
From the 1China Research Center on Disability, School of Public Health, Fudan University, 2Shanghai Yangzhi Rehabilitation Hospital (Shanghai Sunshine Rehabilitation Center), Shanghai, China, and 3School of Community and Environmental Health, Old Dominion University, Norfolk, VA, USA
#These authors contributed equally.
Objective: To evaluate the quality of life of patients with chronic spinal cord injury in mainland China.
Design: Cross-sectional study.
Subjects: A total of 247 adults ≥ 1 year post-SCI in mainland China.
Methods: The World Health Organization (WHO) Quality of Life Scale Brief Version (WHOQOL-BREF) and the add-on modules on disability-related QoL (WHOQOL-DIS) were used to assess quality of life. Anxiety/depression was measured using the Zung Self-Rating Anxiety/Depression Scale. Quality of life was compared with that of reference populations from China, Korea, the international field trial (23 countries). Multivariate linear regression was conducted to determine the factors that might be associated with quality of life.
Results: The means of the 4 domains of the WHOQOL-BREF varied from 11.5 to 13.0. The mean of the 12-item WHOQOL-DIS module was 38.7. The quality of life of the participants as measured by the WHOQOL-BREF was 1.1–4.7 points lower than that of the global reference population, while quality of life as measured by the WHOQOL-DIS module was 1.2 points lower than that of the Korean data. Anxiety and depression were negative factors associated with quality of life (p < 0.05). Better community integration was a positive factor for physical quality of life and quality of life as measured by the WHOQOL-DIS module (p <0.01).
Conclusion: The quality of life of adults with chronic spinal cord injury in mainland China was lower compared with reference populations. Duration of spinal cord injury, sex, community integration, anxiety, and depression were related to quality of life.
Key words: spinal cord injury; quality of life; community; comparative study; China.
Accepted Apr 23, 2020; Epub ahead of print May 8, 2020
J Rehabil Med 2020; 52: jrm00058
Correspondence address: Jun Lu, China Research Center on Disability, School of Public Health, Fudan University, Shanghai, China, 200032. E-mail: junlu_shmu@163.com
Quality of life is an important outcome in spinal cord injury rehabilitation practice and research. This study described the quality of life profile of 247 adults with c-hronic spinal cord injury in mainland China. The quality of life of the participants was lower than that of the global reference population, as was disability-related quality of life compared with the Korean data. Duration of spinal cord injury was a positive factor in the physical health of adults with spinal cord injury, while anxiety and depression were negative factors associated with quality of life in the same population. Community integration improvement was correlated with better physical and disability-related quality of life. To improve quality of life, rehabilitation schemes may include interventions to promote mental health and community integration among patients with chronic spinal cord injury.
A spinal cord injury (SCI) can be devastating, because SCI is still not curable (1) and SCI patients often require lifelong treatment and rehabilitation, resulting in heavy economic and emotional burdens. Quality of life (QoL) is regarded as the key outcome of SCI rehabilitation (2). It is defined by the World Health Organization (WHO) as “individuals’ perceptions of their positions in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.” Previous studies assessing the QoL of people with SCI have used the International SCI QoL Basic Data Set (3), the Short Form 36 Health Survey (SF-36) (4), and the WHO Quality of Life (WHO QoL) Scales, comprised of the WHO Quality of Life Scale Brief Version (WHOQOL-BREF) and the add-on modules on disability-related QoL (WHOQOL-DIS module) (5).
It is estimated that at least 1 million people with SCI live in mainland China, with 60,000 new cases every year (6). There has been extensive research into QoL of people with SCI in developed countries (7, 8). To the best of our knowledge, a management information system for adults with SCI was still not set up in mainland China at the time of this study, and QoL information was not collected in routine healthcare systems (9). Little research has examined the QoL of adults with chronic SCI (cSCI), meaning those who have lived with SCI for at least one year, using the WHOQOL Scales. The measurement tools applied in QoL-related research on patients with SCI in mainland China focuses on the WHOQOL-BREF (10–12), but very few studies have used the WHOQOL-DIS module to measure QoL in patients with SCI.
The objective of this study was to examine the QoL of adults with cSCI in mainland China. The specific aims were: (i) to describe perceived mental functioning, community integration, and QoL in relation to values from the reference population, where available, in Guangzhou, China (13), and other countries; and (ii) to examine the factors associated with QoL of adults with cSCI.
Participants and procedures
The Shanghai Sunshine Rehabilitation Center’s (SSRC) “Hope House/Halfway House” project provided the participants. The project is a government-supported programme that provides inpatient rehabilitation training services for people with SCI from Shanghai and other provinces (14). Researchers asked those who agreed to participate in the study to sign informed consent prior to the survey soon after admission to Hope House.
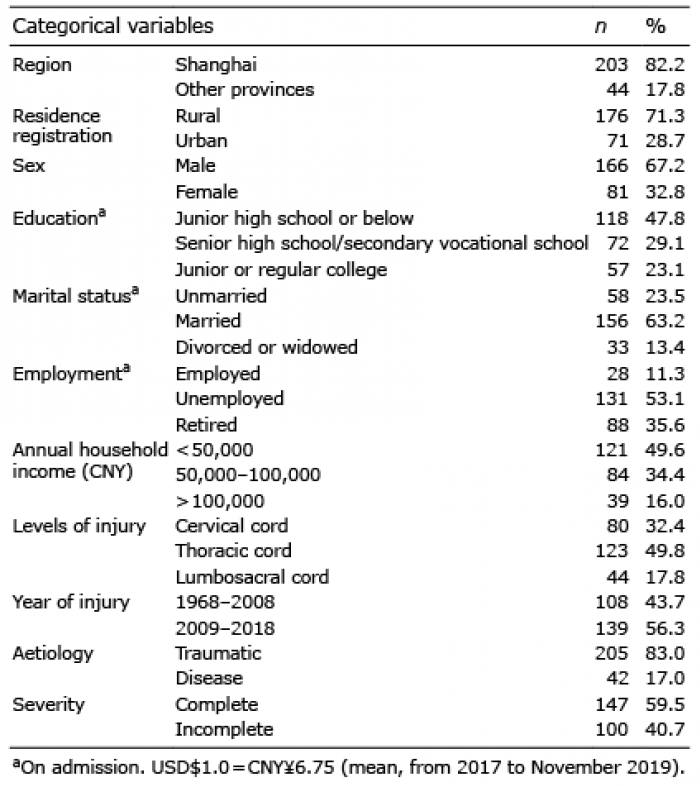
Inclusion criteria were: (i) age between 18 and 70 years, and (ii) had lived with the injury for at least one year. Adults with a congenital injury or cognitive impairment were ineligible. There were 266 individuals invited to complete the questionnaire between March 2017 and November 2019. Excluding 19 invalid questionnaires, the final sample of the study included 247 adults; 203 (82.2%) were from Shanghai, and 44 were from other provinces (Anhui Province 14; Jiangsu Province 7; Shandong Province 5; Jiangxi Province 4; Sichuan Province 3; Fujian Province 2; Zhejiang Province 2; other provinces 7). This study was approved by the ethics committee of the School of Public Health at Fudan University, Shanghai, China.
Data and measurement
The study’s design was cross-sectional. The data included the participants’ sex, age, region, type of residence registration (rural or urban), educational background, marital status, employment, annual household income, time of injury, cause of injury, level of injury, and its severity. The severity of the injury was defined as complete or incomplete. Marital status was classified as unmarried, married, divorced, or widowed. Levels of lesion were categorized into cervical, thoracic, and lumbosacral. The causes of injury were classified as traumatic and disease-induced. Information on annual household income was collected based on a single-choice question: “What is your annual household income (CNY)? (< 50,000; 50,000–100,000; > 100,000)”.
Quality of life
QoL was assessed with the WHOQOL Scales for people with physical disability (PD) (15). Tian found that the Chinese Version of the WHOQOL Scales was acceptable, reliable, and valid and could be used in the study of QoL in Chinese people with disability (16). The instrument comprised the local version of the WHOQOL-BREF plus the international WHOQOL-DIS add-on module (15, 17). The WHOQOL-BREF is an appropriate generic health-related quality-of-life measure for persons with SCI (18), and it has shown good reliability and validity in the SCI population (19). The Chinese version of the WHOQOL-BREF was introduced into mainland China in 1998 (17). The first 2 items of the WHOQOL-BREF evaluate general QoL and health, while the remaining 24 items, on a 5-point scale, could be classified into 4 domains: physical (7 items), psychological (6 items), social relationships (3 items), and environment (8 items). For each of these domains, summary scores were calculated and transformed to a 0–100 scale following the manual’s instructions (20), with low scores indicating poor QoL. Cronbach’s α of the WHOQOL-BREF was 0.934 in this study. The WHOQOL-DIS module is a scale added to the WHOQOL-BREF to assess the QoL of people with disabilities and comprises 12 items that function as a single overall domain plus one general item that assesses the overall impact of disability. Responses to each item were measured on a scale from 1 (not at all) to 5 (very much). A higher score reflected a higher QoL. The Cronbach’s α of the WHOQOL-DIS module was 0.802 in this study.
Anxiety and depression
Anxiety/depression was measured using the Zung Self-Rating Anxiety/ Depression Scale (SAS/SDS) (21, 22). The SAS/SDS is a 20-item inventory, with each item rated by the subject on a 4-point scale. The raw score multiplied by 1.25 is converted to a standardized score ranging from 25 to 100, with higher scores indicating more severe anxiety/depression. The standard score of 50/53 was regarded as the cut-off point for clinical significance of anxiety/depression (23, 24).
Community Integration Questionnaire
The Community Integration Questionnaire (CIQ) (25) has a total of 15 items across 3 domains: Home Integration (sum items 1–5), Social Integration (sum items 6–11) and Productivity (sum item 12 with the Job/School variable score based on items 13–15). The domains assess the level or frequency of involvement in a range of community activities including financial management, grocery shopping, childcare, meal preparation, housework, community access, social activities, employment, study, and volunteer work. Total score from the CIQ ranges from 0 to 29. Higher scores indicate better functioning in social integration and productivity. Liu et al. (26) reported Cronbach’s α for the total scale score was 0.8 in Chinese people with disabilities, and 1-month test-retest reliability was 0.92 for the total scale score, and between 0.89 and 0.95 for the subscales.
Statistical analyses
The descriptive analysis included the counts and percentages of the categorical variables, as well as the means of all numerical variables with standard deviations (SDs), median and range. The severity of anxiety/depression was classified as mild (50–59/53–62), moderate (60–69/63–72) and severe (≥ 70/≥ 73) by standard score (23, 24). Stacked bar charts were used to show the severity of anxiety and depression.
Mean WHOQOL-BREF domain scores were calculated and compared with the Guangzhou reference population (13) and reference values obtained from the original normative sample (23 countries) (27). WHOQOL-DIS module scores, excluding item 1, were calculated and compared with the Guangzhou reference population (16) and 58 people with SCI in Korea (28), a developed country in Northeast Asia with a GDP per capita in 2018 > USD$30,000. Multivariate linear regression models were applied to examine the factors related to QoL, which were measured by the 5 domain scores of the WHOQOL Scales. We included 15 independent variables in the regressions: region, residence registration, sex, age on admission, educational background, marital status, family income, employment, level of lesion, aetiology of lesion, severity, length of time since injury, anxiety, depression, and CIQ. Except for age on admission, length of time since injury, anxiety, depression, and CIQ, all other independent variables were defined as dummy variables. All statistical tests were 2-sided with a significant p-value < 0.05. The Statistical Package for Social Sciences for Windows (SPSS for Windows 13.0, SPSS Inc., Chicago, IL, USA) was used to perform descriptive statistics and multivariate linear regressions.
Participant characteristics
The majority of participants were from Shanghai and Guangzhou. Both in Shanghai and in Guangzhou, the per capita GDP in 2018 was more than USD$20,000, making it on the threshold of being equivalent to more developed economies. Among 247 people with cSCI who received rehabilitation training in SSRC, the male:female ratio was 2.05:1 (Table I). The mean age (SD) on admission was 49.4 years (SD 13.4). The mean age at injury was 36.5 years (SD 16.0). The mean length of time since their injury was 12.8 years (SD 13.8), and the range was 1–61 years. Among 148 respondents who had been employed before injury, only 16.9% who were of working age (male: < 60 years; female: < 55 years) was employed on admission. Demographic and injury characteristics of the study population in the SSRC are shown in Table I.
Table I. Demographic and injury characteristics of 247 people with chronic spinal cord injury (SCI)
Descriptive statistics
Means, SDs, medians, and ranges for measures of the variables are presented in Table II. The means of general QoL and overall health were 3.0 and 2.6, respectively. Of the participants 29.6% reported good and very good overall QoL, and 20.6% (51 participants) were satisfied with their health, while 45.3% were dissatisfied. The means of transformed scores for the 4 WHOQOL-BREF domains from low to high were as follows: physical 46.8, environmental 52.4, social 52.7, and psychological 56.0. The mean of the impact-of-disability item was 2.2, and the mean of the 12-item WHOQOL-DIS module was 38.7. 10.2% of the participants claimed that their disability had only a little negative effect on their day-to-day life, and only 1.7% (4 participants) claimed that the disability had no negative effect; 66.5%, however, reported either a mostly or a totally negative effect. The means of standardized scores for SAS and SDS were 47.8 and 53.3, respectively. The prevalence estimates for probable anxiety and depression were 44.6% and 52.7% (Fig. 1), respectively; among them, 4.5%/8.5% had severe anxiety/depression. As for the 3 variables measuring community integration, the means from high to low were social integration 6.4, family integration 3.5, and productivity 2.1, with the means of the total CIQ score being 12.1.
Table II. Descriptive statistics for quality of life (QoL), anxiety, depression, and community integration questionnaire (CIQ)
Fig. 1. Stacked bar charts showing the severity of anxiety and depression.
Comparative analysis
Table III shows the mean and SD of each domain of the WHOQOL Scales for the participants in this study, as well as the results from the Guangzhou population, 23 countries samples, and patients with SCI in Korea. Scores for the people with cSCI were 1.1–4.7 points less than those of the global samples across all WHOQOL-BREF domains; the score of the 12-item WHOQOL-DIS module for our sample was 1.2 points lower than that of Korean patients with SCI. Scores for the participants in this study were 0.7–3.1 points less than those for Guangzhou residents across the 3 WHOQOL-BREF domains, except for environmental health, which was a tenth point higher than that of the Guangzhou data; however, the score of the 12-item WHOQOL-DIS module for our sample was 4.1 points higher than that of Guangzhou patients with PD.
Table III. Dimensional scores of WHOQOL-BREF (score range 4–20) and WHOQOL-DIS module (score range 12–60), compared with other population data
Multivariate linear regression
To investigate how QoL was related to the socio-demographic, injury, psychological, and community integration variables, 5 separate multiple regression analyses were conducted. The score for each QoL domain was used separately as the dependent variable, and the potential related variables were entered as the predictors. The results showed that the region, whether or not the participants came from Shanghai, was not related with the QoL (p > 0.05). However, the urban people with cSCI had significantly lower social QoL (β = –0.17, p = 0.03) than the rural people with cSCI (Table IV). Females with cSCI had a higher social QoL score than males with cSCI (β = 0.21, p < 0.01). Further analyses showed that, after controlling for other relevant variables, individuals with a wealthier family background had significantly higher environmental QoL than did those with poorer backgrounds (β = 0.20, p = 0.01). Participants with a longer time from injury had significantly higher physical QoL than those with a shorter duration of SCI. Anxiety was a negative factor associated with physical, environmental, and the WHOQOL-DIS module QoL, whereas participants with higher SDS scores had lower scores in physical, psychological, and social QoL. Furthermore, a higher score of CIQ was a factor associated with higher physical and WHOQOL-DIS module QoL.
Table IV. Linear regression analyses of five domains of WHOQOL Scales for physical disabilities
QoL is an important outcome in SCI rehabilitation practice and research. This study describes the QoL profile of 247 people with cSCI in mainland China, which could enrich our knowledge of the condition of this vulnerable population.
Consistent with previous studies in China (29) and Australia (30), this investigation showed a significant decrease in the 3 domains of QoL of individuals with SCI, as measured by the WHOQOL-BREF compared with residents in reference areas in China. However, compared with the QoL of newly injured in-patients with SCI (31), our community participants, with a mean of 13 years injury history, reported higher QoL scores. As for the WHOQOL-DIS module, we found the participants had a few QoL scores lower than people with SCI in Korea and had higher QoL than people with PD in Guangzhou. The latter could be partly attributable to some persons in Guangzhou actually having one or more types of disabilities besides PD, and the people with multiple disabilities showed much lower QoL (16). Among the 4 domains of the WHOQOL-BREF, the physical QoL score in this study was the lowest. This finding was in agreement with the studies in Hong Kong (32), Tanzania (33) and Canada (34), which suggests that SCI has a greater impact on physical health than on mental, social, and environmental health.
With regard to physical health, the QoL of people with cSCI increases with the passage of time since injury. This finding is in line with previous investigation (8), but a prospective survey in Australia found the time span since injury was not a relevant factor (30). Of the participants 24.1% reported moderate or severe depression, as measured by SDS, and 17.0% showed moderate or severe anxiety, as measured by SAS. This suggests that, though many years may have passed since injury onset, anxiety and depression are still serious problems for people with SCI (35) and are negatively correlated with their QoL (12), underscoring the importance of treatments for psychological problems after SCI (36). More research is needed to understand why urban people with cSCI had lower scores in the social domain than those of rural people with cSCI. The possible reason would be that interpersonal and community relationships are more numerous and/or tighter in small communities, where knowing your neighbours is easier both due to community smallness and due to relatively less population movement/turn-over. Thus, with time, someone with all the limitations of a SCI will reconnect him-/herself into those social and community circles in ways that are suited to their new, altered functional capacities. The mobility and greater degree of personal anonymity (i.e. weakening of relationship bonds) of urban areas prevents this happening as readily. Women with cSCI reported higher social scores than men with cSCI, a gender disparity that has been found in other studies (37–39).
Community integration is a primary objective for rehabilitation programmes focused on SCI (40). The current study found that community integration was a positive factor associated with physical (30) and WHOQOL-DIS module QoL. However, literature review found that the CIQ score of Chinese adults with cSCI was lower than that of community-dwelling adults with SCI in Australia (41) and Bangladesh (42). More active interventions are needed to improve community integration among individuals with cSCI (43).
Our results via multivariate analysis revealed that 7 demographic (age, marital status, education background, and employment) and injury characteristic (level, severity, and aetiology) variables were not predictors of QoL in people with SCI in mainland China. An Indian study identified age, education, and marital status as not being associated with QoL scores, but employment was associated with higher scores of QoL (44). Qiu et al. (37) showed that married persons with 1–2 months SCI history showed lower social and psychological QoL than that of unmarried people. Wang et al. reported that level of lesion was not correlated with QoL in China (12). People with a higher injury level and individuals with a complete injury reported lower physical QoL in European rehabilitation centres during the first 2 years post-injury, younger persons had higher psychological QoL, and aetiology was not a factor related to QoL (8). Barker et al. (30) found that neurological level and age were not associated with QoL. However, Pentland et al. (45) discovered that age was a positive factor to more overall life satisfaction. A review (46) reported that among persons with SCI, there were conflicting effects of age, employment status, marital status, and educational level on QoL, with an unclear impact of injury completeness or injury level on QoL. In general, the relationship between some demographic and injury characteristics with QoL deserves further study.
The QoL of people with cSCI in mainland China was relatively low, and our findings suggest multiple ways to improve it in this vulnerable target population: First, more family income could bring higher environmental QoL. Therefore, more efforts should be made to help people with SCI to return to work, which could both facilitate community integration and improve family income, thus helping to improve their QoL (47). Secondly, it is essential to establish a surveillance system to collect comprehensive data about such issues as QoL in routine healthcare systems (48), which would provide important information for physicians and policy-makers. Thirdly, the physical health of newly injured people with SCI needs more attention from healthcare providers and communities. Last, but not least, the barrier-free environment in mainland China is still limited, which creates an obstructive environment for using wheelchairs in homes and communities. To promote community integration, it is essential to accelerate the construction of a barrier-free environment and housing to help wheelchair-dependent citizens reintegrate into their families and society.
The study has a few limitations. First, the sample size was limited due to the relatively low incidence of SCIs and the limited service capacity of the SSRC training centre. Therefore, the factors without significance in this study should not be excluded in future research, as this may be an artefact of the small sample size. Secondly, the big challenge was the comparability of our results with “reference data”. Extra caution should be used when interpreting these comparisons. Thirdly, the ASIA (American Spinal Injury Association) Impairment Scale (AIS) grade (49) was not collected. Finally, this study design was only a cross-sectional study without follow-up. A more rigorous study design, such as a cohort study, should be implemented to evaluate the long-term effects of interventions on QoL (50).
In summary, this study evaluates the QoL, anxiety, depression, and community integration of adults with cSCI in mainland China. Our results suggest that the QoL of people with cSCI, as measured by the WHOQOL-BREF, is lower than that of the reference population. Meanwhile, the score measured by the 12-item WHOQOL-DIS module was slightly lower than that of the Korean reference group. Men or urban adults with cSCI had lower social QoL than female or rural people with cSCI. Higher family income was associated with higher environmental QoL. Duration of SCI was a positive factor in the physical health of adults with SCI, while anxiety and depression were negative factors associated with QoL in the same population. Community integration improvement was correlated with better physical and WHOQOL-DIS module QoL. Therefore, policymakers should allocate more resources to help improve the QoL of people with cSCI in mainland China.
The authors thank the SSRC for their help collecting data. This work was supported by the National Natural Science Foundation of China [71673052], China Scholarship Council [201506105030], Shanghai Pujiang Program of Shanghai Municipal Human Resources and Social Security Bureau [17PJC003], the 111 Project [Grant Number B16031], a major project of the National Social Science of China [No.17ZDA078], and a first-class discipline construction of public health and preventive medicine from the pilot construction of high-level local universities in Shanghai Medical College at Fudan University.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize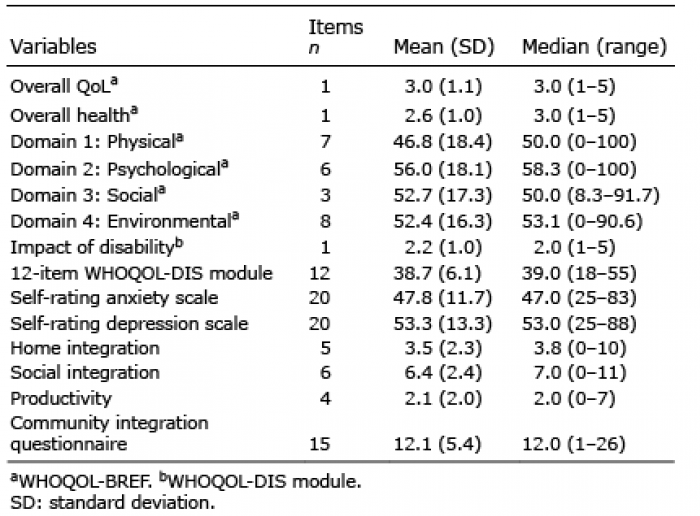 Click to show fullsize
Click to show fullsize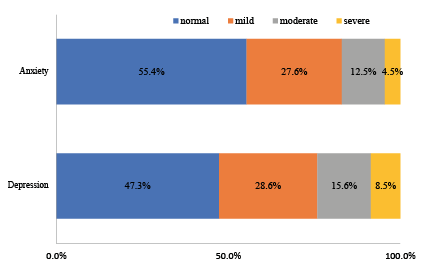 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize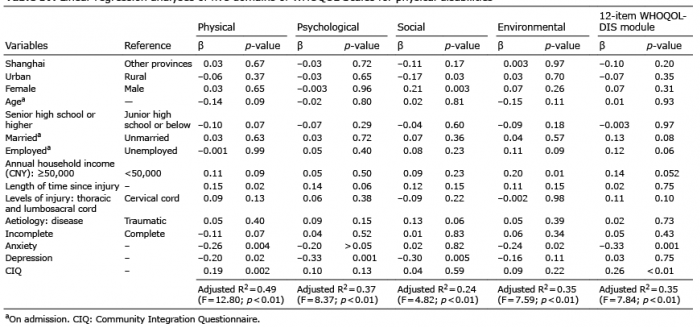 Click to show fullsize
Click to show fullsize