
From the Department of Rehabilitation Medicine, The First People’s Hospital of Changzhou & Third Affiliated Hospital of Soochow University, Changzhou, Jiangsu, China
Objective: To analyse disorders and components of attention in patients with complicated mild traumatic brain injury. This information is needed to en-able clinical workers to evaluate and provide training for attention deficits in patients with mild traumatic brain injury.
Design: Randomized controlled trial.
Setting: In-patient and community recruitment.
Participants: In-patients with mild traumatic brain injury (n = 44) and community-recruited healthy subjects (n = 45).
Outcome measures: All participants used a battery of attention tests including the Digit Span Test (DST), Digit Cancellation Test (D-CAT1 and D-CAT2), Symbol Digit Modalities Test (SDMT), and the Paced Auditory Serial Addition Test (PASAT).
Results: There were no differences in the results of the D-CAT between the patient and control groups (p > 0.05); however, there were significant differences in the DST, SDMT and PASAT (p < 0.01).
Conclusion: Patients with mild traumatic brain injury were found to have normal sustained attention and selective attention, but impaired attention span, divided attention, shifting attention and information processing speed, requiring clinical workers to focus more on these deficits.
Key words: mild traumatic brain injury; attention; cognitive function.
Accepted Mar 27, 2020; Epub ahead of print Apr 8, 2020
J Rehabil Med 2020: 52: jrm00050
Correspondence address: Yi Zhang, Department of Rehabilitation Medicine, The First People’s Hospital of Changzhou & Third Affiliated Hospital of Soochow University, No.185 Juqian Street, Changzhou City, Jiangsu, China. E-mail: 83232136 @qq.com
Patients with mild traumatic brain injury generally have a good prognosis. However, some patients develop attention deficit, which affects their life and work. This study evaluated the components of attention in patients with traumatic brain injury. The results show that patients with complicated mild traumatic brain injury had significant deficits in attention span, divided attention, shifting attention and information processing speed. Thus, clinicians should take into consideration these aspects of attention in treating patients with traumatic brain injury, in order to provide early rehabilitation interventions that may reduce the adverse effects of these deficits on life and work.
Traumatic brain injury (TBI) continues to be a critical public health and socioeconomic problem worldwide. The incidence of TBI worldwide is reported to range from 47.3 to 849 hospital admissions per 100,000 people per year (1), including mild traumatic brain injury (mTBI), which accounts for more than 80% of cases (2). MTBI can alter the structure of the brain and result in a range of disorders, including a wide range of cognitive impairments (3). Neurological damage associated with mTBI has traditionally been viewed as transient, yet a growing number of studies has suggested long-lasting cognitive changes following mTBI (4). The impact of TBI on cognitive functioning can be extensive and far ranging. Attention and memory deficits are the most prominent cognitive impairments commonly reported by patients and their relatives, and these deficits affect the daily lives of patients. These symptoms, may make it unsafe for people with mild brain injury to drive (5).
Attention is a basic cognitive function, which therefore interacts closely with all other cognitive processes. It is not considered a unitary process, but is composed of different and, in part, highly specific components. Based on attentional performance measures, Mirsky et al. proposed 5 main components of attention, including attention span (6) , sustained attention (7), selective attention (8), divided attention and shifting attention (9). According to another theoretical model of attention, attention is also divided into endogenous (top-down) and exogenous (bottom-up) processes. Endogenous attention involves the conscious control of attention directed toward some target. Conversely, exogenous attention occurs when the brain automatically orients or attends to salient sensory characteristics in the environment. Both endogenous and exogenous attention have relatively independent neural anatomical networks (10).
An attention disorder is characterized by a lack of focus, a tendency to become distracted, and the incapacity to do 2 things at once, such as listening while writing. In addition, attention can affect memory (11), executive function and other related cognitive processes (12). There have been few studies on attention disorders in patients with TBI, and most of these focus on a single component or an integrated measure of attention in patients with moderate and severe TBI. Such components include sustained attention (13), selective attention (14) or response inhibition, and divided attention (15). To date, no study has conducted a multicomponent analysis of attention in patients with mTBI.
The objectives of this study were to assess all components of attention in patients with mTBI and to compare performance on these components with performance in a control group. Understanding of the attention characteristics of patients with mTBI will provide a theoretical basis and potential targets for treatment to guide clinical work.
This study was approved by the institutional review boards of the participating hospitals.
Subjects
A total of 205 participants, including the mTBI group and control group, were eligible for this study. Subjects for the control group were randomly recruited from the community service center of hongmei street in changzhou, which serves 80,000 residents. Patients in the mTBI group were recruited from the Neurosurgery Department of The First People’s Hospital of Changzhou during May 2017 to January 2018 (a period of 8 months). Patients in the mTBI group were tested withinone week of injury. The inclusion criteria for the cohort of patients with mTBI were: (i) age over 18 years; (ii) no history of brain trauma, stroke or other neurological disease; (iii) Glasgow Coma Scale (GCS) score 13–15 determined within the first 24 h post-injury or indicated by magnetic resonance imaging (MRI) or computed tomography (CT) scan; (iv) able to understand and speak Mandarin proficiently; and (v) provided informed consent, as did their guardians. According to the Mild Traumatic Brain Injury Committee of the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine, the definition of mTBI included at least one of the following: (i) any loss of consciousness; (ii) any loss of memory for events immediately before or after the accident; (iii) any alteration in mental state at the time of the accident; (iv) focal neurological deficit(s) that may or may not be transient (16); but where the severity of the injury does not exceed the following: (i) loss of consciousness of approximately 30 min or less; (ii) after 30 min, an initial GCS of 13–15; (iii) post-traumatic amnesia (PTA) not greater than 24 h.
Exclusion criteria were as follows: (i) severe visual and auditory impairment; (ii) severe aphasia; (iii) other neurological diseases, psychiatric illnesses or other medical complications; (iv) previous brain damage or head injury history; and (v) failure of the patients and their guardians to cooperate or be evaluated.
Measurements
Attention test battery. All enrolled subjects were tested by the same trained rehabilitation physician, and all tests were conducted in a quiet, undisturbed environment, in order to reduce interference from the external environment on attention outcomes. Assessment and scoring were carried out in strict accordance with the operation manual, to ensure consistency in testing.
The attention test battery included the Digit Span Test (DST), Digit Cancellation Test (D-CAT), Symbol Digit Modalities Test (SDMT), and the Paced Auditory Serial Addition Test (PASAT), which tested 5 components of attention, including attention span, sustained attention, selective attention, shifting attention and divided attention (15, 17).
The DST in the Wechsler batteries (the intelligence and memory scales) are the format in most common use for measuring span of attention. These batteries comprise 2 different tests: Digits span Forward and Digits span Backward. The Digits span Forward test requires subjects to repeat a series of digits, with the number of digits increasing over trials. The numbers in the series were presented orally at a rate of 2/s to prevent rehearsal. The series length began with 2 digits and gradually increased to 10 digits. The Digits span Backward test required subjects to recall digits in reverse serial order (e.g. 1-2-3 would be correctly recalled as 3-2-1). The DST mainly measures attention span when evaluating attention (15).
In 1974, Diller et al. constructed 9 different cancellation tests. One of these was the D-CAT, which consists of 2 parts: tests 1 and 2. Tests 1 and 2 were used to assess sustained attention and selective attention, respectively. Test 1 consisted of 4 pages with 800 randomly chosen digits, with even spaces between digits. Subjects were instructed to cross out all instances of the number 3 as quickly as possible. The final result takes into consideration the number of correctly crossed-out digits, the number of incorrectly crossed-out digits, and the time taken to complete the test. In test 2, subjects were instructed to cross out numbers in front of 3 as quickly as possible. The evaluation was similar to test 1 (18).
The SDMT is a measure of attention switching, which was developed by Smith (19). The test form is placed before the patient, and the examiner reads the instructions provided in the SDMT Manual. As in the older versions of the Wechsler Digit Symbol subtest, subjects are allowed 90 s to complete the trial. The patient fills in the numbers that correspond to symbols (i.e. “marks”) according to the key provided at the top of the page. Performance indicators include the number of completed numbers, correct numbers and scores.
The PASAT has been widely used to assess divided attention (20). There are many versions of the test. The current study used the 2-s trial of the PASAT.
A random series of numbers from 1 to 9 are presented, and the subject is instructed to consecutively add pairs of numbers, such that each number is added to the number that immediately preceded it (i.e. the second number is added to the first, the third number to the second, the fourth number to the third, etc.). For example, if the stimulus “1” followed by “9” is presented, the examinee must respond “10”; if the next stimulus is “4,” the examinee must respond “13” (i.e. by adding “4” to the previous digit “9,” not to the examinee’s own response of “10”), and so on. This response requirement is sustained over numerous items until the end of the trial.
Statistical analyses
The mean value and standard deviation (SD) were used to describe the data distribution. All data were tested for homogeneity of variance. Independent t-tests used to compare the mTBI group with the control group in demographic data, such as age, education and sex. When the variance was homogeneous, one-way analysis of variance (1-way ANOVA) was used to assess differences in the attention test battery. If the variance was not homogeneous, the Wilcoxon rank-sum test was used. p ≤ 0.05 was considered statistically significant. All tests were one-tailed. The analyses were performed using the Statistical Package for Social Sciences software for Windows 10, v22 (SPSS; IBM Corp; USA).
Sample characteristics
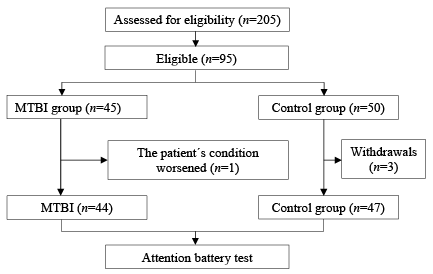
From a total of 205 participants, 110 were excluded. The remaining 95 participants (45 patients with mTBI and 50 healthy adults from the community) were recruited to the study. During the test, one patient with mTBI withdrew as a result of a worsening condition. Three of 50 healthy control subjects did not complete the tests for personal reasons. A total of 47 subjects remained in the control group (Fig. 1).
Fig. 1. Flow diagram of participants in the study. MTBI: mild traumatic brain injury.
A final total of 91 subjects were included in the study (44 in the mTBI group and 47 in the control group). Demographic characteristics of the subjects are shown in Table I. There was no significant difference between the 2 groups in terms of sex, age, level of education, hypertension and diabetes. In the mTBI group, the type of intracranial lesion included traumatic subarachnoid haemorrhage (t-SAH), brain contusion (ICH), subdural haematoma (SDH), epidural haematoma (EDH), intracerebral haematoma, concussion and brain stem haematoma. The mean GCS score in patients with mTBI was 14.55 (SD 1.19). The common causes of mTBI were slipping, getting hit by heavy objects, traffic accidents, and falling, with traffic accidents being the most common.
Table I. Demographic and clinical information about the participants of the study
Attention span
The DST was used to measure attention span, as shown in Table II. In the Digits Span Forward test, the mTBI group and the matched control group showed a significant difference (p < 0.01). In the Digits Span Backward test, there was a statistically significant difference between the 2 groups (p < 0.05).
Table II. Attention span
Sustained attention
This study used the D-CAT test 1 to assess sustained attention. Compared with the control group, the mTBI group showed no differences in terms of correct numbers (p > 0.05), incorrect numbers (p > 0.05), leakage numbers (p > 0.05), net scores (p > 0.05) and error rate (p > 0.05); choice reaction time was significantly different (p < 0.05) (Table III). The mean number of correct numbers in the mTBI group was 29.64, which was within the 95% confidence interval (95% CI) of the control group and was consistent with the results of 1-way ANOVA. The number of incorrect responses, leak number, net score and error rate were the same across groups. However, the mean choice response time was significantly higher (i.e. more than the upper 95% CI) in the mTBI group than in the control group.
Table III. Sustained attention
Selective attention
To assess selective attention, the D-CAT test 2 was used. Participants were instructed to cross out digits in front of 3, which was different from D-CAT test 1. In D-CAT test 2, there were no differences in terms of correct numbers (p > 0.05), incorrect numbers (p > 0.05), leakage numbers (p > 0.05), net scores (p > 0.05) and error rate (p > 0.05) between the mTBI and control groups; however, the choice reaction time was different between the groups (p > 0.05) (Table IV). The mean number of correct numbers in the mTBI group was 28.75, which was within the 95% CI of the control group and consistent with the results of the 1-way ANOVA. The number of incorrect responses, leak number, net scores and error rates were the same across groups. However, the mean choice response time in the mTBI group was significantly increased compared with the control group, which was consistent with the results from D-CAT test 1.
Table IV. Selective attention
Attention switching
This study used the SDMT to measure attention switching. The 2 groups were compared, and the results, including the completed numbers, correct numbers and scores, showed significant differences (p < 0.01) (Table V).
Table V. Attention switching
Divided attention
Similarly, divided attention was measured with the PASAT. After comparing the 2 groups, the results showed a significant difference (p < 0.01) in the number of correct answers (Table VI).
Table VI. Divided attention
Attention plays a very important role in our daily lives. Attention disorders after mTBI may affect people’s daily lives and work. Attention disorders in patients with TBI are related to the destruction of brain tissue. Studies have found that attention is commonly associated with the frontal, cingulate and parietal cortices, subcortical white matter, and reticular activating systems (21). However, the frontal lobe is one of the most vulnerable areas in TBI (22). On the other hand, changes in neurotransmitters often occur after TBI, and attention is also associated with changes in neurotransmitters, such as dopamine, acetylcholine and norepinephrine (23). Compared with stroke, TBI leads to a wider range of damage through more complex mechanisms. In patients with TBI and no structural damage, as assessed by conventional imaging examination, the use of functional MRI technology can reveal small structural or functional abnormalities, which may be the pathological basis of cognitive abnormalities, including attention deficits. The subjects in this study were all hospitalized patients with mTBI accompanied by visible brain tissue damage on CT, and their attention impairments were obvious. Attention is not conceptualized as a unitary and well-localized function, but is composed of a number of distinct processes. In the present study, the characteristics of attention in patients with mild brain injury is different from the healthy subjects.
Attention span refers to the number of objects that people perceive or recognize in an instant. According to various theoretical models of attention, attention span consists of phasic alertness (a bottom-up process) and an encoding process (a top-down process) (24). It has been reported that attention span is associated with the right cerebral hemisphere (25). In the current study, the DST showed significant deficits in attention span in the patients with mTBI compared with controls. This result was consistent with those of Bate et al. (26).
Sustained attention refers to a person’s ability to focus steadily on a particular object and activity for a certain period of time. For example, when reading a book, a person may be able to concentrate for an hour without being distracted by interference from others. Attention deficits may lead to more errors and diminished quality of work as a result of a gradual decrease in alertness. According to a current model of attention, sustained attention has 2 components: tonic alertness (a bottom-up process) and focused attention (a top-down process) (27). According to previous studies, tonic alertness and focused attention are related to the left cerebral hemisphere (25) and the right frontoparietal system (28), respectively. In 1991, Mirsky suggested that sustained attention was reliant on the rostral midbrain and thalamic nuclei, which may be less vulnerable to injury from TBI compared with the prefrontal, inferior parietal, and superior temporal cortical regions that support the shifting of attention. In this study, D-CAT test 1 indicated that sustained attention was not impaired in patients with mTBI. In patients with severe brain injury, sustained attention is impaired, and the present results were inconsistent with Chan’s conclusions (29). These inconsistencies in results may be closely related to the severity of damage to the brain tissue after TBI. Alternatively, the inconsistencies might have been related to performance on the visual and auditory tasks.
Selective attention refers to a person’s ability to filter information to detect relevant information and reject or inhibit distracting information. Selective attention is also related to 2 processes: selective attention (a bottom-up process) and inhibition (a top-down process). Selective attention has been related to posterior parietal and anterior midline structures and the basal ganglia. Inhibition is related to the dorsal anterior cingulate and posterior cingulate cortex (30). In the D-CAT test 2 there were no significant differences in the correct numbers, incorrect numbers, leakage numbers, net scores and error rate between the 2 groups. These results suggest that patients with mTBI have no significant problems with selective attention. These results are inconsistent with selective attention deficits reported after severe TBI (31). This may be related to the locations and magnitude of brain damage. However, there were significant differences in response times between the 2 groups. This suggests that information processing speed in patients with mTBI may be affected. Similarly, Philip & Annette’s study found a decrease in information processing speed in patients with mTBI (32).
The shifting of attention refers to the ability of a person to actively and purposefully direct attention from one object or activity to another in a timely manner. According to some models, shifting attention is a top-down attention process. Many studies have found that shifting attention is closely related to the frontal and parietal lobes, including the inferior region of the parietal lobe (33, 34), the dorsal anterior cingulate cortex (ACC), and regions of the middle frontal gyrus (33). In the SDMT, the results of the control group were better than those of the mTBI group (p<0.01). This suggests that attention shifting is impaired in patients with mTBI. Moreover, most of the subjects in this study had frontal lobe lesions, which is consistent with the above anatomical lesion locations. A study by Kinsella et al. (35) with elderly patients with mTBI (older than 65 years), found that shifting attention was also impaired. These findings are consistent with those of other studies (36).
Divided attention means that a person can distribute his/her attention equally among various activities (e.g. cooking while listening to the news). This process is also a form of top-down attention. Disorders affecting divided attention often slow down the gait and simultaneously reduce the attention span of patients with mTBI (37). Current research shows that divided attention is associated with the dorsolateral prefrontal cortex and anterior cingulate gyrus (28). In the PASAT, comparing the results between the 2 groups revealed a significant difference (p < 0.01). This suggested that divided attention in patients with mTBI is also affected. This finding is consistent with the results of Paré et al. (38). Similarly, the divided attention of patients with severe brain trauma is also decreased (31). However, Dall’Acqua et al. (39) showed that divided attention with auditory stimuli was normal, but divided visual attention was impaired in patients with mTBI, which was different from our findings.
Study limitations
This study has some limitations. First, there was a lack of detailed information about the subjects in the current study, such as smoking and drinking histories, presence of obstructive sleep apnoea (OSA), and intake of drugs that may affect cognition (40). Differences in these factors may have influenced the results. Secondly, the tests used in this study were all traditional attention tests; however, some tests are considered controversial for testing specific components of attention. Thirdly, the testing in this study was conducted in a quiet room, which may be different from people’s normal environment. Therefore, the study lacks ecological validity. Fourthly, this was a cross-sectional study, which lacks longitudinal data on changes in attention over time; thus, it was not possible to track changes that may occur at later stages. Finally, the sample size was relatively small, and there is a lack of multicentre randomized controlled studies.
Conclusion
In patients with complicated mTBI, some components of attention are impaired, mainly attention span, divided attention, shifting attention and information processing speed. Although some patients undergo full recovery of attention, some patients have long-term impairment of different components of attention. Thus clinicians should assess attention processes in patients with mTBI as early as possible and follow up these patients regularly. These results may help clinicians and neuropsychologists to assess potential attention disorders in patients with mTBI for clinical intervention, while guiding the focus of attention training.
The authors would like to thank Drs Ting Sang, Fan Xie, Chaolan Wang and Jiao Deng for collecting the data.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize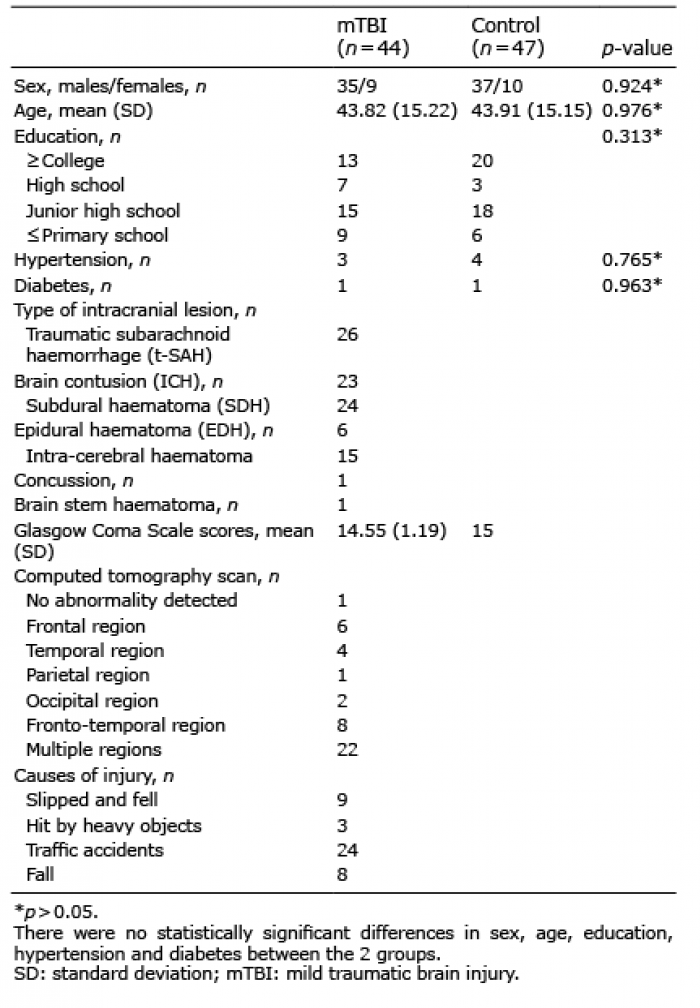 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize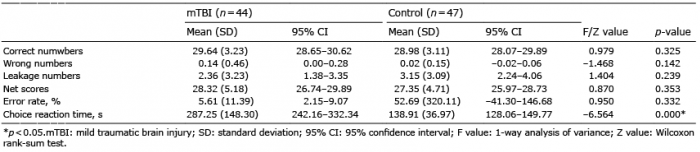 Click to show fullsize
Click to show fullsize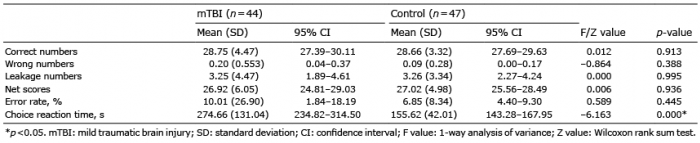 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize