
From the 1Neuromotor and Cognitive Rehabilitation Research Center, Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona and 2Neurorehabilitation Unit, Hospital Trust of Verona, Verona, Italy
Objective: To evaluate the role of diagnostic nerve block in predicting the outcome of subsequent botulinum toxin type A treatment for spastic equinovarus foot due to chronic stroke.
Design: Retrospective observational study.
Patients: Fifty chronic stroke patients with spastic equinovarus foot.
Methods: Each patient was given diagnostic tibial nerve block (lidocaine 2% perineural injection) assessment followed by botulinum toxin type A inoculation into the same muscles as had been targeted by the nerve block. All patients were evaluated before diagnostic nerve block, after the nerve block, and 4 weeks after botulinum toxin injection. Outcomes were ankle dorsiflexion passive range of motion of the affected side, and calf muscle spasticity, measured with the modified Ashworth scale and the Tardieu Scale.
Results: Significant improvements were measured after diagnostic nerve block and botulinum toxin injection compared with the baseline condition. Diagnostic nerve block led to significantly greater improvements in all outcomes than botulinum toxin injection.
Conclusion: This study confirmed diagnostic nerve block as a valuable screening tool in deciding whether to treat spastic equinovarus with botulinum toxin. However, the results support the evidence that diagnostic nerve block results in a greater reduction in muscle overactivity than does botulinum toxin type A in patients with spastic equinovarus due to stroke.
Key words: botulinum toxin; diagnosis; equinus deformity; muscle spasticity; nerve block.
Accepted May 7, 2020; Epub ahead of print May 20, 2020
J Rehabil Med 2020; 52: jrm00069
Correspondence address: Alessandro Picelli, Neuromotor and Cognitive Rehabilitation Research Center, Physical and Rehabilitation Medicine section, Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona. P.le L.A. Scuro, 10. 37134 Verona, Italy. E-mail: alessandro.picelli@univr.it
This study reviewed data from 50 chronic stroke patients with spastic equinovarus foot in order to compare the outcome of tibial nerve (main trunk and motor branches) diagnostic block (which temporarily relieves focal muscle overactivity, allowing assessment of the contribution of different muscles) with that of subsequent botulinum toxin injected into the same muscles as were targeted by the nerve block. Outcome measures were passive motility of the affected ankle and overactivity of the calf muscles. All patients were evaluated before and after the nerve block, and 4 weeks after the botulinum toxin injection. Significant improvements were found both after the nerve block and after botulinum toxin injection in comparison with the baseline condition; however, the improvements observed after nerve block were significantly greater. These results confirm that diagnostic nerve block is a useful screening tool for use before botulinum toxin treat-ment, although less improvement occurred after botulinum toxin injection compared with after nerve block.
Botulinum toxin type A (BoNT-A) is an effective and safe first-line treatment for lower limb spastic muscle overactivity post-stroke (1). Spastic equinovarus foot is the pattern most commonly treated with BoNT-A in patients with lower limb spastic muscle overactivity (2). Spastic equinovarus foot after stroke has the following main causes: calf muscle spasticity; spastic calf muscle contracture/shortening; ankle dorsiflexor muscle weakness leading to drop-foot during the swing phase of gait; imbalance between the tibialis anterior and peroneus muscles (3).
Diagnostic nerve block (DNB) transiently relieves focal muscle hypertonia (4). It allows the differentiation of spastic muscle overactivity from contracture, determination of the respective role of different muscles in patterns of overactivity, and testing of the strength of antagonist muscles (3–5). Thus, DNB of the tibial nerve and its motor branches is recommended to determine the causes of spastic equinovarus foot and define its most appropriate therapeutic management (3).
Treatment with BoNT-A is indicated in patients with a notable/complete correction of spastic equinovarus foot in the swing and stance phases of gait after tibial nerve (main trunk and motor branches) DNB (3). However, from a clinical point of view, even though selective DNB of the tibial nerve motor branches represents a key way to identify which muscles to inject with BoNT-A, it may be challenging to replicate the outcome of DNB by means of BoNT-A injection (6). This must be considered together with the major causes of loss of BoNT-A response in patients with spastic muscle overactivity (i.e. inaccurate selection and identification of the correct muscle for injection, insufficient drug dosage, inadequate injection technique, development of changes in the muscle, and formation of neutralizing antibodies) (7).
Although DNB is suggested to predict the effects of treatment for muscle hypertonia by simulating its outcome (3, 4), to the best of our knowledge no previous study has compared the effects of DNB and BoNT-A injection. Conversely, this issue has been investigated previously by Deltombe and colleagues with regard to selective tibial neurotomy (8). This permanent neurosurgical procedure showed equal efficacy to DNB of the tibial nerve for treating spastic equinovarus foot in hemiplegic patients (8). Thus, DNB has been suggested as a valuable screening tool prior to neurotomy. The main aim of this study was to evaluate the role of DNB in predicting the outcome of BoNT-A treatment for spastic equinovarus foot due to chronic stroke.
This single-centre, retrospective (chart review), observational study analysed data from 50 chronic stroke patients with spastic equinovarus foot, who had undergone BoNT-A injection into the spastic calf muscles after tibial nerve DNB at our clinical Neurorehabilitation Unit, from January 2016 to December 2019.
Inclusion criteria were: age over 18 years; spastic equinovarus foot consequent to first-ever unilateral ischaemic or haemorrhagic stroke (documented by a computerized tomography scan or magnetic resonance imaging; subarachnoid haemorrhage excluded); calf muscles spasticity graded at least 2 on the Modified Ashworth Scale (MAS) (9); at least 6 months since stroke onset; notable/complete relief of spastic equinovarus foot after tibial nerve (motor branches and main trunk) DNB; spasticity pattern involving at least one of the following muscles: soleus, tibialis posterior, gastrocnemius medialis and gastrocnemius lateralis (10).
Exclusion criteria were: participation in other trials; spasticity pattern involving the following muscles: flexor digitorum longus, flexor digitorum brevis, flexor hallucis longus and extensor hallucis longus (10); previous treatment of spastic equinovarus foot with neurolytic or surgical procedures; other neurological or orthopaedic conditions involving the affected lower limb.
All participants were outpatients. All patients provided informed consent for data extraction from chart review, as needed. The study was carried out according to the principles of the Declaration of Helsinki and was approved by the local Review Board.
Treatment procedures
According to our clinical practice, the affected leg of all patients was evaluated by serial selective DNB of tibial nerve motor branches (the DNB was performed first at the soleus motor nerve branch followed, in the case of no or scant relief of muscle overactivity, by the motor nerve branch to the tibialis posterior, to the gastrocnemius medialis and to the gastrocnemius lateralis muscles). If necessary, the DNB was finally performed at the tibial nerve main trunk (mixed sensorimotor nerve block) (8). Patients lay in the prone position with their legs outstretched during the whole procedure. A 22-gauge, 80-mm, ultrasound faceted tip echogenic needle for nerve block (SonoPlex STIM, Pajunk, Geisingen, Germany) was guided to the tibial nerve (motor branches and main trunk) by means of ultrasonography (MyLab 70 XVision, Esaote, Genoa, Italy) and electrical nerve stimulation (Plexygon ,Vygon, Padua, Italy). Anatomical landmarks were used for linear transducer (scanning frequency 15 MHz) and needle tip positions (11). Once tibial nerve (motor branches or main trunk) was identified by means of ultrasonography, following elicitation of appropriate muscular response to a 1 Hz, 100 μs, 0.5 mA electrical stimulus, lidocaine 2% was injected (1–2 ml for each motor nerve branch blockade and 5–6 mL to block the main nerve trunk; no more than 10 mL in total per session). Gentle aspiration was performed before lidocaine injection to ensure the absence of vessels at the needle tip.
Once the spastic equinovarus pattern had been defined by tibial nerve (motor branches and main trunk) DNB, each patient was given ultrasound-guided BoNT-A inoculation into the spastic calf muscles. Only the muscles targeted for injection by DNB were treated (namely soleus and/or tibialis posterior and/or gastrocnemius medialis and/or gastrocnemius lateralis; see inclusion/exclusion criteria) (12). Thus, BoNT-A treatment was tailored to each patient on the basis of DNB outcome. BoNT-A treatment features (injected muscles, toxin brand, dose, dilution, injection sites) were defined for each patient according to our daily clinical practice, which is line with the local regulatory and European guidelines (7). Our chart did not record information about the prescription or execution of adjuvant treatment (e.g. electrical stimulation, casting, taping or physiotherapy) in the period between BoNT-A treatment and after injection evaluation with DNB (13).
Evaluation procedures
All patients were evaluated before DNB, after DNB, and 4 weeks after BoNT-A treatment. Patients remained in the supine position with their knees extended during evaluations. The spastic ankle dorsiflexion passive range of motion (PROM) was measured using a handheld goniometer. The sensitivity of the measurement was set at 5°. The dorsiflexion angle was defined as positive and the plantar flexion angle as negative, taking 0° as the neutral position of the joint (14). The MAS is a 6-point scale grading the resistance of a relaxed limb to rapid passive stretch (0=no increase in muscle tone; 1 = slight increase in muscle tone at the end of the range of motion; 1+ = slight increase in muscle tone through less than half of the range of motion; 2 = more marked increase in muscle tone through most of the range of motion; 3 = considerable increase in muscle tone; 4 = joint is rigid) (9). For statistical purposes, a score of 1 was considered as 1, a score of 1+ was considered as 2 and so on, up to a score of 4, which was considered as 5. The MAS was used to evaluate spastic calf muscles tone. The Tardieu Scale was used to evaluate spastic calf muscle tone according to the Tardieu Scale spasticity grade, which measured the gain in muscle reaction to fast stretch in dorsiflexion from (0: no resistance throughout passive movement; 1: slight resistance throughout passive movement; 2: clear catch at a precise angle, interruption of the passive movement, followed by release; 3: fatigable clonus occurring at a precise angle; 4: unfatigable clonus occurring at a precise angle), and the Tardieu Scale spasticity angle, which measured the difference (a – b) between the angle of catch-and release/clonus at fast stretch in (b) dorsiflexion and (a) ankle dorsiflexion PROM (15).
Statistical analysis
Statistical analysis was performed with the Statistical Package for Social Science for Macintosh, version 26.0 (SPSS Inc., Armonk, NY, USA). Descriptive statistics were used for demographic and clinical features of our sample. The paired sample t-test was performed to compare the outcome of DNB and BoNT-A treatment with the baseline (before DNB evaluation). The alpha level for significance was set at p < 0.05. Bonferroni correction for multiple comparisons was applied, resulting in p < 0.016 as the significance threshold.
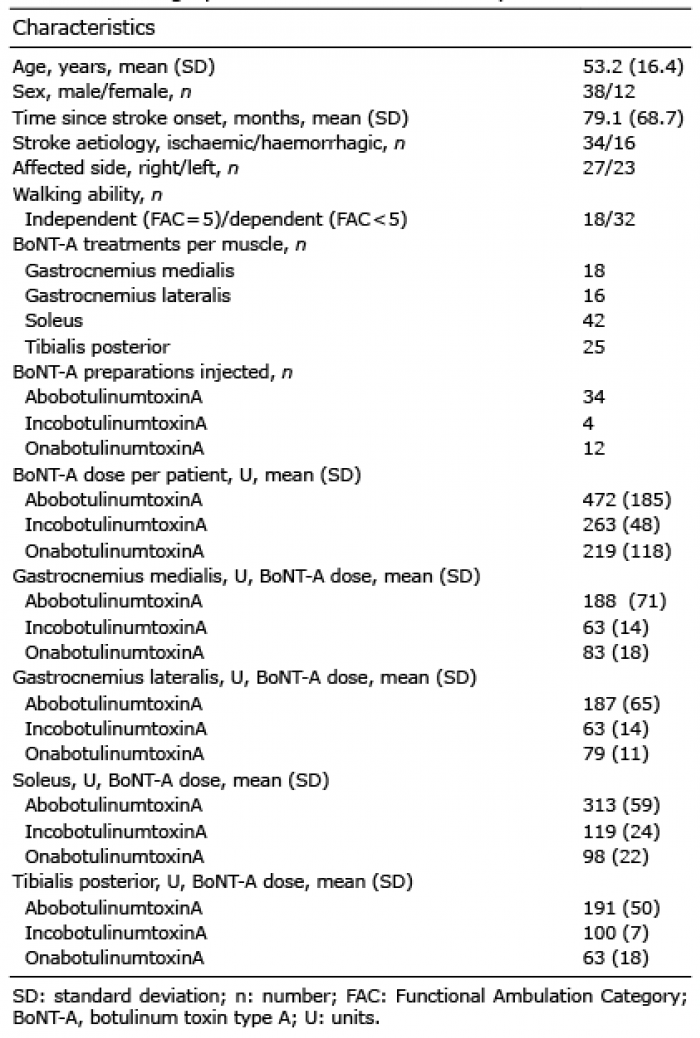
Demographic and clinical features of patients are reported in Table I.
Comparison of pre-DNB vs post-DNB conditions revealed significant improvements after DNB in ankle PROM (t49 = –10.128; p < 0.001) and calf muscle spasticity on the MAS (t49 = 11.523; p < 0.001), Tardieu Scale spasticity grade (t49 = 7.849; p < 0.001) and Tardieu Scale spasticity angle (t49 = 6.325; p < 0.001). Comparison of pre-DNB vs post-BoNT-A injection conditions showed significant improvements after BoNT-A injection in ankle PROM (t49 = –3.665; p = 0.001) and calf muscle spasticity on the MAS (t49 = 6.654; p < 0.001), Tardieu Scale spasticity grade de (t49 = 7.134; p < 0.001) and Tardieu Scale spasticity angle (t49 = 3.317; p = 0.008). Comparison of post-DNB vs post-BoNT-A injection conditions showed significant differences in favour of the post-DNB condition with regard to ankle PROM (t49 = 6.157; p < 0.001) and calf muscle spasticity on the MAS (t49 = –4.810; p < 0.001), Tardieu Scale spasticity grade (t49 = –3.383; p = 0.001) and Tardieu Scale spasticity angle (t49 = –3.960; p = 0.002). Table II shows the clinical features of the patients with spastic equinovarus foot and the results of the comparisons.
Table I. Demographic and clinical features of patients
Table II. Clinical features of spastic equinovarus foot and comparisons
Selective DNB of the tibial nerve and its motor branches is mandatory in order to evaluate and define the management of spastic equinovarus foot due to stroke (3, 6, 8, 16). The effectiveness of DNB indicates muscle overactivity as the “main problem”, supporting the use of a drug treatment (such as BoNT-A) and helping the detection of muscles to inject (6). Our findings are in line with this view. Indeed, we observed that BoNT-A injection into those muscles targeted by DNB of the tibial nerve (motor branches and main trunk) led to a significant improvement in spastic equinovarus foot by 4 weeks after treatment. Hence, this study further confirmed tibial nerve DNB as a valuable screening tool in decisions about treating spastic equinovarus foot with BoNT-A. Interestingly, both DNB and BoNT-A improved all outcomes (ankle PROM and calf muscle tone), which assessed both neural and non-neural components of spastic muscle overactivity. Although our patients with stroke were long-term chronic patients (mean time from onset 6.5 years), this study only included people with notable/complete relief of spastic equinovarus foot after tibial nerve (motor branches and main trunk) blockade. Hence, our patients had no clinically relevant contracture. On this basis, our findings are in line with the current literature, which reported improvements in passive joint motion and muscle tone after BoNT-A administration in patients with spastic muscle overactivity due to stroke (1, 17). Nonetheless, our personal experience suggested that it is not easy to obtain a similar outcome after DNB and BoNT-A injection. This is the main reason for this retrospective study, which aimed to evaluate whether the outcome of BoNT-A treatment might be predicted by tibial nerve DNB in chronic stroke patients with spastic equinovarus foot. The current findings showed that DNB led to a significantly greater reduction in muscle overactivity than BoNT-A treatment. Thus, our clinical impression about the challenge to replicate DNB outcome with BoNT-A injection is confirmed.
Therapeutic management of spastic equinovarus foot may include focal treatment with drugs (BoNT-A injection and neurolysis with phenol or alcohol), rehabilitation procedures (physiotherapy, muscle strengthening and stretching, taping, casting, orthosis, functional electrical stimulation, physical modalities) and surgical approaches (selective neurotomy, tendon transfer and tendon lengthening) (3, 13). Our clinical experience in this field is in line with the Mont-Godinne interdisciplinary guidance, which considers the DNB of tibial nerve (main nerve trunk and motor branches) as the central point of a pathway for assessing and planning the management of spastic equinovarus foot in patients with stroke (3). Neural blockade with anaesthetics is a safe, low-cost, simple diagnostic tool to obtain a fast (few minutes) suppression of muscle overactivity, which may last for several hours depending on the anaesthetics used (e.g. lidocaine 2% or bupivacaine 0.5%) (2, 3, 8). Regarding stroke patients with spastic equinovarus foot, DNB and selective neurotomy (surgical partial section of selected motor nerve branches) were found equally to reduce muscle overactivity as a consequence of their similar action upon Ia fibres (which mediate the myotatic reflex) and alpha motor fibres (which mediate voluntary contraction) (8). On the other hand, despite the fact that BoNT-A is the focal treatment for muscle hypertonia with the highest level of evidence (level A), it has been found inferior to selective neurotomy for reducing muscle overactivity in patients with spastic equinovarus foot (1, 16). Based on similar reasoning, we decided to compare the effects of DNB and BoNT-A injection. The results of the current study showed a lower reduction in spastic muscle overactivity after BoNT-A injection (compared with DNB), taking into account some of the main causes of non-response (i.e. DNB allowed us to correctly define the pattern of muscle overactivity and excluded clinically relevant contracture, and BoNT-A was properly injected into the overactive muscles by means of ultrasound) and according to the international consensus (7). On the other hand, despite the dosage of BoNT-A was defined according to the local regulatory, one may argue that it was insufficient to reach the same effect of DNB. This may be considered as a limitation of this study. Current evidence from the literature suggests that doses of BoNT-A higher than labelled ones are effective in reducing spasticity of the upper and lower limbs after stroke. Furthermore high doses of BoNT-A appear to be safe, with low occurrence of mild adverse effects (18, 19). However, to date, the administration of high-dose BoNT-A has been debated mainly in terms of maximum dose per treatment session in order to allow the injection of a larger number of muscles (18, 19) in multilevel treatments. Less is known about the maximum dose per muscle in relation to the total body dose. Future research should improve our knowledge about this issue. Other limitations of this study are as follows. First, we did not include a control group to assess the importance of muscle targeting by means of DNB for the success of BoNT-A injection into the posterior calf muscles. Secondly, the design of this study was retrospective, thus there was no standardization of our patients before and after interventions. Thirdly, our patients were evaluated at one month after a single BoNT-A treatment. Thus, we cannot draw conclusions about the clinical condition of our patients later in the same injection cycle or about how many BoNT-A injection cycles are needed to obtain improvements similar to those observed after DNB. Fourthly, we did not consider an outcome measure more related to spastic co-contraction and active function, such as ankle dorsiflexion active range of motion. Fifthly, even if our charts did not report the prescription or execution of adjuvant treatments after BoNT-A injection, considering the retrospective design of this study, we cannot be sure about the activities performed by our patients after BoNT-A injection. Moreover, we cannot infer about the add-on effect of adjuvant therapies to gain improvement similar to DNB after BoNT-A treatment (13). Sixthly, no functional (e.g. motion analysis) and neurophysiological (e.g. electromyography) evaluation was performed to assess improvements after DNB and BoNT-A injection.
In conclusion, this study confirmed DNB as a valuable screening tool in making decisions about treating spastic equinovarus foot with BoNT-A. However, the results support the evidence that DNB allows a greater reduction in muscle overactivity than BoNT-A in patients with spastic equinovarus due to stroke. To improve these observations, larger scale prospective studies are needed, taking into account (and overcoming) the limitations reported above.


 Click to show fullsize
Click to show fullsize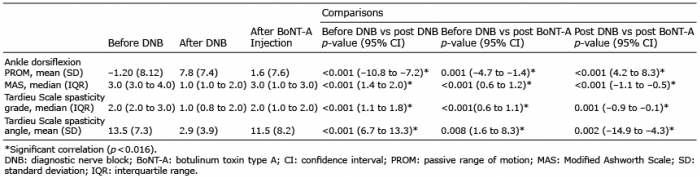 Click to show fullsize
Click to show fullsize