
From the 1Department of Epidemiology and Health Statistic, West China School of Public Health, and West China Fourth Hospital, Sichuan University, Chengdu, 2Department of Anorectal Surgery, Changhai Hospital of Shanghai, Shanghai, 3Department of Neurorehabilitation, Shanghai Second Rehabilitation Hospital, 4School of Rehabilitation Science, Shanghai University of Traditional Chinese Medicine, Shanghai, China.*Those authors contributed equally to this work.
Objective: To systematically synthesize and critically evaluate evidence on the effects of tai chi for patients with type 2 diabetes mellitus.
Data sources: Seven electronic databases (Wan Fang, SinoMed, China National Knowledge Infrastructure, VIP, PubMed, Embase, and Cochrane Library) were systematically searched from their inception to March 2018.
Study selection: Randomized controlled trials investigating the effects of tai chi on individuals with type 2 diabetes mellitus were eligible.
Data extraction: Biomedical outcomes (fasting plasma glucose, glycosylated haemoglobin (HbA1c), fasting insulin, insulin resistance, body mass index, total cholesterol, blood pressure) as well as balance and quality of life-related outcomes were extracted independently by 2 reviewers. Stata 12.0 software was used to synthesize data if there was no or moderate heterogeneity across studies. Otherwise, narrative summaries were performed.
Data synthesis: A total of 23 studies (25 articles) involving 1,235 patients were included in this meta-analysis. Significant changes in tai chi-related effects were observed in lowering fasting plasma glucose (standardized mean difference; SMD –0.67; 95% confidence interval (95% CI) –0.87 to –0.47; p < 0.001), HbA1c (mean difference; MD–0.88%; 95% CI –1.45% to –0.31%; p =0.002) and insulin resistance (MD –0.41; 95% CI –0.78 to –0.04; p = 0.029). Beneficial effects of tai chi were also found in decreasing body mass index (MD –0.82 kg/m2; 95% CI –1.28 to –0.37 kg/m2; p < 0.001) and total cholesterol (SMD –0.59; 95% CI –0.90 to –0.27; p < 0.001). In addition, tai chi reduced blood pressure (systolic blood pressure (MD –10.03 mmHg; 95% CI –15.78 to –4.29 mmHg; p = 0.001), diastolic blood pressure (MD –4.85 mmHg; 95% CI –8.23 to –1.47 mmHg; p = 0.005)) and improved quality of life-related outcomes (physical function (MD 7.07; 95% CI 0.79–13.35; p = 0.027), bodily pain (MD 4.30; 95% CI 0.83–7.77; p = 0.015) and social function (MD 13.84; 95% CI 6.22–21.47; p < 0.001)). However, no impact was exerted on fasting insulin (SMD –0.32; 95% CI –0.71 to 0.07; p = 0.110) or balance (MD 2.71 s; 95% CI –3.29 to 8.71 s; p = 0.376).
Conclusion: Tai chi is effective in controlling biomedical outcomes and improving quality of life-related outcomes in individuals with type 2 diabetes mellitus, although no effects were observed on balance and fasting insulin. Further high-quality research is needed to elucidate the effects of different types of tai chi, the long-term effects of tai chi, the impact on respiratory function, and the association between tai chi and the risk of developing type 2 diabetes mellitus in healthy individuals.
Key words: tai chi; type 2 diabetes mellitus; meta-analysis; systematic review.
Accepted Mar 22, 2019; Epub ahead of print Apr 10, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Rongsheng Luan, Department of Epidemiology and Health Statistic, West China School of Public Health, West China Fourth Hospital, Sichuan University, 17 Renminnan Road, Wuhou District, Chengdu, Sichuan 610041, China. E-mail: three_stones_SCU@163.com; Kunpeng Li, Department of Neurorehabilitation, Shanghai Second Rehabilitation Hospital, 25 Changjiang Road, Baoshan District, Shanghai 200441, China. E-mail: 929186865@qq.com
A review of research into the effects of tai chi for patients with type 2 diabetes mellitus was carried out. The results indicate that tai chi is favourable in improving outcomes in some areas, e.g. fasting plasma glucose, glycosylated haemoglobin (HbA1c), total cholesterol, balance, and quality of life. However, differences between study methods limit the conclusions regarding some outcomes. Tai chi might be a suitable complementary therapy for individuals with type 2 diabetes mellitus.
D
iabetes mellitus (DM) is a metabolic disturbance characterized by an increase in blood glucose levels due to insulin deficiency and/or resistance. During the past decades, there has been a sharp increase in the prevalence of DM worldwide (1). In 2003, the World Health Organization (WHO) predicted that the number of patients with diabetes would increase to 370 million by 2030 (2). DM is regarded as one of the major threats to public health (3). There are 2 main types of DM: type 1 diabetes mellitus (T1DM), caused by the destruction of pancreatic β-cells; and type 2 diabetes mellitus (T2DM) caused by insulin resistance or impaired insulin secretion. T2DM is the most prevalent form of diabetes, patients are more likely to usually develop diabetic ketoacidosis (4) and damage can occur to tiny blood vessels and nerves. For patients with T2DM, the duration of the disease influences the severity of diabetic neuropathy, increasing activity limitations (5). In addition, patients are more likely to develop cardiovascular and Alzheimer’s disease, as well as various cancers (1). T2DM is a chronic disease, exerting an adverse influence on the daily life of patients and imposing a burden on their finances. Therefore, great emphasis should be placed on disease nursing for patients with diabetes.
Tai chi (also known as tai ji or tai chi quan), originating from ancient China, is a mind-body exercise characterized by mild or moderate aerobic activity. It is also an effective muscle strength training for the upper and lower extremities. Tai chi is currently often recognized as a physical fitness technique in our society, especially for middle-aged or elderly people (6). There are several styles of tai chi; Yang, Chen, Sun and Wu styles are commonly practiced in daily life, and the Yang style is the most popular among the public, while the Chen style is viewed as the oldest (7). The Yang style is typical of its concise movement, while the Wu style is more notable for gentle action. Movement in the Chen style varies during the whole process, while the Sun style is well known for coherence (8). However, different types of tai chi have a common method. All of the styles involve continuous, gentle and slow movements involving balance, strengthening, breath control, mental concentration and relaxation (9). Tai chi can therefore play a role in both physical and mental rehabilitation. Some studies have suggested that tai chi has favourable effects on a variety of factors, including cardiovascular protection (10), fall prevention (11), balance (12), flexibility (13), depression (14) and quality of life (QoL) (15). Tai chi has potential benefits in treating different diseases, including chronic obstructive pulmonary disease (16), Parkinson’s disease (17), osteoarthritis (18) and stroke (19). Thus, tai chi may be a suitable exercise for individuals with chronic diseases (9, 20).
Compared with pharmacological therapy, tai chi is an economical treatment, and can be performed wherever convenient, and is less likely to result in adverse effects (21). As a mind-body exercise, tai chi may have effects on both physical and mental well-being. Individuals who perform tai chi are reported to tend to have better psychological health (7). Given the above strengths, tai chi may be a suitable complementary treatment for patients with T2DM; thus it is critical to elucidate its effects on such patients. Although some systematic reviews (22–25) have been performed to evaluate the effectiveness of tai chi for patients with T2DM, no definite conclusions have been drawn. First, discrepancies existed in the conclusions of those reviews. Lee et al. (22), Yan et al. (23) and Lee et al. (24) reported that tai chi did not reduce fasting plasma glucose (FPG), glycosylated haemoglobin (HbA1c), or insulin resistance (IR), and they did not find that tai chi was an effective rehabilitation therapy for T2DM. On the other hand, Huang & Yeh (25) indicated that tai chi was effective in improving HbA1c and FPG. Furthermore, it is inappropriate for some reviews (23, 24) to combine data from studies with different designs or methods, as this might lead to high heterogeneity. In addition, since these reviews were published a long time ago, the evidence should be updated.
For some patients with T2DM, the main pathological change is IR, which in turn contributes to the high concentration of fasting insulin (FIN) in peripheral blood. Therefore, FIN may be regarded as a medical indicator reflecting IR to a certain degree. Patients with T2DM are more vulnerable to diabetic neuropathy, foot ulceration and nerve damage due to infection (26). Postural instability, which is common in diabetic sensory neuropathy, could increase the risk of minor foot trauma (27). Improvement in stability is a prerequisite for normal physical activity. Moreover, patients with T2DM are under great pressure to treat themselves, and they usually have lower QoL compared with healthy individuals (28). QoL is one of the comprehensive indicators for evaluating self-management of disease and therapeutic effects, and thus QoL may be an appropriate target for treatments in patients with T2DM. However, whether tai chi training could improve these outcomes remains controversial, and no relevant content was reported in the above reviews.
The objective of this review was therefore to synthesize and critically evaluate the published evidence on the effects of tai chi on FPG, HbA1c, IR, FIN, body mass index (BMI), total cholesterol (TC), blood pressure (BP), balance and QoL among individuals with T2DM.
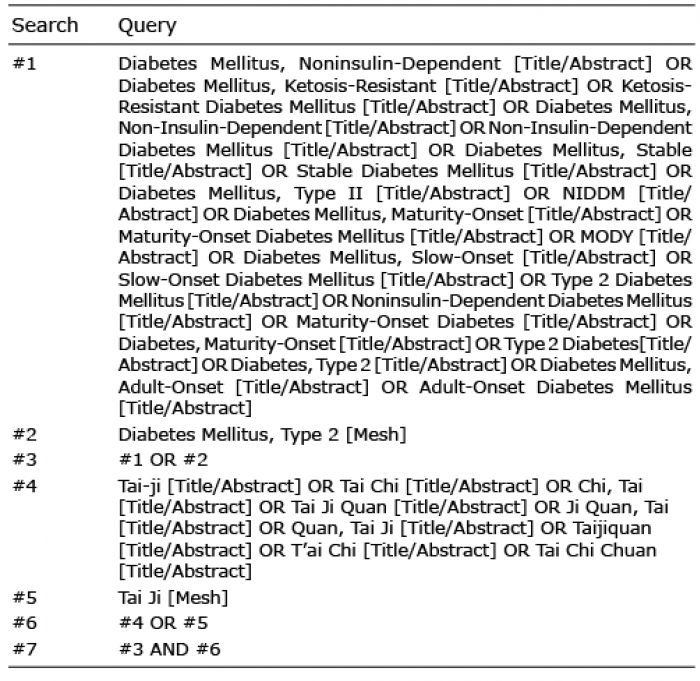
Seven electronic databases (Wan Fang, SinoMed, China National Knowledge Infrastructure, VIP, PubMed, Embase, and Cochrane Library) were searched for eligible publications from their inception to March 2018. The following search terms were used: “tai ji”, “tai ji quan”, “tai chi”, “tai chi chuan”, “type 2 diabetes mellitus”, “noninsulin-dependent diabetes”, “maturity-onset diabetes”. Variations and synonyms of these search terms were used in order to perform an overall and systematic search. In addition, the reference lists of all related literature were reviewed to identify potentially eligible studies. The detailed search strategy for PubMed is shown in Table I.
Table I. Search strategy for PubMed
Titles and abstracts of retrieved literature were independently screened by 2 reviewers (ZL. Z and RZ. Z) according to pre-defined eligibility criteria. Full-text reading was performed for studies whose relevance could not be determined from their titles and abstracts. During study selection, discrepancies were discussed until consensus was reached.
More specifically, included studies had the following features (PICOS criteria: Participants, Interventions, Comparisons, Outcomes, Study design).
Patients diagnosed with T2DM age > 18 years.
Only randomized controlled trials (RCTs) published in Chinese or English were included in this meta-analysis. Systematic reviews, meta-analyses or reference papers were excluded. Studies were also excluded if outcome data were not available even though attempts were made to contact the authors.
Tai chi, regardless of type, must be performed by participants in the intervention group of included studies. Studies were excluded if the intervention was tai chi combined with other treatments. No restriction was imposed on location (community/hospital, outdoors/indoors), format (group/individual), intensity, frequency or duration of treatment.
The control group received “usual care or exercise”, “sham exercise”, or “no intervention”. All the conditions except the treatment of intervention group should be comparable with those of control group.
FPG, HbA1c, FIN, IR, BMI, TC, systolic blood pressure (SBP) and diastolic blood pressure (DBP) were used to evaluate the effects of tai chi on biomedical outcomes. Among these indicators, IR should be evaluated by homeostasis model assessment (HOMA) version 1 or 2. In addition, QoL and balance (measured with the 36-item Short-Form (SF-36) scale (29) and duration of single-leg stance, respectively) as well as BMI, were assessed.
Data were independently extracted by 2 reviewers (ZL. Z and Y. Z) according to a pre-specified data extraction table, which comprised the following items: first author, publication year, region, sample size, characteristics of participants (disease status, age, FPG at baseline, disease duration). Outcomes at baseline and follow-up were also recorded. Data on intervention regimens, including type of tai chi, training time, frequency and duration, were extracted. A mutual check on extracted data was performed by 2 reviewers. Disputes and disagreements were solved by discussion or referral to a third reviewer (KP. L).
Two reviewers (ZL. Z and RZ. Z) independently assessed the risk of bias in individual studies by using the Physiotherapy Evidence Database (PEDro) scale (30), which was commonly used to judge the quality of RCTs regarding physical therapy. Studies with a PEDro score over 4 points were regarded as high quality. Any discrepancies were resolved through discussion. If consensus was not reached, a third reviewer (RS. L)was consulted.
Pooled analyses were performed using Stata 12.0 software. Mean changes from baseline to follow-up were synthesized for continuous data, and 3 aspects of QoL were evaluated: physical function, bodily pain and social function. Mean difference (MD) or standardized mean difference (SMD) with 95% confidence interval (95% CI) were summarized for continuous outcomes evaluated, respectively, by identical measurement or different measurements. Heterogeneity across studies was assessed by I2 statistic. A fixed-effects pooled analysis was conducted if no or low heterogeneity (I2< 50%) existed, and when there was high heterogeneity among studies (I2> 50%), a random-effects meta-analysis was performed. Sensitivity analysis was performed to explore the impact of methodological quality of included studies on results by removing low-quality studies (PEDro score ≤4). In addition, data were synthesized after excluding studies in turn to test the stability of results, if necessary. Funnel plot and Egger’s test (31) were used to assess the possibility of publication bias, if appropriate.
A total of 487 articles were retrieved according to the search strategy, and no articles were obtained from other sources (Fig. 1). A total of 292 articles remained after removing duplicates. After removal of irrelevant articles through titles and abstracts, full-text reading of 50 articles was performed for further assessment. Of these, 25 articles were excluded for various reasons (see Fig. 1). Therefore, a final total of 23 studies reported in 25 articles (32–56) were included in this systematic review and meta-analysis.
Fig. 1. Flow chart of study selection. T2MD: type 2 diabetes mellitus; RCT: randomized controlled trial.
One RCT reported in 3 articles (49–51) was regarded as a study, which together with another study (48) originated from Australia (Table II). One of 23 studies originated from South Korea (43), one was conducted in Thailand (42) and the rest in China. The sample size ranged from 16 to 200, and mean age ranged from 35.6 to 69.5 years. The average duriation of disease a ranged from 1 to 23 years, and the mean HbA1c before treatment from 6.9% to 11.9%. Four studies (33, 34, 36, 38) applied Chen style tai chi, and one (34) applied Yang style tai chi. A simplified style was used in 5 studies (45–47, 55, 56). Sun style and Yang style tai chi was used in 2 studies (4 articles) (48–51), Lin style was used in 1 study (42), and Da-yuan-jiang-tang style was used in 1 study (54). The mean time per session ranged from 15 to 120 min, mean intervention frequency from 2 to 14 sessions per week, and the mean duration of the intervention from 4 to 24 weeks.
Table II. Basic characteristics of included studies.
The majority of studies reported inclusion criteria, except for 2 studies (38, 55). The treatment group and the control group were comparable at baseline for all studies, and point estimates and variability were all reported. All studies except 4 (32, 36, 43, 56) were considered high quality. The risk of bias assessment is shown in Table III.
Table III. Assessment of bias risk in individual study
Fasting plasma glucose. A total of 21 studies (32–45, 47, 51–56) evaluated the effects of tai chi on FPG. With high heterogeneity across studies, a random-effects pooled analysis was performed to synthesize the data. The results indicated that tai chi was potentially effective in reducing FPG (SMD –0.67; 95% CI –0.87 to –0.47; p < 0.001; heterogeneity, I2 = 53.2%, p = 0.001; Fig. 2).
Fig. 2. Forest plot of the effects of tai chi on fasting plasma glucose. StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; SMD: standardized mean difference; 95% CI: 95% confidence interval.
Glycosylated haemoglobin (HbA1c). A total of 14 studies (35, 36–43, 45, 48, 49, 52–54) compared the effects of tai chi on HbA1c with a control group. Meta-analysis showed that tai chi was beneficial in lowering HbA1c (MD –0.88; 95% CI –1.45% to –0.31%; p = 0.002; heterogeneity, I2 = 97.8%, p < 0.001; Fig. 3A). Sensitivity analysis showed that 2 studies (37, 45) exerted great influence on the stability of synthesized results. The results after excluding these 2 studies also indicated that tai chi was effective in decreasing HbA1c (MD –0.53; 95% CI –0.62% to –0.44%; p < 0.001; heterogeneity, I2 = 43.4%, p = 0.033; Fig. 3B).
Fig. 3. Forest plot of the effects of tai chi on glycosylated haemoglobin. (A) All included studies; (B) all studies except for Bao’s and Wu’s research; StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; WMD: weighted mean difference; 95% CI: 95% confidence interval.
Fasting insulin. Eight studies (33, 38, 41, 45, 47, 52, 53, 55) evaluated the impact of tai chi on FIN. The pooled analysis suggested that tai chi failed to show favourable influence on FIN (SMD –0.32; 95% CI –0.71 to 0.07; p = 0.110; heterogeneity, I2 = 73.3%, p < 0.001; Fig. 4).
Fig. 4. Forest plot of the effects of tai chi on fasting insulin. StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; SMD: standardized mean difference; 95% CI: 95% confidence interval.
Insulin resistance. The effects of tai chi on IR measured by HOMA were reported in 5 studies (33, 35, 41, 48, 49). A fixed-effects pooled analysis showed favourable effects of tai chi on reducing IR (MD –0.41; 95% CI –0.78 to –0.04; p = 0.029; heterogeneity I2 = 0.0%, p = 0.5; Fig. 5).
Fig. 5. Forest plot of the effects of tai chi on insulin resistance. StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; WMD: weighted mean difference; 95% CI: 95% confidence interval.
Total cholesterol. Ten studies (32, 33, 35, 37, 38, 41, 47, 48, 52, 55) evaluated the effects of tai chi on TC. A random-effects pooled analysis demonstrated positive effects of tai chi on decreasing TC (SMD –0.59; 95% CI –0.90 to –0.27; p < 0.001; heterogeneity, I2 = 66.6%, p = 0.001; Fig. 6).
Fig. 6. Forest plot of the effects of tai chi on total cholesterol. StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; SMD: standardized mean difference; 95% CI: 95% confidence interval.
Body mass index. Seven studies (33, 37, 38, 42, 49, 55, 56) compared the effects of tai chi on BMI with control group. A fixed-effects pooled analysis indicated that there was a statistically significant reduction in BMI (MD –0.82 kg/m2; 95% CI –1.28 to –0.37 kg/m2; p < 0.001; heterogeneity, I2 = 26.3%, p = 0.228; Fig. 7A).
Balance. Two studies (43, 50) comprising 3 intervention groups evaluated the effects of tai chi on balance according to the duration of single-leg stance. A random-effects pooled analysis revealed no effects of tai chi on increasing the duration of single-leg stance (MD 2.71s; 95% CI –3.29 to 8.71 s; p = 0.376; heterogeneity, I2 = 63.8%, p = 0.063; Fig. 7B).
Fig. 7. Forest plot of the effects of tai chi on: (A) body mass index; (B) balance. StudyID:study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; WMD: weighted mean difference; 95% CI: 95% confidence interval.
Blood pressure. Five studies (38, 42, 45, 48, 53) compared the effects of tai chi on BMI with a control group. The results of meta-analysis indicated there was a statistically significant reduction in SBP (MD –10.03 mmHg; 95% CI –15.78 to –4.29 mmHg; p = 0.001; heterogeneity, I2 = 55.4%, p = 0.062; Fig. 8A) and DBP (MD –4.85 mmHg; 95% CI –8.23 to –1.47 mmHg; p = 0.005; heterogeneity, I2 = 33.1%, p = 0.201; Fig. 8B).
Fig. 8. Forest plot of the effects of tai chi on blood pressure. (A) systolic blood pressure; (B) diastolic blood pressure; StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; WMD: weighted mean difference; 95% CI: 95% confidence interval.
Quality of life. Five studies (41, 43, 45, 46, 48) compared the effects of tai chi on QoL with a control group. A pooled analysis suggested that tai chi improved physical function (MD 7.07; 95% CI 0.79–13.35; p = 0.027; heterogeneity, I2 = 79.6%, p = 0.001; Fig. 9A), bodily pain (MD 4.30; 95% CI 0.83–7.77; p = 0.015; heterogeneity, I2 = 39.2%, p = 0.160; Fig. 9B) and social function (MD 13.84; 95% CI 6.22––21.47; p < 0.001; heterogeneity, I2 = 86.0%, p = 0.063; Fig. 9C).
Fig. 9. Forest plot of the effects of tai chi on quality of life. (A) Physical function; (B) bodily pain; (C) social function; StudyID: study reference; Tn: number of participants in treatment group; Cn: number of participants in control group; WMD: weighted mean difference; 95% CI: 95% confidence interval.
The results of funnel plot (Fig. 10) and Egger’s test (t = –1.93, p = 0.064) suggested there was no publication bias across studies. Sensitivity analysis revealed that tai chi potentially had beneficial effects in reducing FPG (SMD –0.62; 95% CI –0.84 to –0.39; p < 0.001), decreasing HbA1c (MD –0.89%; 95% CI –1.49% to –0.29%; p = 0.003), lowering BMI (MD –0.83 kg/m2; 95% CI –1.30 to –0.37 kg/m2; p = 0.001; heterogeneity, I2 = 38.1%, p = 0.152) and TC (SMD –0.45; 95% CI –0.67 to –0.24; p < 0.001) as well as improving social function (MD 11.92; 95% CI 4.02–19.83; p = 0.003). However, there was no effect on balance (MD –0.63 s; 95% CI –3.29 to 8.71 s; p = 0.563), physical function (MD 6.33; 95% CI –0.67 to 13.34; p = 0.076) or bodily pain (MD 3.44; 95% CI –0.11 to 6.99; p = 0.058).
Fig. 10. Funnel plot of publication bias. SMD: standardized mean difference; se(SMD): standard error of standardized mean difference.
The aim of this systematic review was to evaluate the effects of tai chi in patients with T2DM. The review was performed following the procedures recommended by the Cochrane Handbook (57). The results indicate that tai chi has beneficial effects on controlling some biomedical outcomes (FPG, HbA1c, IR, BMI, TC, BP) and QoL-related outcomes (physical function, bodily pain, and social support), but did not improve FIN and balance.
A total of 23 studies (26 articles) were included in this meta-analysis, and no publication bias existed. In this systematic review, tai chi was found to be effective in lowering FPG (SMD –0.67; 95% CI –0.87 to –0.47; p<0.001) and HbA1c (MD –0.88%; 95% CI –1.45% to –0.31%; p = 0.002). Compared with usual treatments, tai chi could reduce HbA1c by 0.88%. Previous study found tai chi could contribute to increased CD4+/CD25+ T-lymphocytes, and the latter was related to the decrease in HbA1c (58). Consistent with our findings, Huang & Yeh (25) also suggested favourable effects of tai chi in decreasing FPG and HbA1c. Due to high heterogeneity of HbA1c across studies, the stability of the results was tested by excluding included studies in turn to detect the sources. Analysis showed that 2 studies (37, 45) carried huge weight in the stability of results. Detailed analyses were performed, in which remarkable differences were found in the intervention regimens between these 2 studies and the others. In Bao’s study (37) the duration of intervention was up to 24 weeks, with a frequency of 14 sessions per week and 2 h per session, which was the longest among included studies. Similarly, in Wu’s study (45) the shortest session was over 1 h, with at least 3 sessions per week; thus it is impossible to specify the total time of practicing tai chi. It was therefore assumed that the total time of treatment might be the main source of heterogeneity.
Further analyses found favourable effects of tai chi, in reducing IR (MD –0.41; 95% CI –0.78 to –0.04; p = 0.029), TC (SMD –0.59; 95% CI –0.90 to –0.27; p < 0.001) and BMI (MD –0.82 kg/m2; 95% CI –1.28 to –0.37 kg/m2; p < 0.001). The relatively small magnitude of the above outcomes may be due to the short duration of intervention (59). Tai chi also decreased BP (SBP (MD –10.03 mmHg; 95% CI –15.78 to –4.29 mmHg; p = 0.001) and DBP (MD –4.85mmHg; 95% CI –8.23 to –1.47 mmHg improved; p = 0.005)), QoL (physical function (MD 7.07; 95% CI 0.79–13.35; p = 0.027) decreased, bodily pain (MD 4.30; 95% CI 0.83–7.77; p = 0.015) and increased social function (MD 13.84; 95% CI 6.22–21.47; p < 0.001)). Thus, tai chi was more efficient in improving BP and QoL-related outcomes compared with usual care of treatments, which is in agreement with the results of a previous study (60). A beneficial trend was also observed in reducing FIN (SMD –0.32; 95% CI –0.71 to 0.07; p = 0.110) and improving balance (MD 2.71s; 95% CI –3.29 to 8.71 s; p = 0.376), although no significant difference was achieved. One important reason for the insignificant effects of tai chi on FIN was heterogeneity. Included studies varied in sample size, population, types of tai chi, intervention regimens and study design. In addition, allocation concealment and blinding were not clear or applied in the majority of included studies, which might give rise to the bias. The results of the current review are consistent with a previous study of balance (61). When practicing tai chi, patients need to control their body balance while continuously changing position and bodily center of gravity. In addition, tai chi helps improve the ability of controlling muscles and joints, which is associated with better balance control (62). Moreover, the results of sensitivity analysis based on the PEDro scale score were consistent with the previous findings, except for physical function and bodily pain, which might be due to insufficient eligible studies. The contrary findings indicated the results of these two outcomes were unstable, which should be taken into consideration when interpreting our concludions.
There are several theories that could account for the effects of tai chi. Chen et al. (63) reported the main beneficial effects of tai chi are to enhance metabolism, anti-inflammatory activation and cardiopulmonary regulation, rather than consume calories. DM was also regarded as an inflammatory disease (27), and previous studies have found that tai chi is beneficial for regulatory T-cell function (64) and the reaction of type 1 helper (Th1) cells (27). As a type of moderate exercise, tai chi could improve basic metabolism and it has been shown to be beneficial for glucose absorption and glycogen synthesis, which in turn benefits glycaemic control (65). Furthermore, the bioactivity of insulin receptors on cytomembrane was also enhanced through tai chi (53).
In view of the beneficial effects of tai chi on many outcomes, we recommend that patients with T2DM should practice tai chi as a complementary rehabilitation therapy, especially those patients who also have obesity or hypertension. Considering that the effects of single aerobic exercise last less than 72 h (59), we also suggest that patients should practice tai chi at least 3 times per week.
This review has several limitations. First, some studies fulfilling the inclusion criteria might not have been included in the meta-analysis. Unpublished articles, such as grey literature, were not attainable despite the exhaustive search strategy. In addition, there was a possibility of language bias, since only English and Chinese literature was searched. Furthermore, the baseline information in some studies was incomplete, which might result in difficulty in performing further analysis, with misleading results. In addition, there was heterogeneity in several results due to different intervention regimens, baseline characteristics of patients, and duration of follow-up. The heterogeneity across studies and insufficient sample size might weaken the strenght of our conclusions for some outcomes; thus, there is a need for multi-centre, high-quality RCTs to further investigate the effects of tai chi on T2DM.
The current review also provides additional information for further study in related topics. First, tai chi could be categorized into many types (e.g. Chen style, Yang style, etc.) but insufficient evidence regarding differing effects of different types of tai chi makes it difficult to determine which style of tai chi should be practiced. Secondly, since the longest follow-up duration studied was 24 weeks, it is impossible to observe the long-term effects of tai chi. Thirdly, one needs to control breath when performing tai chi, and this indicates that tai chi might be associated with respiratory function, although most studies did not explore the related outcomes. Other outcomes, such as immune function, nerve modulation, and survival time, were rarely investigated in these studies. Lastly, most previous studies focus on the therapeutic effects of tai chi on T2DM, but whether performing tai chi could reduce the risk of T2DM in healthy individuals remains unclear. For the reasons described above, further research is suggested to investigate the effects of various styles of tai chi, the long-term effects of tai chi, the impact on the above outcomes, and the association between tai chi training and risk of developing T2DM
In conclusion, tai chi may be a suitable mind-body therapy for individuals with T2DM, since it is beneficial in reducing FPG, decreasing HbA1c and improving a variety of other outcomes.
The authors are grateful to the authors of the primary studies and acknowledge the assistance provided by Maowen Li with statistical analysis.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize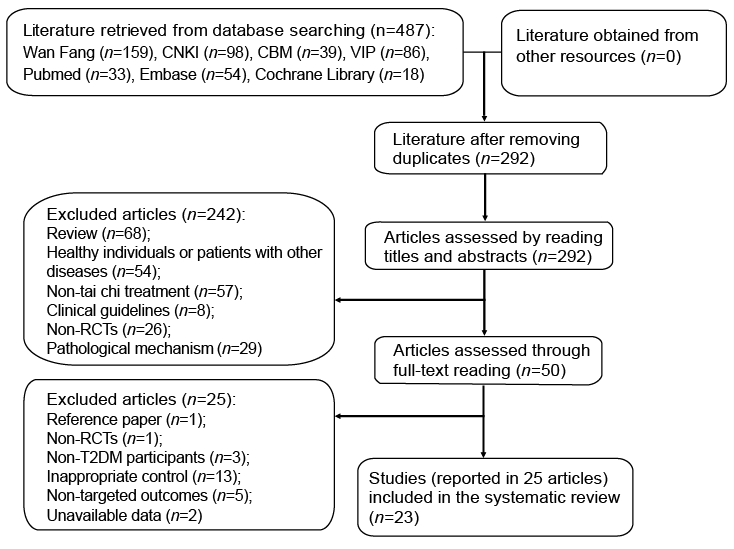 Click to show fullsize
Click to show fullsize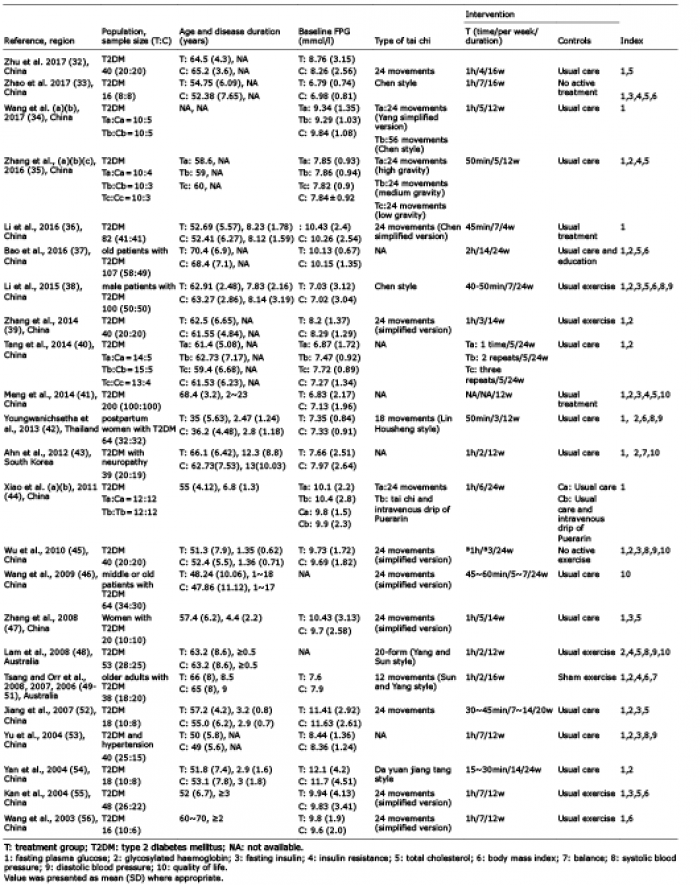 Click to show fullsize
Click to show fullsize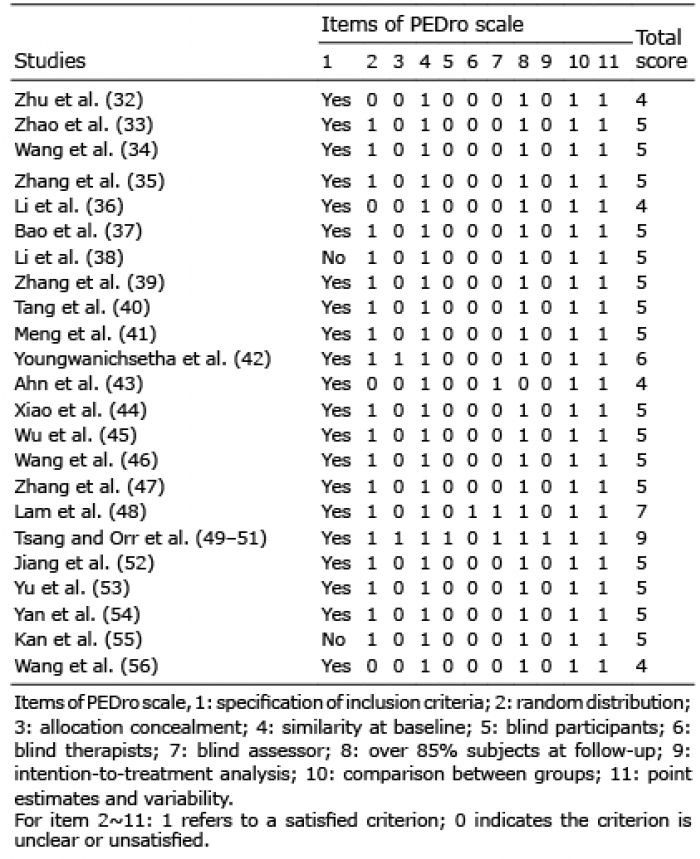 Click to show fullsize
Click to show fullsize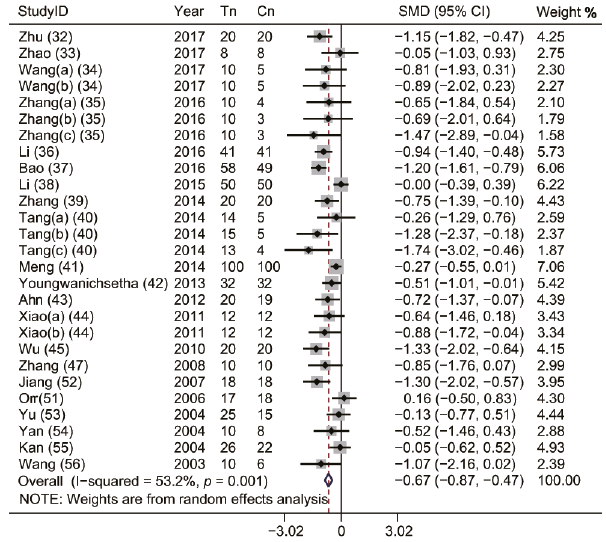 Click to show fullsize
Click to show fullsize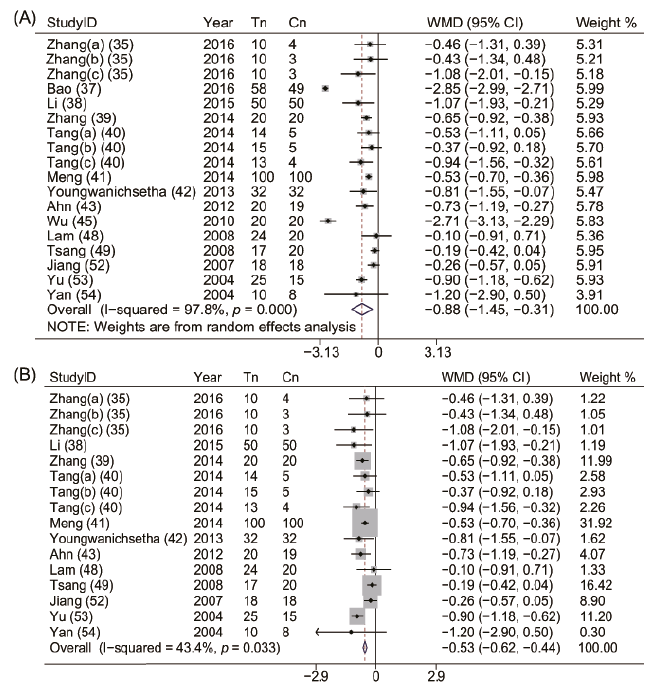 Click to show fullsize
Click to show fullsize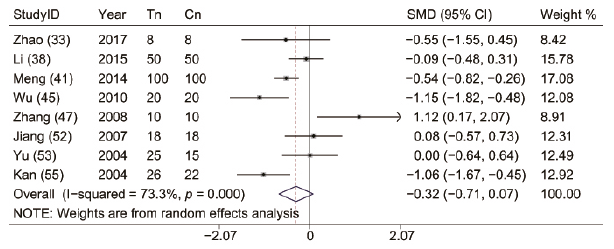 Click to show fullsize
Click to show fullsize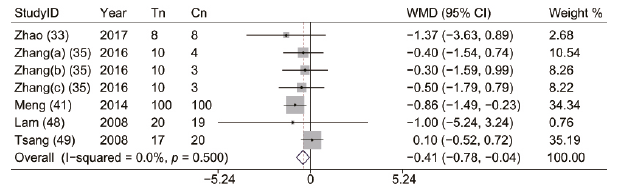 Click to show fullsize
Click to show fullsize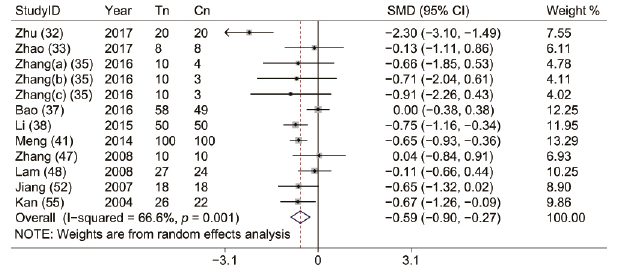 Click to show fullsize
Click to show fullsize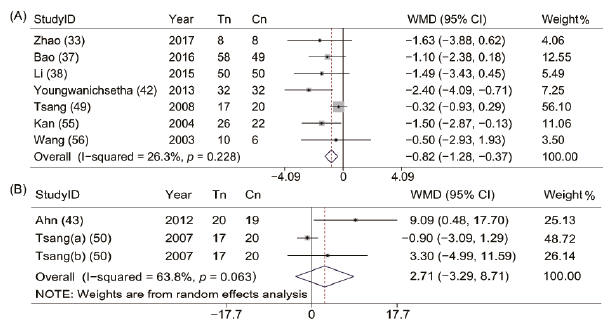 Click to show fullsize
Click to show fullsize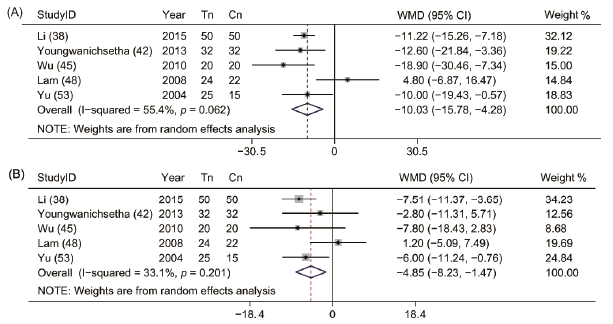 Click to show fullsize
Click to show fullsize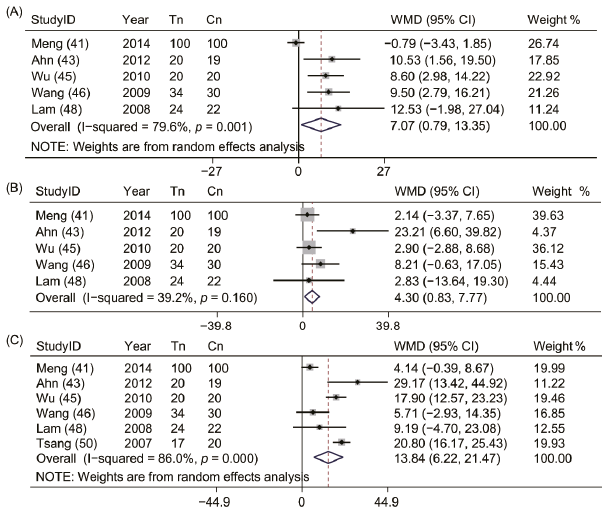 Click to show fullsize
Click to show fullsize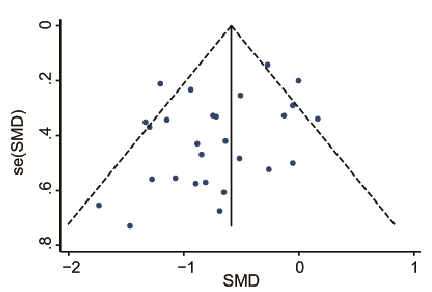 Click to show fullsize
Click to show fullsize