
From the Department of Clinical Neuroscience, Rehabilitation Medicine, Institute of Neuroscience and Physiology, Sahlgrenska, Academy, University of Gothenburg, Gothenburg, Sweden
Objective: To investigate different aspects of self-perceived impact of stroke 1 and 5 years after stroke onset, with a focus on self-perceived participation.
Design: Longitudinal cohort study.
Participants: Forty-five persons diagnosed with first-time stroke included in the Stroke Arm Longitudinal study at University of Gothenburg (SALGOT).
Methods: Participants responded to the Stroke Impact Scale, the Impact on Participation and Autonomy and the European Quality of Life 5 dimensions at 1 year and 5 years post-stroke. Wilcoxon signed-rank test was used to check for differences in changes over time between groups.
Results: In general, the perceived consequences of stroke were more severe after 5 years compared with at 1 year. Strength, emotion and participation were the areas most affected, along with restrictions in social life and autonomy indoors. Global disability (mRS) was moderately correlated with quality of life.
Conclusion: The perceived impact of stroke becomes more prominent with time, even for persons with mild-to-moderate stroke. This study highlights the need for long-term support for persons with stroke.
Key words: stroke; Stroke Impact Scale; longitudinal; participation.
Accepted Aug 21, 2019; Epub ahead of print Sep 2, 2019
J Rehabil Med 2019; 51: 660–664
Correspondence address: Katharina S. Sunnerhagen, Department of Clinical Neuroscience, Rehabilitation Medicine, Institute of Neuroscience and Physiology, Sahlgrenska, Academy, University of Gothenburg, Gothenburg, Sweden. E-mail: katharina.sunnerhagen@neuro.gu.se
Stroke is a major cause of death and disability world-wide. Persons with stroke experience many types of consequences. This study investigated the self-perceived consequences of stroke at 1 and 5 years post-stroke. Forty-five people participated in face-to-face interviews at 1 year and responded to surveys via regular mail after
5 years. The results show that the perceived impact of stroke becomes more severe with time, even for persons with mild-to-moderate stroke. We conclude that persons with stroke are in need of continuous support.
Stroke is a major cause of death and disability worldwide. More than 10 million people are affected by stroke every year (1). The majority of persons with stroke survive and, globally at least, 25 million people live with the consequences of stroke (1). In Sweden stroke affects approximately 25,000 persons every year and is the most common cause of neurological disability (2).
The consequences of stroke may impact various aspects of a person’s life. For example, reduced ability to manage activities of daily living (ADL), participation in society, or return to work or social life (3). Participation is defined by the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) as “involvement in life situation” (4). Previous research has shown that persons with stroke experience restriction in participation even after 5 years (5). A review study based on interview studies (6) found that rehabilitation did not focus sufficiently on psychological support after stroke to reduce experienced loneliness, but rather placed too much focus on functional rehabilitation (6). Some of the most frequent self-reported persisting consequences in a 10-year follow-up study were mobility, anxiety/depression, and pain/discomfort (7). The Stroke Impact Scale (SIS) is a questionnaire developed to evaluate not only the physical, but also other aspects important to how persons with stroke perceive their life after stroke (8). Most follow-up studies using SIS do not use it more than 1 year after stroke, but a Swedish study (9) investigated the self-perceived impact measured by the SIS after 6 years. The most positive clinical meaningful changes between 1 and 6 years were found in the domain participation. Those with moderate/severe stroke and older age experienced more negative clinically meaningful changes in different domains. However, even those that only had mild stroke still experienced consequences after 6 years (9).
To our knowledge not many studies have investigated the self-perceived impact of stroke using the same questionnaires and comparing them at 1 year and 5 years after stroke. The aim of the current study was to investigate different aspects of self-perceived impact of stroke 1 and 5 years after stroke onset, with a focus on participation.
This longitudinal cohort study is based on data from the Stroke Arm Longitudinal study at University of Gothenburg (SALGOT) and the SALGOT extended study (10, 11). The SALGOT study included all patients with first clinical stroke at Sahlgrenska University Hospital in Gothenburg, Sweden during 18 months in 2009–10. Inclusion criteria were: first-ever stroke based on World Health Organization (WHO) criteria, International Classification of Disease (ICD) codes, ischaemic stroke (I63) and haemorrhagic stroke (I61); living in the Gothenburg urban area (within 35 km of the hospital); age 18 years or older; able to communicate in Swedish prior to the stroke; and impaired arm function on day 3. Exclusion criteria were: impaired arm function prior to stroke onset; short life expectancy; and not able to communicate in Swedish prior to the stroke. In the SALGOT the participant were assessed on 8 occasions during the first year post-stroke. A set of questionnaires were sent out 5 years later to the surviving participants. Participants in the present study should have participated in the 1-year follow-up in the SALGOT study, as well as responded to the 5-year follow-up survey. The STROBE guidelines for observational studies were followed.
Clinical characteristics from stroke onset were obtained from medical charts. This includes National Institute of Health Stroke Scale (NIHSS) at admittance, the modified Rankin Scale (mRS, 0 = no symptoms, 5 = severe dependency) at discharge from hospital, which measures dependence in the daily activities after stroke and can be seen as a measure of stroke severity (12). The Charlson Comorbidity Index (CCI) (13) is a grading system in which various factors of a patient give different amounts of points depending on age and severity of a disease or syndrome. For comorbidity, the CCI is used, based on data from medical charts from the time at the stroke unit. The set of questionnaires included the Stroke Impact Scale (SIS) (8), the Impact on Participation and Autonomy (IPA) (14) and the European Quality of Life 5 dimensions (EQ-5D) (15). The responses were gathered by a face-to-face interview at 1-year post-stroke and by regular mail 5 years post-stroke.
The SIS is a multidimensional self-report questionnaire that evaluates the impact of stroke from the participant’s perspective, using 59 questions across 8 dimensions; strength, memory and thinking, emotion, communication, ADL, mobility, hand function, and participation (16). The questions within each dimension are scored 1–5, where 5 is best (least problems). The scores of each dimension are then converted into a value 0–100, where a score of 100 indicates no problems.
The IPA is a questionnaire with 5 different subscales; autonomy indoors, family role, autonomy outdoors, social life and relationships, and work and education. In total, the questionnaire consists of 32 questions or items (14). The questions pertaining to work and education are answered only for those who are in paid or voluntary work or for those who wish to enter further education. If not of working age the “not applicable” option could be used. Each question has a scoring range from 0 to 4, where 0 is very good and 4 is very poor. In order for a subscale to be valid, a minimum of 75% of the questions must be completed.
The EQ-5D is a questionnaire that measures general health status across 5 dimensions: mobility, self-care, common activities, pain/discomfort, and anxiety/depression. For each domain there are 3 grades: no problems, moderate problems, or severe problems (15).
Statistical methods
The data were processed and analysed in IBM Statistical Package for Social Sciences (SPSS) version 22 for Windows. p < 0.05 is considered statistically significant in the present study. Drop-out analysis was performed with regards to age, sex, stroke severity (NIHSS at admittance) and global disability at discharge according to mRS. The drop-out analysis was performed with χ2 test regarding sex and mRS and by Mann–Whitney U test for NIHSS and age. Wilcoxon signed-rank test was used to check for statistically significant differences over time between 2 related samples (16). Correlations were analysed by Spearman rank correlation, and correlations less than 0.3 are considered weak, between 0.3 and 0.5 moderate, and >0.5 strong (17).
Ethical considerations
The Regional Ethical Review Board approved the study: Dnr 225-8 with a complementary approval T801-10, as well as Dnr 400-13. All participants gave informed oral and written consent.
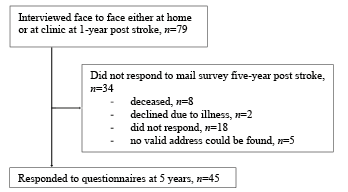
Seventy-nine persons participated at the 1-year follow-up, of whom 45 participated at the 5-year follow-up, and were included in the present study (Fig. 1). The number of participants that have answered the questionnaire within each assessment varies. The mean age at stroke onset was 63.8 years and the majority of participants were men (Table I). There were no significant differences regarding sex (p = 0.116) or age (p =0.800) between the non-responders (n = 34) and responders at 5 years (n = 45). The median NIHSS at admittance for the whole group was 7, and the difference between responders and non-responders was not significant. However, the non-responders had a higher mRS at discharge (p < 0.0001). Only 3 participants reported having had a new stroke during the 5-year follow up.
Fig. 1. Flow chart of the population selection procedure starting at year 1 post-stroke with inclusion at 5 years.
Table I. Clinical characteristics of the population, n = 45
Self-perceived impact measured by the SIS was more prominent after 5 years compared with 1-year post-stroke, as can be seen in Table II in 5 out of 8 dimensions. After 5 years, emotion, strength and participation were the dimensions with the most experienced problems. The dimensions assessed as the most impacted at 1 year were hand function and participation, but at 5 years emotion, strength and participation were the dimensions for which participants experienced the most problems.
Table II. Self-perceived impact of stroke according to Stroke Impact Scale after 1 and after 5 years. Differences in change over time were analysed by Wilcoxon signed-rank test
Autonomy indoors includes looking after oneself as one wants and getting around the house when and where one wants. At 1 year, the participants scored very good for the indoors subscale. For all the other subscales the median was 1, meaning good. Also at 1 year, no participant reported worse than fair, but after 5 years the worst was very poor. Out of 45 participants, 41 reported more severe consequences at 5 years for the indoor subscale. For social life the median at 5 years was 1.75 compared with 1 at 1 year, 1.75 falls between good and fair on the scale. There were no participants at 1 year who reported very poor, the worst was poor, but at 5 years the participants with worst problems reported that their social life was very poor. Out of 44 participants that answered the questionnaire at 5 years regarding the social life subscale, 39 experienced more severe problems and 5 the same, none of the participants experienced fewer problems after 5 years compared with after 1 year. In Table III, the results of the IPA at 1 year and at 5 years post-stroke show that the impact was most pronounced within the autonomy indoor (p < 0.001) and social life (p < 0.001) subscales, where the majority of participants reported a worse situation after 5 years compared with after 1 year.
Table III. Self-perceived Impact on Participation and Autonomy (IPA) 1 year and 5 years after stroke
Strongest correlations between mRS and SIS were seen in the dimensions strength (–0.385), ADL (–0.454) and hand function (–0.461) (Table IV). This means that a higher level of global disability according to the mRS correlates to higher self-perceived impact of strength, ADL and hand function. These correlations were moderate. Moderate correlation was seen between more severe stroke and health-related quality of life.
Table IV. Correlation of global disability assessed by modified Rankin Scale with self-perceived impact of stroke and quality of life at 5 years post-stroke
From 1 to 5 years post-stroke, participants reported a worsening in the self-perceived impact of stroke. Most pronounced were changes in strength, emotion, and participation, as well as autonomy indoors and social life. There were moderate correlations between dependency at discharge from hospital (mRS) and strength, ADL and hand function (SIS) as well as with health-related quality of life (EQ5D) 5 years post stroke.
The results that self-perceived impact of stroke could be more pronounced after several years are shown in a recent longitudinal study over 6 years (9). Similarly, the same trend can be seen in another study (18) where deterioration could be seen in functional outcome during the first year after stroke. An interview study (19) showed that persons with stroke are still facing challenges 5 years post-stroke and view it as an ongoing process. Persons with stroke have fewer social relations and participate less in society after 5 years. Furthermore, persons adjust their life after stroke by, for example, developing new skills and realizing their limitations (19). The results of that study can explain the results of the present study, which showed a lower score for the participation dimension after 5 years.
In the present study, the emotion domain showed significant deterioration at 5 years compared with 1 year. Other studies (20, 21) have shown a relationship between mood state and participation, and this could not be ruled out in the present study. Poor community participation has been shown to be a predictive factor for depression in persons with stroke (20). Another study showed that mood disorders, as measured by Hospital Anxiety and Depression Scale (HADS), was a contributing factor of participation restriction (21). In the IPA, there was a significant deterioration in the autonomy indoors and social life subscales in 1–5 years. A recent study (22) indicated that between 1 and 6 years, the proportion who were satisfied with their family life were lower. This is in line with the present results, with more perceived problems regarding indoor autonomy, which will affect family life.
Previous studies (23, 24) with shorter follow-up periods of 3 and 6 months, respectively, have shown that outdoor autonomy was most affected. It is possible that, with time, people refrain from using mobility devices indoors, and therefore a deterioration in autonomy indoors occurs. It is also possible that the inability to continue doing the same activities as before stroke contributes to the feeling of restrictions in social life (3).
The present study showed moderate correlations between the strength, ADL and hand function dimensions of the SIS and dependency measured by mRS. Considering that mRS measures functional dependency, it seems natural that these dimensions have the strongest correlations with mRS. The correlation in the present study between mRS and ADL was slightly weaker than was seen in another study (25) conducted approximately 3 weeks into rehabilitation. In the present study, the analysis was performed 5 years post-stroke, when the rehabilitation period is completed and people have probably adjusted themselves to their new situation post-stroke.
Limitations
The present study has some limitations that should be taken into account. The study only includes patients who were treated at 1 hospital, where all the thrombolysis and thrombectomy treatments in the region take place, resulting in, for instance, a selection bias towards younger people (since, at the time, there was an age limit on thrombolysis). Furthermore, participants included in the study initially all had impaired upper extremity function, which results in a selected group of participants and may limit the possibility to generalize the results. The method of gathering information, with interviews at 1 year and postal surveys at 5 years, may have influenced the results. However, it has been shown previously that there is a moderate agreement between postal surveys and interviews (26). There is a response bias, with persons with less severe stroke participating in the follow-up. This, as well as the small sample size, reduces the generalizability of the results. This indicates a need for longer, larger follow-up studies. The fact that there is no control population means that the normal ageing process, which could have an influence, is not addressed in the study design. However, since the mean age at stroke onset was 64 years, the healthy normal ageing process between 64 and 69 years will probably not have a large impact on participation.
Conclusion
It appears that the perceived impact of stroke becomes more prominent with time. This is the case even for persons with mild-to-moderate stroke. Some of the most affected areas are emotion and participation. The present study highlights the need for regular long-term follow up for persons with stroke. The content at follow-up should contain not only secondary prevention, but also an assessment of the whole situation for the person. The World Stroke Organization endorsed Post-stroke Checklist (27, 28) is tool to help healthcare workers to identify problems that can be resolved either locally or by referral. The support needed for stroke survivors can come from healthcare as well as from other parts of society.
The study was supported by grants from the Swedish Research Council (VR 2012-70X-22122-01-3, VR2017-00946), The Swedish Heart-Lung Foundation, The Swedish Brain Foundation, Promobilia, Norrbacka-Eugenia Foundation, the Swedish Stroke Association, as well as by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-718711).


 Click to show fullsize
Click to show fullsize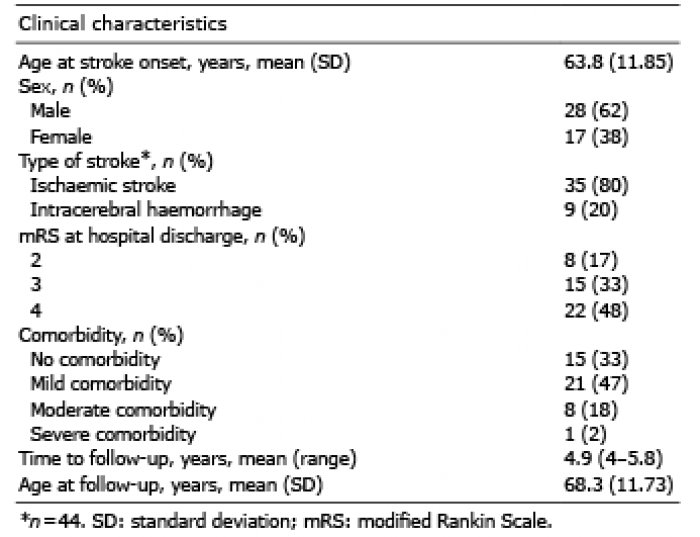 Click to show fullsize
Click to show fullsize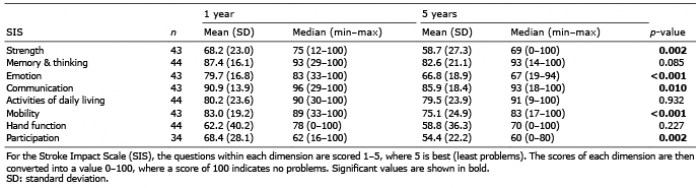 Click to show fullsize
Click to show fullsize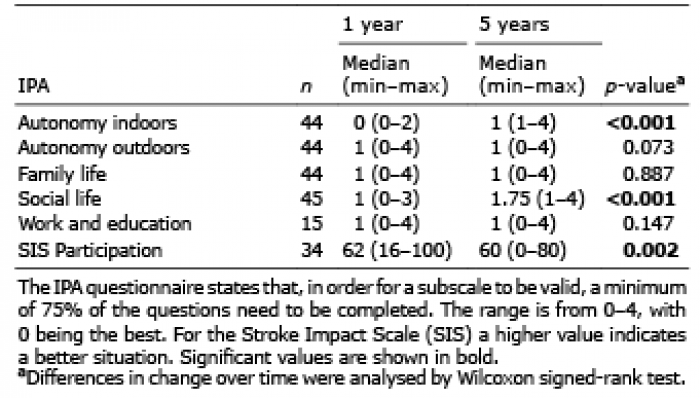 Click to show fullsize
Click to show fullsize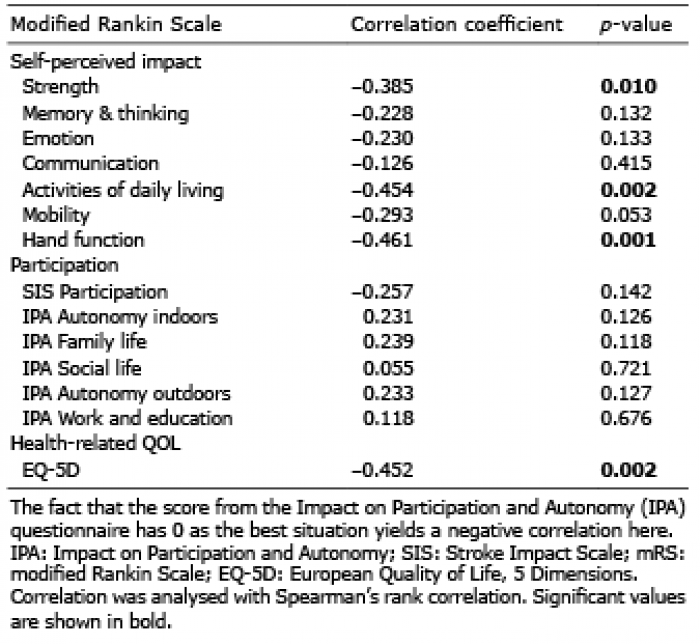 Click to show fullsize
Click to show fullsize