
From the 1Department of Rehabilitation, Shanghai General Hospital, Shanghai Jiaotong University, 2Department of Rehabilitation, School of International Medical Technology, Shanghai Sanda University and 3Department of Rehabilitation, Shanghai Fifth Rehabilitation Hospital, Shanghai, China
Objective: To compare the efficacy of kinesio taping on chronic non-specific low back pain with that of other general physical therapies.
Methods: Relevant studies published up to 31 July 2018 were searched in electronic databases (PubMed, Web of Science, Science Direct, Physiotherapy Evidence Database (PEDro), Cochrane Library, Wanfang Data, Vip Data and China National Knowledge Infrastructure). The quality of included studies was assessed using a risk of bias assessment tool, as recommended by the Cochrane Collaboration. Data from visual analogue scales and Oswestry Disability Index were extracted as selected outcome indicators. Tests of heterogeneity were performed. Weight-ed mean difference (WMD) data with its 95% confidence intervals (95% CI) were used as a measure of effect sizes, in order to pool the results from each included study using either a fixed or random effects model (where appropriate and possible).
Results: Eight studies fulfilled the inclusion and exclusion criteria. The quality of included studies was moderate. Patients with chronic non-specific low back pain in the kinesio taping group achieved better pain relief (WMD = –1.22; 95% CI –1.49 to –0.96, I2 = 91%, p < 0.00001) and activities of daily living (WMD = –7.11; 95% CI –8.70 to –5.51, I2 = 77%, p < 0.0001) than those in the control group.
Conclusion: Kinesio taping may be a new, simple and convenient choice for intervention in low back pain. In the future, we can measure the efficacy about kinesio taping via clinical application in order to prove the possibility of treatment for low back pain.
Key words: kinesio taping; chronic non-specific low back pain; visual analogue scale; Oswestry Disability Index.
Accepted Sep 4, 2019; Epub ahead of print Sep 23, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Bo Yu, Department of Rehabilitation, Shanghai General Hospital, Shanghai Jiaotong University, No. 100, Haining Road, Shanghai 200080, China. E-mail: boyujtu@163.com
Low back pain can be treated with a variety of approaches, as described in clinical practice guidelines. The aim of this study was to determine the efficacy of kinesio taping for pain release and functional improvement in people with chronic low back pain. Significant pain relief was achieved in patients with low back pain with kinesio taping treatment, and taping was superior to physical therapies, with improvement in functional movement. Kinesio taping may be a new, simple and convenient choice for intervention in low back pain.
Low back pain is a major health issue worldwide and severely affects the quality of life of patients, resulting in disability and work absence (1). A 2012 review of the worldwide prevalence of low back pain reported a mean point prevalence of 11.9% (standard deviation (SD 2.0) and 1-year prevalence of 23.2% (SD 2.9) (2). Chronic non-specific low back pain (CNSLBP) caused by acute or chronic lumbar diseases can influence the structure and functioning of the body, leading to reduced muscle strength, endurance capacity and mobility, and reduced ability in activities of daily living (ADL) (3). Mechanical disorders, including injured intervertebral disc, injury to a facet joint or sacroiliac joint, osteoarthritis and lumbar spinal stenosis, are responsible for the main aetiology of CNSLBP (4, 5). In addition, non-mechanical factors, such as infectious, neoplastic, rheumatological, endocrinological, vascular, and gynaecological factors, are also associated with CNSLBP (5).
Self-report questionnaires, such as visual analogue scales (VAS), and the Oswestry Disability Index (ODI), are commonly used to identify the baseline status of patients with chronic low back pain (6, 7). A VAS questionnaire can be used to represent pain intensity before and after treatment on a 0–10 scale, representing progressively increasing pain (6). The ODI is a relative method to assess pain, flexibility, function, and disability changes in a patient’s status. A higher ODI score indicates more severe dysfunction (7). These self-report questionnaires provide descriptions of symptom grade, and are important for planning clinical interventions or treatment.
Management of chronic low back pain currently comprises a range of intervention strategies, including physical treatments (e.g. electrotherapy, traction), exercise therapy, manual therapy (mobilization/manipulation and massage), drug therapy (e.g. paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), opioids, muscle relaxants) and invasive procedures (e.g. acupuncture, injections and nerve blocks) (8, 9). In most situations, the therapeutic effect of a single therapy is not significant and a combination of the above methods is recommended to achieve a good curative effect.
Kinesio taping (KT) is the application of an elastic tape, which can be stretched up to 140% of its original length (approximately the stretch capability of normal skin), for treating musculature-related conditions (10). KT attached to injured skin or muscle regions may enhance muscle strength, relieve spasms, pain and oedema, improve blood circulation and lymph reflux, as well as stabilize joints and increase range of motion (10–12). KT, as a rehabilitative taping technique designed to promote the body’s natural healing process, is widely applied in treatment of CNSLBP (13).
Although the application of KT for patients with CNSLBP is increasing, overall comparison with other therapies of its effectiveness has been little reported. The aim of the current study was to systematically compare the effect of KT or KT plus conventional therapies (e.g. acupuncture, electric therapy or other physical therapy) applied to patients with CNSLBP with that of placebo taping or conventional therapies through assessment of VAS and ODI data.
This meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA) (14).
Search strategy
Randomized controlled trials (RCTs) assessing the effect of KT on patients with CNSLBP, published in Chinese or English, up to 31 July 2018, were systematically retrieved from several databases: PubMed, Web of Science, Science Direct, Physiotherapy Evidence Database (PEDro), Cochrane Library, Wanfang Data, Vip Data and China National Knowledge Infrastructure. Search terms were a combination of key words and free-text terms (“chronic non-specific low back pain” OR “non-specific low back pain” OR “low back pain” OR “back pain”) AND (“kinesio taping” OR “elastic taping” OR “taping”).
Inclusion and exclusion criteria
Inclusion criteria for the studies were: (i) the design of the study was an RCT and participants were patients with CNSLBP; (ii) patients with CNSLBP should present with an episode of chronic pain with limitation of motion in the lower back and demonstrate a normal low back on X-ray, computed tomography (CT) or magnetic resonance imaging (MRI); (iii) the study must compare the effect of KT and other non-elastic taping or other conventional therapy; (iv) the main outcomes of VAS and ODI in individuals with CNSLBP were tested.
Exclusion criteria were: (i) the sample size was no more than 15 subjects (15) ; (ii) the full text was not available; (iii) relevant outcomes were lacking; (iv) the study was a systematic review, case report, comment or letter; (v) the study was published repeatedly; (vi) participants had clinical signs of spondylolisthesis, lumbar stenosis, infectious pathologies in the spine, or inflammatory diseases with spine involvement; (vii) participants had previously undergone spinal surgery.
Retrieved article titles and abstracts were read to assess whether the study was eligible, with reference to the inclusion and exclusion criteria above; otherwise, the full text was read if the information was unclear.
Data extraction
Article selection and data extraction were completed independently by 2 reviewers, and a consensus was achieved by discussion. The following data were extracted from each included study: name of first author, year of publication, study characteristics (sample size, interventions, treatment frequency, outcomes measure, and follow-up time), and participants’ characteristics (mean age, sex, and duration of disease). If the original data was unclear or lacking, the corresponding author was contacted to obtain further information. Articles were excluded if the authors could not be contacted.
Quality assessment
The quality of each included study was assessed with a risk of bias assessment tool, as recommended by the Cochrane Collaboration (16). This tool evaluates the selection, performance, detection, attrition, and reporting bias with 7 items. If discrepancies were found for a specific item, a final agreement was reached by discussion with a third reviewer. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) system was applied to evaluate the overall quality of the evidence and the strength of recommendations according to outcome (17). The grade of confidence in the estimate of effect was categorized into 4 levels: “very low”, “low”, “moderate”, and “high”.
Quantitative data synthesis
Meta-analysis was performed with RevMan 5.3 software. VAS and ODI were selected as outcome indicators. Weighted mean difference (WMD) data with its 95% confidence intervals (95% CI) was used as a measure of effect sizes to pool the results from each included study. Heterogeneity within the included studies was evaluated by Q test and I2 index (18). A fixed effects model was applied for data synthesis when no significant heterogeneity was detected (p > 0.05 or I2 < 50%) (19); otherwise, a random effects model was used if significant heterogeneity was found (p < 0.05 or I2 ≥ 50%) (20).
Sensitivity analysis
In order to investigate the heterogeneity of sources, sensitivity analysis was conducted to assess the influence of each study on the combined result by removing studies one at a time.
RESULTS
Eligible studies
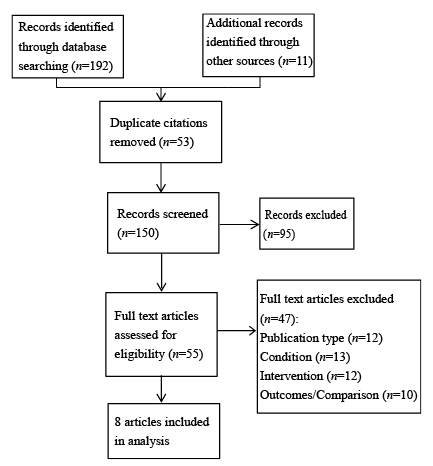
A total of 203 articles were retrieved using the preliminary search strategy. Of these, 53 repeated articles were excluded. After reading the abstracts, a further 95 irrelevant or ineligible articles were excluded. The full texts of the remaining 55 articles were reviewed in detail, and 47 were removed based on the exclusion and inclusion criteria. A final total of 8 eligible articles were therefore included in the present study (21–28) (Fig. 1).
Characteristics of included studies
The main characteristics of each included study are shown in Table I. These studies were published during 2012–2015 and enrolled a total of 530 participants, aged 18–80 years, including 257 male and 273 female patients with CNSLBP. Patients with CNSLBP in the control group were provided with conventional therapies, including physical therapy (combined massage, strength training and endurance training), combined ultrasound, hot packs and transcutaneous electrical nerve stimulation (TENS), separate acupuncture, or separate high- + medium-frequency electric therapy, etc., while patients in the treatment group were treated with KT with or without the above interventions.
Fig. 1. Flowchart of study selection for the meta-analysis.
Table I. Summary of the basic information of included trials.
Quality assessment of the included studies
The quality of each included study is shown in Fig. 2. The majority of studies had a low risk of bias in random sequence generation, allocation concealment, incomplete outcome data, and others. However, 5 studies had a high risk of unblinding of participants and personnel, and 4 studies had a high risk of unblinding of outcome assessment. In addition, all studies had a high or unclear risk of selective reporting. Collectively, the quality of included studies was moderate.
Fig. 2. Risk of bias assessment for the included studies. –: high risk of bias; +: low risk of bias; ?: unclear risk of bias.
Data synthesis of outcome measures
VAS assessment. The VAS score was used as outcome indictor in all the included studies. High heterogeneity was detected within all included studies (p < 0.00001 and I2 = 91%), thus a random effect model was applied to pool the VAS data of each study. The pooled results demonstrated that significantly reduced pain was achieved in 258 patients with CNSLBP with KT treatment compared with 252 patients in other conventional
therapy groups (WMD = –1.22; 95% CI = –1.49 to –0.96; Fig. 3). In addition, sensitivity analysis showed that a significantly reduced VAS was found after omitting all included studies one at a time (ranges of WMD (95% CI): –1.30 (–1.58, –1.02) to –1.10 (–1.33, –0.86), p < 0.001), demonstrating that the pooled VAS result was stable (Fig. 4).
Fig. 3. Forest plot of efficacy evaluation according to visual analogue scale (VAS) (kinesio tape vs other therapy groups). Squares indicate outcome estimates for corresponding study, and the size of the square indicates the weight of the corresponding study. Horizontal lines and figures in parentheses represent the 95% confidence interval (95% CI). Diamonds indicate the pooled effect size with the corresponding 95% CI. SD: standard deviation.
Fig. 4. Forest plot of efficacy evaluation on the Oswestry Disability Index (ODI) (kinesio tape vs other physical therapy groups).
ODI assessment. All the studies reported the ODI score, and significant heterogeneity was found among these studies (p < 0.0001 and I2 = 77%). Therefore, the random effect model was used for merging ODI score. The WMD for ODI was –7.11 (95% CI –8.70 to –5.51, Fig. 5), indicating that KT had a more positive effect on improving ADL than other methods of conventional therapy. A stable ODI result was found by sensitivity analysis after omitting the included studies one at a time (ranges of WMD (95% CI) –7.51 (–9.17, –5.86) to –6.20 (–7.37, –5.03), p < 0.001) (Fig. 6).
Fig. 5. Results of sensitivity analysis for visual analogue scale (VAS) after omitting each study one at a time. CI: confidence interval.
Fig. 6. Results of sensitivity analysis for the Oswestry Disability Index (ODI) after omitting each study one at a time. CI: confidence interval.
GRADE evidence
The overall confidence in the estimates of VAS and ODI was low due to the risk of bias and inconsistency, which may reduce the recommendation strength of the pooled results (Table II).
Table II. Grading of Recommendations Assessment, Development and Evaluation (GRADE) evidence quality for each outcome
This meta-analysis included 8 eligible studies that were relevant to the evaluation of efficacy of KT on pain relief and ADL progress for patients with CNSLBP. KT was found to be superior to other conventional therapies (e.g. physical therapy (combined massage, strength training and endurance training), acupuncture, or high- + medium-frequency electric therapy) applied to CNSLBP, with significantly decreased VAS and ODI scores.
The findings of the current study indicate that KT is superior to other methods, including no taping, acupuncture and other general physical therapy methods, for CNSLBP patient treatment, with reduced VAS and ODI. Similarly, Kelle et al. demonstrated a significant improvement in pain control in a KT group compared with a control group for patients with acute non-specific low back pain (29). A RCT study conducted by Forozeshfard et al. demonstrated that KT significantly reduces pain and functional disability in young females with menstrual low back pain (30). Moreover, it has been reported that application of KT results in a significant reduction in neck and low back pain, as well as disability indexes in surgeons with musculoskeletal pain (31).
Although a variety of studies demonstrate the effect of KT on pain relief, functional performance, disability and improvement in ADL, the specific mechanism of action of KT remains unclear. Possible explanations for the mechanism of pain relief are that KT can effectively increase the kinesio taping may provide force on skin and increase the gap which is underneath the skin or the gap between epidermis and dermis, promote subcutaneous blood and lymphatic reflux, and accelerate the healing of injured areas through its own natural tension. In addition, KT can produce continuous sensory input to the skin sensors, which may relatively suppress the sensory input of pain perception (32). An additional possible explanation for functional performance, disability or improvements in ADL is that application of KT may increase the range of motion of the temporomandibular joint during exercise (33).
Study limitations
Although this study resulted in some meaningful implications, it also has several limitations. First, a limited number of studies were included; there is a need for more high-quality RCT studies with large sample sizes to confirm the reliability of the present study. Secondly, the total quality of included studies was rated as moderate, and overall confidence in the VAS and ODI estimates was low, which may lead to overestimation of effect and reduction in the recommendation rate of our pooled results. Thirdly, because there are few RCTs on this topic, this supports the inclusion of other measures of pain and disability, and since we only investigated VAS and ODI measures to assess the pain and disability, it is possible that relevant studies may have been missed. Fourthly, methodological heterogeneity occurred in many included studies, with comparisons between different intervention strategies, and several studies assessed the combined effect of KT and other intervention strategies. Thus, further studies are needed to compare KT separately with some specific general interventions. Finally, the shape, direction and tensile force of KT for pain reduction or functional performance are different in different individuals (34). Further studies, focusing on the effect on pain reduction or improvement in functional performance using different shapes, directions or tensile forces of KT, should be included in the analysis.
Conclusion
This meta-analysis demonstrated that KT, either separately or in combination with other general therapies, resulted in greater pain relief and improvement in ADL in patients with CNSLBP than did general physical therapies without KT.
This study was supported by the programme of Shanghai Science and Technology Committee (No.16411955200) and Scientific Research and Innovation Team Funding Plan of Shanghai Sanda University.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize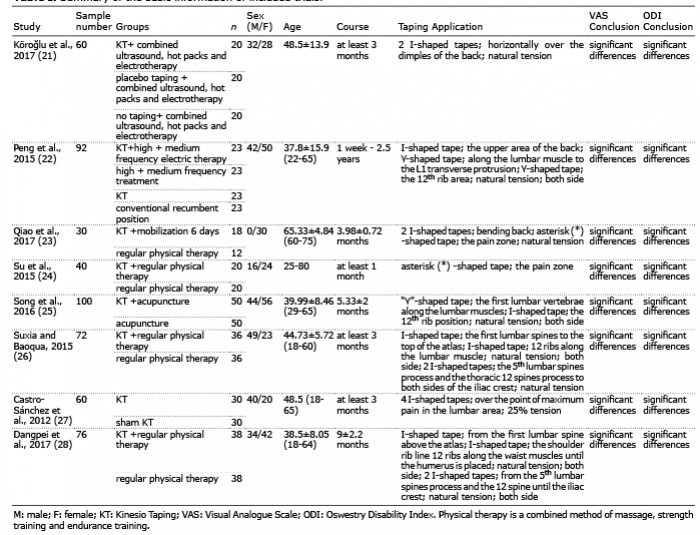 Click to show fullsize
Click to show fullsize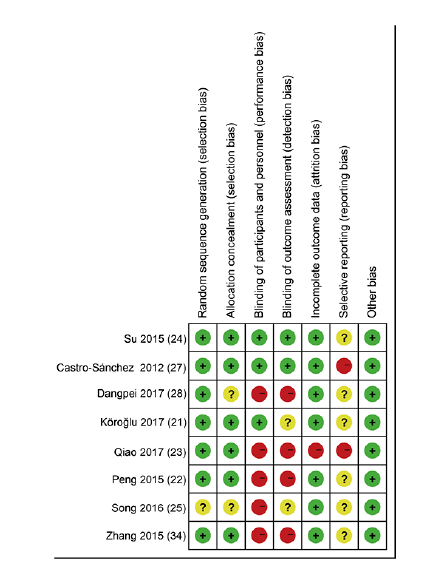 Click to show fullsize
Click to show fullsize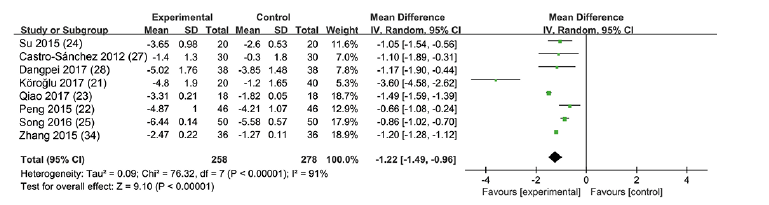 Click to show fullsize
Click to show fullsize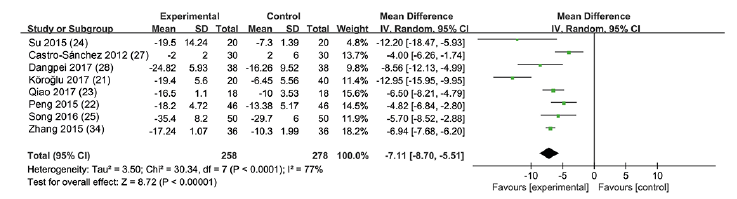 Click to show fullsize
Click to show fullsize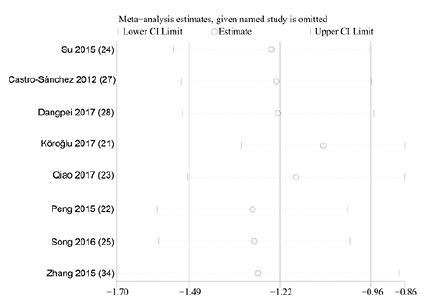 Click to show fullsize
Click to show fullsize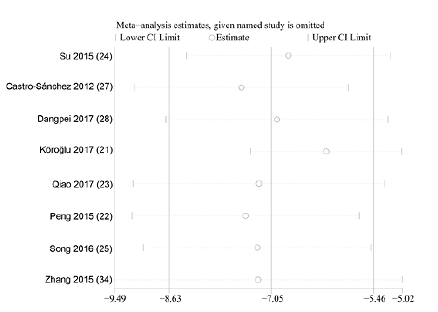 Click to show fullsize
Click to show fullsize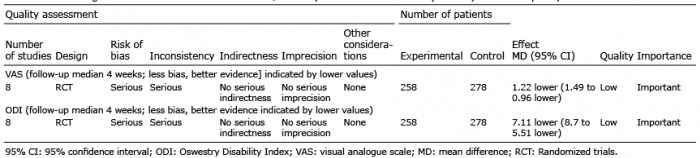 Click to show fullsize
Click to show fullsize