
From the 1Université Catholique de Louvain, Secteur des Sciences de la Santé, Institut de Recherche Expérimentale et Clinique, NeuroMusculoSkeletalLab (NMSK), 2Cliniques Universitaires Saint-Luc, Service de médecine physique et réadaptation, Brussels, Belgium, 3Neurology Department, Federal State Hospital Treatments and Rehabilitation Center of the Ministry of Health and Social Development of the Russian Federation, Moscow, Russia, 4Department of Palliative Care, Policy and Rehabilitation, Florence Nightingale Faculty of Nursing, Midwifery and Palliative Care, King’s College London, 5Regional Hyper-acute Rehabilitation Unit, Northwick Park Hospital, London, UK, 6Ipsen Bioscience, Cambridge, MA, USA, 7Ipsen Pharma, Boulogne-Billancourt, 8Université de Reims Champagne-Ardenne, Hôpital Sébastopol, Centre Hospitalier Universitaire de Reims, Physical Medicine and Rehabilitation Department, Reims, France, 9,10See study group lists in supplementary materials
Objective: To compare patients with upper limb spasticity who did or did not receive abobotulinumtoxinA (Dysport®) in shoulder muscles during 2 international clinical studies.
Design: Phase 4 Upper Limb International Spasticity Study-II (ULIS-II; NCT01020500) endpoints: primary goal selection and achievement. Phase 3 Adult Upper Limb (AUL) open-label study (NCT01313299) endpoints: Disability Assessment Scale principal target of treatment and mean (standard deviation) change from baseline to week 4 (last cycle involving shoulder muscles) for pain, Modified Frenchay Scale (active function), and Tardieu Scale parameters.
Patients: Shoulder population: patients receiving abobotulinumtoxinA injections in shoulder muscles (n = 82 and n = 96 in ULIS-II and AUL open-label study, respectively); non-shoulder population: patients not injected in shoulder muscles (n = 239 and n = 158, respectively).
Results: ULIS-II: primary treatment goal was pain in 25.6% vs 8.4% patients (3-fold higher) in shoulder vs non-shoulder populations, with high goal-achievement for pain reduction (85.7%). AUL open-label study: Disability Assessment Scale pain selection was 9.5% vs 5.1% (almost double); pain improvements were –0.7 (0.9) vs –0.4 (0.7); active function improvements were +0.60 (0.80) vs +0.33 (0.79), in shoulder vs non-shoulder populations, respectively. Tardieu scale parameters were improved.
Conclusion: High goal achievement rates for pain reduction and improved active function were observed in patients receiving abobotulinumtoxinA in shoulder muscles.
Key words: botulinum toxins, type A; abobotulinumtoxinA; muscle spasticity; shoulder joint; shoulder pain; observational study; clinical trials, phase III.
Accepted May 13, 2020; Epub ahead of print May 25, 2020
J Rehabil Med 2020; 52: jrm00068
Correspondence address: Thierry Lejeune, Médecine Physique et Réadaptation, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Avenue Hippocrate 10, 1200 Woluwe-Saint-Lambert, Brussels, Belgium. E-mail: thierry.lejeune@uclouvain.be
Botulinum toxins, such as abobotulinumtoxinA, are used to treat spasticity (muscle overactivity) in arm muscles. Spasticity in shoulder muscles occurs in many patients following a stroke. Shoulder spasticity can be painful and limit limb movement. This paper compares the results from patients who did and those who did not receive abobotulinumtoxinA injections in shoulder muscles (among other arm muscles) in 2 studies. In both studies, the results showed that more patients receiving treatment in shoulder muscles chose pain as a key goal for treatment and had reduced pain following treatment compared with patients not treated in the shoulder. In addition, patients receiving shoulder injections showed further improvement in arm movement compared with those not receiving shoulder injections. Overall, these results suggest that abobotulinumtoxinA treatment in shoulder muscles may improve outcomes for patients with arm spasticity involving the shoulder.
Spasticity and pain in the shoulder are common in patients with hemiplegia after stroke or traumatic brain injury (TBI) (1–3), negatively impacting quality of life (1). Shoulder spasticity develops in approximately 58% of patients who have experienced stroke, of whom 60% experience shoulder pain (4). An association has been observed between the degree of shoulder spasticity and pain, and both can contribute to hemiparetic patients’ functional impairment, affecting balance, walking and self-care activities (2, 5). Range of motion in the joint can also be impeded, reducing hand function and limiting patients’ abilities to perform daily activities (1–3). Furthermore, shoulder spasticity has the additional burden of impeding patients’ ability to complete occupational therapy and physiotherapy, hindering recovery (1, 6).
AbobotulinumtoxinA (Dysport®) has been demonstrated to be effective in the treatment of adult spasticity in the upper extremity (7) and is licensed for use in the shoulder muscles (8). However, there are limited data in the literature investigating the impact of BoNT-A treatment in patients with upper limb spasticity (ULS) requiring injection in the shoulder muscles, with the available data focusing predominantly on shoulder pain, rather than function (9, 10). The evidence, though limited, indicates an important role for reducing pain and functional impairment related to shoulder spasticity with BoNT-A; however, findings are not consistent and sample sizes are small (11–17).
It has been shown previously that the location of BoNT injections across proximal and distal muscles in patients with upper limb spasticity were largely selected based on injector beliefs and ease of access to the muscle, rather than patient goals, patient characteristics and their degree of spasticity (18). This highlights the need to better inform clinicians about how to use BoNT-A in shoulder muscles to better address patients’ needs.
In recent years, there have been 2 large clinical studies in patients with ULS receiving abobotulinumtoxinA in which some patients received injections in their shoulder muscles. The phase 3 AUL open-label, extension study (Adult Upper Limb; NCT01313299) analysed the effect of single and repeated injections of abobotulinumtoxinA into muscles of the upper limb, which included shoulder extensors and internal rotator muscles. Improvements were observed in active movements, and perceived and active function (19). The Phase 4 observational ULIS-II study (Upper Limb International Spasticity Study-II; NCT01020500) quantified and characterized patient-centred goal achievements following one abobotulinumtoxinA injection, and demonstrated that approximately 80% of patients reached their treatment goals (20, 21).
The ULIS-II and AUL studies provide large data sets, enabling the investigation of outcomes among the subset of patients who received shoulder injections. The aim of the present analyses was to investigate whether the outcomes of patients receiving abobotulinumtoxinA in shoulder muscles differed from those who did not receive shoulder muscle injections. We report here baseline demographics and goal-setting data, as well the effects of abobotulinumtoxinA injection on patient outcomes, including goal attainment, pain and function, from patients in these 2 studies. Dosing information is also presented to inform treating physicians.
The methodology and primary outcomes of the ULIS-II and AUL open-label studies have been published previously (19–21).
The complementary analyses undertaken here compared the sub-populations of patients who received injections in their shoulder muscles (shoulder population) with those who did not receive injections in their shoulder muscles (non-shoulder population). These analyses concerned the prioritization and achievement of treatment goals (ULIS-II study only), as well as improvements in pain on the Disability Assessment Scale (DAS) (22) and Tardieu Scale parameters (23, 24), including passive range of motion (XV1), angle of catch (XV3) and spasticity angle (X; AUL open-label study only).
Study design and treatment
ULIS-II was a Phase 4, international, 18-month, observational, prospective, before-and-after study, conducted at 84 sites in 22 countries within Europe, Pacific Asia, Eastern Europe and South America (20). Therapies were administered in accordance with routine local clinical practice. At baseline (Visit 1), patients received a single injection cycle of any licensed BoNT-A product, as selected by the investigator. The follow-up (Visit 2) was between 3 and 5 months post-injection. Injection doses, injection points (including shoulder injections) and volume per injection point were determined by the investigator. Only patients who received abobotulinumtoxinA injections during ULIS-II were analysed here.
The AUL open-label study (19) was an extension of a Phase 3, international, single-cycle, randomized, double-blind study (25), in which patients received up to 4 additional abobotulinumtoxinA treatment cycles at least 12 weeks apart over 1 year. The open-label phase included rollover patients from the double-blind study and newly recruited patients. Patients were enrolled at 34 sites in 7 countries across Europe and in the USA. At Cycle 1, all patients received 1,000 U abobotulinumtoxinA, or 500 U, at the investigator’s discretion if patients had experienced a treatment emergent adverse event (TEAE) during the double-blind cycle. From Cycle 2 onwards, patients could receive injections into shoulder muscles if deemed appropriate by the investigator, at a maximum dose of 500 U per cycle, with up to 1,000 U injected across other upper limb muscles.
For both studies, written informed consent was obtained from all patients prior to study entry. The AUL open-label study was performed in compliance with the Declaration of Helsinki. As a non-interventional study, ULIS-II did not fall under the scope of Declaration of Helsinki and was conducted in compliance with Guidelines for Good Pharmacoepidemiology Practices.
Patients (eligibility criteria)
In brief, patients included in ULIS-II were adults (≥ 18 years) with post-stroke ULS, for whom a decision had already been made to inject BoNT-A and who had not received BoNT treatment within 12 weeks prior to enrolment.
In the AUL open-label study, patients were adults (aged 18–80 years, inclusive) with hemiparesis who had experienced a stroke or TBI at least 6 months previously; efficacy of BoNT-A in patients with TBI has been previously shown to be consistent with results observed with the overall population (26). Patients were required to have met set minimum criteria for assessments of spastic paresis, including a Modified Ashworth Scale (MAS) score ≥ 2 or 3 in the primary target muscle group (PTMG) for patients naïve or non-naïve to BoNT-A, respectively; and a DAS score ≥ 2 in the principal target of treatment, as a measure of perceived function and pain. Further details of inclusion and exclusion criteria have been published previously (19–21).
The post-hoc analyses presented here compared patients in the ULIS-II or AUL open-label studies who received abobotulinumtoxinA injections into at least one shoulder muscle with those who did not receive shoulder injections.
Functional assessments
The primary objective of the ULIS-II study was to assess the responder rate, defined by the achievement of primary goals from goal attainment scaling (GAS), following one BoNT-A injection cycle (21). GAS was applied using the GAS-light method (27). The main outcome measures for this analysis were the selection and achievement of primary goals in patients who received abobotulinumtoxinA. As a result of the observational nature of the ULIS-II study, related adverse events (AEs) only, were reported.
In the AUL open-label study, the primary objective was the safety of repeated treatment cycles with abobotulinumtoxinA over 1 year (19). TEAEs were spontaneously reported or identified following direct questioning. Functional outcome measures included in this analysis were the selection of the primary target for treatment on the DAS, mean changes from baseline to week 4 of each treatment cycle and the last cycle to include shoulder muscles for pain on the DAS (assessed as intensity of pain or discomfort related to upper-limb spasticity) and active function (Modified Frenchay Scale [MFS] score) (28). Mean changes from baseline to week 4 for the last injection cycle to include shoulder muscles were also assessed for Tardieu Scale parameters, including XV1, XV3 and X. Details of these outcome measures have been described previously (19). For rollover patients in the open-label, extension study, baseline was defined as baseline of the double-blind study.
Statistical analyses
Data are presented for the sub-populations of patients from either the ULIS-II or AUL open-label study who received at least one abobotulinumtoxinA injection into a shoulder muscle (shoulder population) and those who did not receive shoulder injections during the study (non-shoulder population). The respective studies were not powered to investigate the significance of findings in these sub-populations; as such, all analyses presented here are descriptive and exploratory. Safety data from each study are presented descriptively.
ULIS-II study
Patients. In ULIS-II, of the 321 patients injected with abobotulinumtoxinA in the upper limb muscles (finger, wrist, elbow and/or shoulder), 82 (25.5%) received abobotulinumtoxinA in at least one shoulder muscle.
At baseline, patients in the shoulder population had a mean age of 59.2 (standard deviation (SD) 12.0) years and 62.2% were men. In comparison with the non-shoulder population (Table IA), onset of stroke in the shoulder population was slightly more recent (mean 66.2 (SD 72.3) vs 53.8 (SD 59.8) months, respectively); the shoulder population also had a higher composite contracture score (mean 4.3 (SD 3.4) vs 5.4 (SD 3.9), respectively; composite sum of proximal (shoulder, elbow) and distal (wrist, hand) contracture scores) and Total MAS score (10.7 (SD 3.3) vs 11.6 (SD 3.5), respectively; composite sum of MAS score at shoulder, elbow, wrist, finger and thumb joints).
The pectoralis major was one of the most injected muscles in ULIS-II, injected in 76.8% of patients in the shoulder population. Injection sites and doses are shown in Table SIA.
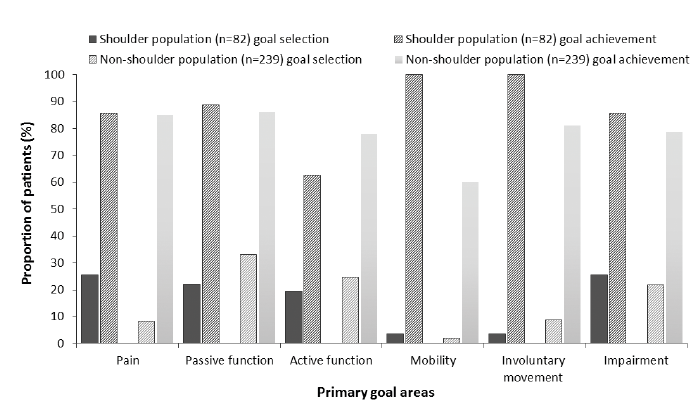
Selection of primary goals at baseline. In comparison with the non-shoulder population (Fig. 1), more patients receiving shoulder injections selected primary goals relating to improvements in pain and impairment (range of movement). The proportion of patients who selected pain as their primary treatment goal was 3-fold higher in the shoulder population compared with the non-shoulder population (25.6% (n = 21/82) vs 8.4% (n = 20/239), respectively), while passive function and involuntary movements were selected by a greater proportion of patients in the non-shoulder population (22.0% (n = 18/82) vs 33.1% (n = 79/239); and 3.7% (n = 3/82) vs 8.8% (n = 21/239), respectively). Other goal selection rates were compar-able between populations.
Fig. 1. Selection and achievement of primary goals in patients receiving shoulder injections compared with the non-shoulder population in the Upper Limb International Spasticity Study-II (ULIS-II) study. “Other” was selected as a primary goal area for 3 patients in the non-shoulder population. n: number.
Achievement of primary goals. In the shoulder population, 82.9% of patients achieved their primary goals. In total, 85.7% to 88.9% of patients achieved their primary goals in pain, passive function (caring for the limb) and impairment (range of movement; Fig. 1), while a lower rate of goal achievement was observed for active function (using the limb; 62.5%).
In the non-shoulder population, 81.6% of patients achieved their primary goals. Overall, 78.0–86.1% of patients achieved their primary goals in pain, passive function, active function, involuntary movement and impairment (Fig. 1), while a lower rate of goal achievement was observed for mobility (balance/gait; 60.0%).
Safety. A single AE was reported in the non-shoulder population (0.4% of patients).
AUL open-label study patients.
In the AUL open-label study, of the 254 patients receiving treatment in the upper limb muscles, 96 (37.8%) received abobotulinumtoxinA injection into a shoulder muscle at one or more treatment cycles. The majority of these patients (n = 84) received at least 2 shoulder muscle injections. At baseline, patient and disease characteristics were comparable between the shoulder and non-shoulder populations (Table IB).
Table I Baseline characteristics for patients who did not receive shoulder injections and patients who did receive shoulder injections in the (A) Upper Limb International Spasticity-II (ULIS-II) study and (B) Adult Upper Limb (AUL) open-label study
In Cycle 1, the most commonly injected shoulder muscle was the pectoralis major (65.7% of patients injected in the shoulder). Injection sites and doses for all cycles are shown in Table SIB.
Assessment of perceived function. As shown in Fig. 2A, pain, hygiene and dressing were each selected as the principal target for treatment on the DAS by a higher proportion of patients in the shoulder population compared with the non-shoulder population. In particular, the proportion of patients selecting pain almost doubled (9.5%) in the shoulder population compared with the non-shoulder population (5.1%). Limb position was selected by a greater proportion of patients in the non-shoulder population.
At week 4 of the last injection cycle to include shoulder muscles, mean (SD) changes from baseline in pain on the DAS were –0.7 (0.9) in the shoulder population compared with –0.4 (0.7) in the non-shoulder population (Fig. 2B). Similarly, the shoulder population showed consistently numerically greater differences from baseline in DAS pain score compared with the non-shoulder population across all treatment cycles, while slightly greater improvements were observed with each cycle for both groups (Fig. 2B).
Fig. 2. Disability Assessment Scale (DAS) in the Adult Upper Limb (AUL) open-label study: (A) primary treatment target selected at baseline, and (B) mean change from baseline to week 4 in the DAS pain domain. *One patient who received shoulder injections had no DAS data. DAS results were not available for some patients at week 4 of each treatment cycle. (B) Patient group numbers are indicated below each column; these numbers indicate all patients who received at least one shoulder muscle injection during any cycle of the AUL open-label study, the numbers of patients injected in the shoulder muscles at each cycle were: n = 35, n = 67, n = 57 and n = 33 at Cycles 1, 2, 3 and 4, respectively. Data presented as the mean; error bars represent standard deviation. “Last cycle” is the last cycle to involve shoulder muscle injections.
Assessment of Tardieu Scale parameters. As shown in Fig. 3, change from baseline to week 4 of the last injection cycle to include shoulder muscles was slightly higher for XV1 in the shoulder population compared with the non-shoulder population (mean (SD), +8.0° (22.2) vs +4.5° (16.1), respectively). Improvements were comparable between shoulder and non-shoulder populations for XV3 (+17.2° (25.2) vs +16.6° (27.6), respectively), and change from baseline for X was slightly greater in the non-shoulder population (–9.2° (27.1) vs –12.1° (27.5), respectively).
Assessment of active function. In patients receiving shoulder injections, a more pronounced improvement was observed in active function compared with the non-shoulder population, with a mean (SD) change from baseline to week 4 of the last cycle to include shoulder muscles in MFS overall score of 0.60 (0.80) and 0.33 (0.79), respectively (Fig. 4). Furthermore, MFS overall score was numerically higher in the shoulder population compared with the non-shoulder population at week 4 of each cycle.
Safety. TEAEs were reported in 55.1% of patients (276 events in 87 patients) in the non-shoulder population compared with 62.5% of the shoulder population (173 events in 60 patients), with falls, muscular weakness, nasopharyngitis, and pain in extremity most commonly reported (6.3% compared with 10.4%; 4.4% compared with 6.3%; 0.6% compared with 5.2%; 3.8% compared with 8.3%, respectively).
Fig. 3. Mean change from baseline to week 4 in passive range of motion (XV1), angle of catch (XV3) and spasticity angle (X) in shoulder muscles at the last injection cycle in the Adult Upper Limb (AUL) open-label study. *One patient who did not receive shoulder injections had no Tardieu Scale results at week 4. Data presented as the mean; error bars represent standard deviation (SD).
Fig. 4. Mean changes in Modified Frenchay Scale (MFS) scores from baseline to week 4 for subpopulations of patients in the Adult Upper Limb (AUL) open-label study. MFS results were not available for some patients at week 4 of each treatment cycle. Patient group numbers are indicated below each column; these numbers indicate all patients who received at least one shoulder muscle injection during any cycle of the AUL open-label study, the numbers of patients injected in the shoulder muscles at each cycle were n = 35, n = 67, n = 57 and n = 33 at Cycles 1, 2, 3 and 4, respectively. Data presented as the mean; error bars represent standard deviation. “Last cycle” is the last cycle to involve shoulder muscle injections.
The present analyses highlight differences in prioritization of rehabilitation goals and treatment responses between patients with ULS who did or did not receive shoulder muscle injections with abobotulinumtoxinA, according to the investigators’ judgement. These descriptive analyses are the first to present data for shoulder spasticity treatment with abobotulinumtoxinA from large-scale, international clinical trials, and present complementary evidence to that of a number of published small-scale randomized controlled trials in this area (11–16, 29).
In ULIS-II, pain was the primary treatment goal in 26% of the shoulder population and only 8% of the non-shoulder population. A similar proportion of patients prioritizing pain as a primary treatment goal (GAS, 26%) was observed by Carvalho et al. (30) in a study of patients with post-stroke ULS receiving BoNT-A treatment in shoulder muscles. However, prioritization of other treatment goals differed from the ULIS-II shoulder population, including involuntary movements/associated reactions (32%), mobility (balance/gait; 18%) and passive function (e.g. hygiene and dressing the affected limb; 9%) (30). Shoulder pain management with BoNT-A treatment alongside concurrent therapy interventions was shown to reduce spasticity, and improve passive function and pain (17). Concomitant therapy during ULIS-II, particularly high intensity therapeutic input, was associated with better goal achievement; although, this was not specific to the shoulder or pain as a primary goal (31). However, evidence from ULIS-III suggests physicians increasingly recognize the need for shoulder injections and benefits of BoNT-A in managing shoulder pain (32). A smaller number of patients received injections in the shoulder in ULIS-II and AUL open-label studies than those that did not receive shoulder injections, reflecting injection practices at the time these studies were undertaken. In ULIS-II, 32.2% of patients were injected around the shoulder, increasing to 39.4% of patients in the ULIS-III study, with most injections targeted at pain reduction, indicating that injection patterns may be changing (32, 33).
In the AUL open-label study, differences in DAS primary treatment target selection were observed between subpopulations. Limb position was selected by the shoulder population less often compared with the non-shoulder population, while the proportion of patients selecting dressing and pain increased notably in patients receiving shoulder injections. These differences between subpopulations in treatment goal prioritization and DAS domains suggest that shoulder spasticity is responsible for some ULS-related pain. These differences also suggest that patients with spasticity affecting proximal upper limb muscles have fewer difficulties with abnormal limb position, while distal muscles may impact the position of the hand, wrist and elbow. Proximal muscles may have a greater impact on disability related to pain, dressing and hygiene.
Overall, high goal achievement rates were observed in ULIS-II for primary goals in the shoulder, particularly relating to pain (85.7%), passive function (88.9%) and impairment (range of movement; 85.7%), with a lower rate of achievement for active function (62.5%). In the AUL open-label study, a notable improvement was observed for DAS pain at week 4 of the last treatment to include shoulder muscles, which was numerically greater in the shoulder population compared with the non-shoulder population (–0.7 vs –0.4, respectively). Improvements in DAS pain (decreased pain) marginally increased across cycles in both subpopulations. These results suggest that abobotulinumtoxinA injections into shoulder muscles may help to achieve patient-centred goals and reduce disability relating to pain.
Although hemiparetic shoulder pain has previously been established and investigated, studies for BoNT treatment have produced varying results (10). Marco et al. (11) (n = 29; targeting the pectoralis major) and Yelnik et al. (12) (n = 20; targeting the subscapularis) reported significant pain relief with abobotulinumtoxinA treatment compared with placebo at 1 month post-injection (p = 0.025). Marco et al. (11) observed significant improvements up to 6 months post-injection. Lim et al. (13) (n = 29, targeting various shoulder muscles) reported pain reduction with onabotulinumtoxinA compared with triamcinolone acetonide. By contrast, studies by de Boer et al. (15) (n = 21; onabotulinumtoxinA, targeting the subscapularis), Wissel et al (29) (n = 18 with shoulder pain as a goal; target muscle not specified) and Kong et al. (14) (n = 16; abobotulinumtoxinA, targeting the pectoralis major and biceps brachii) showed no significant difference in pain relief compared with placebo. Marciniak et al. (16) (n = 21) also reported no difference in magnitude of pain reduction (DAS) between onabotulinumtoxinA and placebo targeting the pectoralis major and teres major; however, patient-reported improvements were observed for DAS hygiene and dressing when treated with onabotulinumtoxinA. This inconsistency in reported benefits of BoNT for shoulder spasticity pain relief may be due to small patient numbers in each trial. Thus, results from the present subanalyses from 2 large-scale studies provides interesting additional data to support the beneficial effect of BoNT in spasticity-related shoulder pain and its impact on patient goal selection, goal attainment, and functional improvements. As previously suggested by Yelnik et al. (12), reduced shoulder pain with BoNT-A injections may improve spasticity in distal muscles.
In the AUL open-label study, a numerically greater improvement in XV1 was observed for patients receiving shoulder muscle injections compared with those without (+8.0° vs +4.5°, respectively). This difference in range of motion, though limited, and perhaps not clinically significant, accords with significant improvements observed by Lim et al. (13) in passive range of motion with onabotulinumtoxinA compared with triamcinolone. Marco et al. (11) also reported significantly improved passive external rotation of the shoulder up to 6 months post-injection (interaction effect, p = 0.041 vs placebo), but not flexion or abduction. Kim et al. (34) showed improved passive range of motion of the affected shoulder (magnitude of +3.8° to +4.9°) with upper limb exercises compared with the control group; these improvements translated into clinically relevant functional improvement in upper extremities, particularly self-care skills such as eating and dressing. Thus, the improved XV1 angles observed here may provide some functional benefit. For XV3 in shoulder muscles, results were similar between shoulder and non-shoulder populations, and slightly greater in the non-shoulder population for X. These Tardieu Scale parameters are recognized as clinically relevant quantitative measures of spasticity (24).
Few previous studies have investigated active function in patients with shoulder spasticity. The present analysis from the AUL open-label study showed improvements in active function (MFS) of almost twice the magnitude in the shoulder vs non-shoulder population (last injection cycle: 0.60 vs 0.33, respectively). In a previous study (n = 16), improvements in passive function, pain and spasticity, were reported following abobotulinumtoxinA injection in patients with spasticity in the shoulder girdle or proximal upper limb muscles (17). Functional improvements may be of considerable importance for patients with shoulder spasticity and pain. In Lindgren et al. (1), patients experiencing shoulder pain after stroke had significantly reduced arm motor function compared with those without shoulder pain (no/reduced function, 83% vs 17%, respectively; p < 0.001). A significantly greater proportion of patients with shoulder pain also experienced moderate or major functional dependence (Barthel Index, 63% vs 25%, respectively; p = 0.001) (1). Targeting shoulder muscles in patients with ULS affecting the shoulder or shoulder pain, may prevent and reduce healthcare utilization. Previously, reduced care burden was reported in patients receiving BoNT-A treatment for ULS (35). Thus, for patients experiencing functional dependence on carers for daily tasks, such as dressing and hygiene, due to shoulder spasticity and associated pain, alleviating these symptoms with BoNT-A may increase independence. Furthermore, these improved MFS scores for patients with shoulder spasticity were observed alongside the improvements described above for XV1, i.e. passive range of motion, which could suggest a beneficial relationship between improved range in the affected shoulder and active function. As noted above, Kim et al. (34) also showed improvements in passive range of motion alongside functional improvement in the upper limb. As discussed elsewhere, and in light of these findings, BoNT-A injections to the shoulder muscles should be considered to reduce pain and improve upper limb movement (36).
The dosing information presented here may be informative for treating physicians. The subscapularis and pectoralis major are the muscles most involved in processes typically observed with shoulder paresis (retraction and depression of the scapula, internal rotation and adduction of the shoulder), while the teres major and latissimus dorsi are involved to a lesser extent (10, 30). Muscle injection patterns observed here were selected according to investigators’ judgement, thus, reflect clinical decision-making of experienced injectors. No new or unexpected safety findings were identified in either the shoulder or non-shoulder groups here, as well as at the doses injected during the AUL open-label study (19), and no investigator-assessed, related AEs leading to withdrawal were reported in the ULIS-II observational study (20).
Although of clinical interest, the present analyses are limited by a lack of formal statistical testing, therefore treatment effects or associations cannot be quantified. These analyses were conducted post hoc and were not powered to explore treatment effects in subpopulations receiving shoulder injections in either trial. Of note, outcome measures in these studies were not selected specifically to assess shoulder function and/or pain. For example, the GAS and DAS measures of pain do not distinguish between pain at rest or during activity, and MFS data were not available for all patients in the AUL open-label study at week 4 of each cycle. In addition, although inter- and intra-rater reliability of the DAS have been established (22), this measure is limited by incomplete evaluation of its validity (37, 38). Further limitations were the absence of a control treatment and that patients were not randomly assigned to treatment arms, due to the observational and open-label designs of the original studies. As this was a post hoc analysis, subgroups were not stratified to account for patients’ baseline characteristics, but as all patients were in the chronic phase of spasticity, this would not be expected to impact the results. Although the design of the present analyses is not as strong as that of the previously published placebo-controlled randomized controlled studies discussed above (11, 12, 14–16, 29), these present analyses were conducted with considerably larger data sets and thus may provide the best current level of evidence for the benefits of abobotulinumtoxinA treatment for patients with ULS requiring shoulder injection.
We present here the first descriptive analyses of patients receiving shoulder injections of abobotulinumtoxinA for ULS treatment in large-scale, international clinical trials. In both studies, pain relief was selected more often as a treatment aspiration in patients requiring shoulder injections compared with those not requiring shoulder injections, suggesting shoulder spasticity may be responsible for ULS-related pain. In ULIS-II, there were high goal achievement rates for all primary goals in the shoulder population, and in the AUL open-label study, greater improvements in pain relief, XV1 and active function were observed for the shoulder population compared with the non-shoulder population. These results indicate that abobotulinumtoxinA injection into shoulder muscles may improve outcomes for adults with ULS involving the shoulder.
The authors thank all patients involved in the study, as well as their caregivers, care team, investigators and research staff in participating institutions. All authors of the current publication were investigators in the ULIS-II and/or AUL studies, and the principal investigators of these 2 studies are informed of and support the development of this publication.
Medical writing support. The authors thank Jacqueline Harte, BSc (Hons) and Germanicus Hansa-Wilkinson, MSc of Watermeadow Medical, an Ashfield Company, for providing medical writing and editorial support, which was funded by Ipsen in accordance with Good Publication Practice guidelines.
Funding. This study was sponsored by Ipsen. The funding agency had no influence on the interpretation of data and the final conclusions drawn.
Data sharing statement. Where patient data can be anonymized, Ipsen will share all individual participant data that underlie the results reported in this article with qualified researchers who provide a valid research question. Study documents, such as the study protocol and clinical study report, are not always available. Proposals should be submitted to DataSharing@Ipsen.com and will be assessed by a scientific review board. Data are available beginning 6 months and ending 5 years after publication; after this time, only raw data may be available.
Conflicts of interest. TL received research grants from Ipsen and consultancy fees from Merz. SK received consultancy fees from Ipsen and Merz. LTS has received consultancy fees from Ipsen. PP and PM are employees of Ipsen. JB was an employee of Ipsen at the time the analyses were run. FCB received consultancy fees from Ipsen, Allergan, Merz and Medtronic.


 Click to show fullsize
Click to show fullsize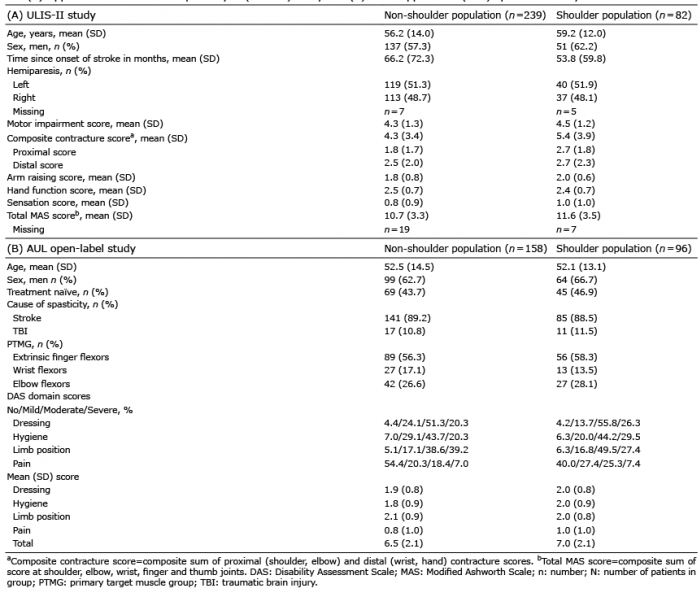 Click to show fullsize
Click to show fullsize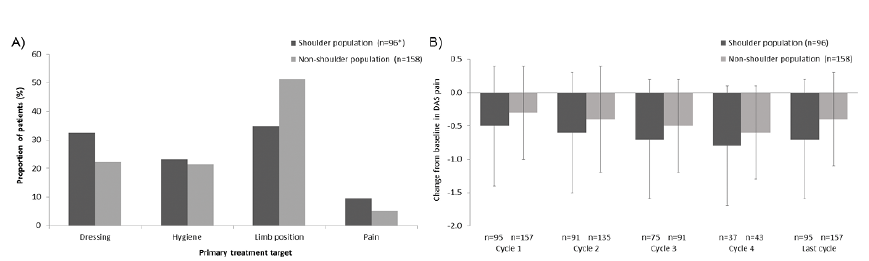 Click to show fullsize
Click to show fullsize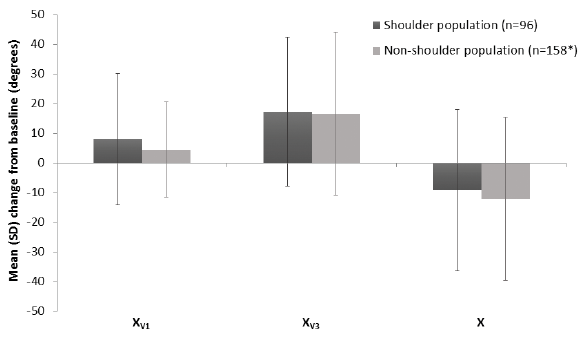 Click to show fullsize
Click to show fullsize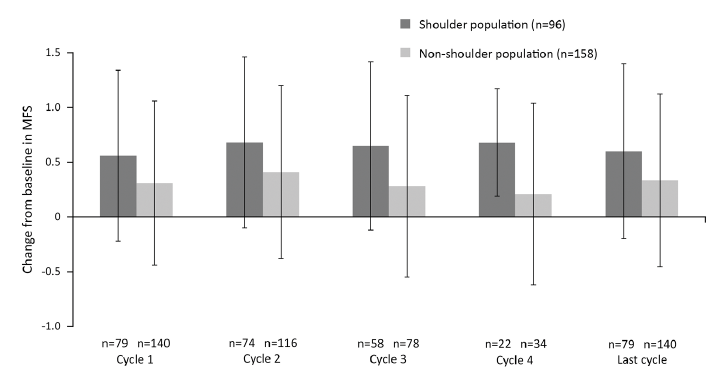 Click to show fullsize
Click to show fullsize