans (8). This underscores the critical importance of estimating the population that would require specific preparedness or assistance with nutritional intake in a disaster setting.
Thus, the present study aimed to estimate the community-dwelling elderly population with a dependence on a specific form of nutritional intake and specific food allocation, as well as those who would experience difficulty solely when ingesting standard emergency foods. The study therefore conducted a local district-based total population survey of community-dwelling elderly care recipients registered in the mandatory long-term care insurance (LTCI) system.
This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Keio University (Tokyo, Japan; No. 20160211). The study was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR) public database (number UMIN000023056).
For this study, emergency foods were defined as storable foods, including pre-gelatinized (alphanized) rice, canned porridge, biscuits/crackers/cereals, protein/granola bars, canned side dishes, trail mix/dried fruit, and ready-to-eat meals, in accordance with government documents (10, 11).
The LTCI system was implemented in Japan as a mandatory public healthcare insurance system. It aims to assist elderly individuals to lead more independent lives and to reduce the burden of care on their families (12). All care recipients are registered at a government-certified care managing office, where a licensed care manager (CM) evaluates the health and medical status of the client and formulates an individualized care plan (12). Approximately 17.7% of Japanese residents older than 65 years are certified by this system and have access to care. This population is classified into 7 levels according to the burden of care: Support Levels 1 and 2, and Care Need Levels (hereafter Care Levels) 1 through 5, with a higher number indicating a more intense level of care. People with dementia are generally classified into a Care Level, whereas those without dementia are classified into a Support Level. For this study, the 7 care levels were re-grouped into 3 grades as follows: Low (Support Levels 1 and 2, Care Level 1), Middle (Care Levels 2 and 3) and High (Care Levels 4 and 5).
This cross-sectional survey targeted community-dwelling recipients of care under the LTCI system. It was conducted in Shinjuku city within the Tokyo Metropolitan District in Japan, which was selected because of its relatively lower rate of ageing (percentage of people aged 65 years and older) within Japan and its consequently fair external validity with respect to other countries. All community-dwelling care recipients in this area were registered at one of 77 local CM offices. The present investigation was conducted through “Caremanet,” an organization of the Shinjuku district liaison council CM office to which all local CM offices belong. Thus, the target population comprised all community-dwelling care recipients in Shinjuku city. No additional selection criteria were applied. Surveys were hand-delivered to representatives from each CM office during a meeting on 25 September 2015 or were posted to offices whose representatives were absent from the meeting. Responses were accepted via fax, mail, or hand delivery until 16 October 2015. Data were analysed in 2016 after receiving approval from the ethics committee. In addition, assessors and their colleagues participated in a 3-h lecture delivered by board-certified physiatrists that addressed general knowledge about dysphagia, disaster preparedness from the standpoint of dysphagia, and the explanation of the specific questionnaire used in the study. Seventy-eight representatives from 56 CM offices attended the lecture.
In the survey, respondents were asked about the number of care recipients in each care grade who met the criteria for dysphagia/nutrition states (A) through (E) as follows: (A) intravenous hyper-alimentation, (B) nasoenteric tube and gastric/intestinal fistula, (C) texture-modified foods/thickened liquids, (D) normal, but difficulties with ingestion of emergency foods, and (E) no notable problems. To distinguish care recipients in categories D and E, CMs used the Seirei dysphagia screening questionnaire (Table SI1), an easy screening questionnaire that is considered highly reliable and valid (13, 14). The Seirei questionnaire was originally established as a self-reported questionnaire comprising 15 different items. In this questionnaire, the practical status is classified into severely impaired, mildly impaired or intact for each item. CMs were asked to evaluate the existence of signs of aspiration noted when they observed the consumption of emergency foods or foods with similar attributes by their care recipients. CMs were also allowed to discuss this issue with care recipients or their families. Elderly individuals with at least 1 severe symptom related to the consumption of emergency foods were categorized into class D (13).
Shinjuku city is one of 23 special wards of the Tokyo Metropolis. Although it is well known as the New Urban Center, according to the Tokyo Metropolitan Government, it comprises a wide variety of components, including highly urbanized business, shopping malls and restaurants, high-end residential areas, hotels, and downtown zones. Currently, Shinjuku has a population of more than 330,000 residents and an ageing rate of 19.5%, which is very similar to those of many developed countries, including Sweden (19.9%), France (19.1%), and Germany (21.2%) (15). Currently, 13,022 residents of Shinjuku are certified in the LTCI system.
The χ2 test was used to evaluate differences in the prevalence of care levels between Shinjuku city and all of Japan. Cramer’s coefficient of association was calculated to compare numbers of elderly people classified in each care grade between Shinjuku city and Japan using SPSS version 25 (IBM Corp., Armonk, NY, USA).
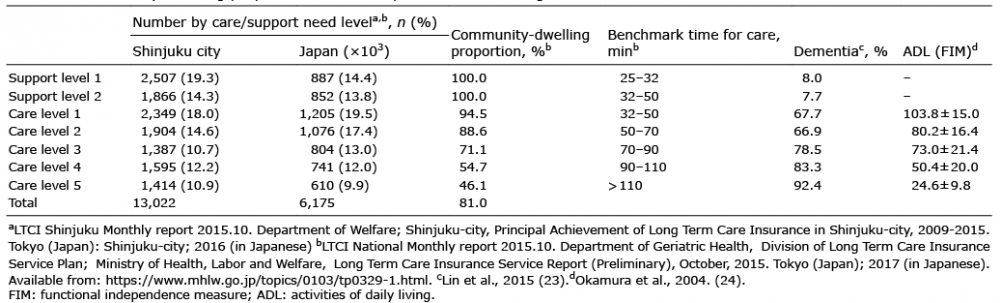
To clarify the characteristics of the study population, we compared the demographics of the LTCI-certified populations of Shinjuku city and Japan (Table I and Table SII1). Although Shinjuku had a relatively lower proportion of elderly residents (19.5% vs 26.2% nationally), it had a relatively higher proportion of residents certified recipients of care by the LTCI system (19.6% vs 17.7% nationally). A small, but statistically significant, difference in the distribution of care levels was observed between the study area and all of Japan (χ2 (df 6) = 361.1 (p < 0.001); Cramer’s V = 0.0073).
Table I. Community-dwelling proportion of care recipients in each care grade
Survey responses were received from 22 of 77 CM offices (28.6%). Representatives of all those 22 offices had attended the preparatory lecture. Data about special needs regarding food intake were acquired from 1,271 of the 10,790 total care recipients (11.8%) registered in Shinjuku (Table II). Of the community-dwelling elderly care recipients who participated in the study, 34.6% were reported to have some level of swallowing difficulty (A+B+C+D). Of these, 23.1% of community-dwelling elderly care recipients were found to have dysphagia (A+B+C), whereas 11.5% were a unique population identified for the first time by this study as people at potential risk of difficulty with ingesting emergency foods, despite being classified as without dysphagia in ordinary settings (D). After excluding the population not dependent on oral ingestion (A+B), 19.7% of the study population was considered at risk of aspiration when consuming regularly distributed emergency foods (C+D).
Table II. Profiles of swallowing problems among community-dwelling older people in need of care
To our knowledge, this is the first study to assess the adaptability of emergency foods for the community-dwelling, care-requiring, elderly population. This study revealed that approximately one-third of such elderly residents in Shinjuku city experienced some difficulties with swallowing. After excluding the non-orally-fed population, approximately one-fifth of community-dwelling elderly care recipients would be at risk of aspiration during the post-disaster period, and more than half of these would face a risk of aspiration solely attributable to the intake of common emergency foods. Using the same questionnaire, Kawashima et al. reported previously that 13.8% of the community-dwelling elderly population experienced dysphagia, regardless of their requirement for care (14).
It is notable that our study population was relatively similar to that in a study by Chen et al., which targeted residents of an urban independent-living senior facility. Although that earlier study involved only 4% of the population requiring substantial care, a questionnaire-based survey revealed that 23.4% of the participants had dysphagia (16). Although these studies cannot be unconditionally compared, the current results were consistent with those of Chen et al. Other studies of healthy community-dwelling populations have reported dysphagia prevalence rates of 11.4% among people older than 65 years (17) and 16.2% among those older than 87 years (18), suggesting that a potentially much larger number of otherwise healthy community-dwelling elderly people would be at risk of aspiration in a disaster setting. This is consistent with our findings, which were also obtained in a population of mostly healthy subjects (support levels 1 and 2).
The 19.7% of care recipients classified into classes C and D in our study would require a specific post-disaster food supply. Again, it is noteworthy that the population in class D could be considered as having normal swallowing function when consuming familiar foods in ordinary settings. These people accounted for 8.5%, 11.8% and 49.7% of care recipients in our simplified Low-, Middle-, and High-grade support/care level categories, respectively. However, it may not be practical to store very large amounts of pre-packaged, texture-modified foods, which tend to be costlier and have shorter expiration periods. Therefore, a critical social safeguard would require not only the storage, but also the supply, or even cooking, of adequate foods for this vulnerable population during post-disaster periods. Well-formulated strategies to achieve this safeguard have been outlined in the principles of “disaster food” (3, 10). It is also notable that both elderly individuals and their non-ordinary caregivers (including volunteers) are frequently overlooked when communicating the potential risks of consuming emergency foods (9). Disaster rehabilitation can play a pivotal role in raising public awareness about this issue.
Disaster rehabilitation (2) and feeding support teams (19) worldwide should better organize efforts to address the large population of elderly survivors with special food intake needs, including those at risk of aspiration solely when consuming regularly distributed emergency foods. Studies have reported the effects of disaster rehabilitation on improvements in physical function, post-traumatic stress disorder, quality of life, and re-employment among disaster victims with various disorders (20). Although, to our knowledge, no previous study has evaluated swallowing management during disasters, disaster evacuees with dysphagia may benefit from a multidisciplinary rehabilitative approach. Previous reports have suggested that oral care reduces the rate of pneumonia in vulnerable elderly populations (21), and home-based exercise has been shown to significantly reduce the incidence of aspiration pneumonia (22). Another report from a feeding support team discusses successful cases in which signs of aspiration were reduced by contriving a means of cooking emergency foods after a disaster (3). These aspects should be evaluated more systematically through structured studies, and preventive interventions should be enforced accordingly to reduce harm during future disasters.
This preliminary study had several limitations of note. First, although most elderly individuals with health issues are certified in the mandatory LTCI system, some people, such as individuals with dysphagia who consider themselves healthy, do not utilize this system. Secondly, nursing home residents were not included in the present study; therefore, the results do not reflect the entire elderly population. However, as nursing homes usually prepare sufficient stockpiles of appropriate foods for their residents, it may not be necessary to include this population from the standpoint of preventive medicine. However, both of these factors will additionally restrict the external validity of the findings from this cross-sectional survey. Thirdly, the survey response rates were relatively low among the CM offices (28.6%) and target population (11.8%). Although we do not have data on attrition at several levels, we speculate that a possible reason for the low response rate may be the lack of a sense of crisis. Despite this low response rate, the current study included a large number of participants (1,271 care recipients), and the findings are considered to be reasonably reliable. Future studies will require better strategies to improve the survey response rate, possibly including hand delivery and collection of the forms, an explanation of the specific method used at each office, detailed subsequent feedback, and an acknowledgement or monetary reward. Fourthly, because we lack exact demographic data about the sample, we cannot determine which groups of elderly people (e.g. females vs males) are at a particularly high risk of having special food intake needs in disaster settings. We recommend that a more detailed survey based on the LTCI system be conducted in the near future. Finally, although we estimated the number of elderly people corresponding to each status, a more focused study is needed to enable an analysis of personal and medical background data, including details of swallowing function and comorbidities.
In conclusion, the present survey revealed that a large proportion of community-dwelling elderly care recipients are at risk of aspiration pneumonia due to the consumption of emergency food in a disaster setting. Importantly, this population includes a subset of people who would be regarded as having normal swallowing function when consuming regular foods in an ordinary setting. Therefore, a proper assessment of food intake statuses in the elderly population is needed prior to making decisions about public food storage. There is an urgent need to educate healthcare professionals and the larger society about this issue and thus enhance preparedness by carefully considering this vulnerable population.
The authors appreciate the help of all the members of the Lincage-promotion committee of The Disaster Assistance Sub-project for Citizens Needing Home Medical Care in the Home Medical Care Promotion Project for Local Municipalities in the Tokyo Metropolitan Government and The Shinjuku-Gokkun project, Ms Eiko Hatano and all the members of the Caremanager Manager Network Shinjuku, and Dr Maiko Ohmori, Dr Yuko Kasashima-Shindo, Ms Makiko Ando and all the members of Department of Rehabilitation Medicine at Keio University School of Medicine and Department of Rehabilitation at Keio University Hospital. This work was supported by The Rehabilitation Support Center for the Western Part of Tokyo Metropolitan Government, and The Disaster Assistance Sub-project for Citizens Needing Home Medical Care in the Home Medical Care Promotion Project for Local Municipalities in the Tokyo Metropolitan Government.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize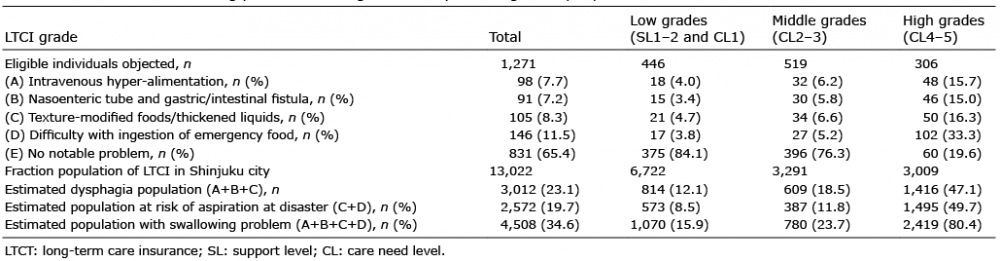 Click to show fullsize
Click to show fullsize