
From the 1Department of Rehabilitation Medicine, 2Institute for Epidemiology, Social Medicine and Health System Research, Hannover Medical School, Hanover, 3Spinal Cord Injury Center, Heidelberg University Hospital, Heidelberg, 4Manfred-Sauer-Foundation, Lobbach, 5Spinal Cord Injury Center, Orthopedic Department, Ulm University, Ulm, 6Treatment Center for Spinal Cord Injury, Trauma Hospital Berlin, Berlin, and 7Clinic for Orthopedics, Clinic Hohe Warte, Bayreuth, Germany
*The GerSCI-Team. This study is a project with several collaborating partners. The cooperating clinics, which are members of the Deutschsprachige Medizinische Gesellschaft für Paraplegiologie (DMGP), provided the field access and sent out the questionnaires. The organization, coordination, data management and descriptive evaluation took place in the Department of Rehabilitation Medicine of Hannover Medical School. The study was carried out in collaboration with the following specialized SCI centers: Paraplegic Center/Department of Paraplegiology and Neuro-Urology Central Hospital Bad Berka, headed by Dr. med. Ines Kurze, SCI Center Median Clinic Bad Tennstedt, headed by Dr. med. Helgrit Marz-Loose, Paraplegic Center of the University and Rehabilitation Clinic Ulm, headed by Dr. med. Yorck-Bernhard Kalke, Medical Rehabilitation Center for Paraplegics of the Heinrich Summer Clinic in Bad Wildbad, headed by Dr. med. Michael Zell, Center for Tetra- and Paraplegia of the Orthopedic Clinic Hessisch Lichtenau, headed by Dr. med. Marion Saur, Center for Paraplegics of the Clinic Hohe Warte Bayreuth, headed by PD Dr. med. Rainer Abel, Department of Paraplegics, Spinal Cord Injury Center at Heidelberg University Hospital, headed by Prof. Dr. med. Nobert Weidner and the Center for Spinal Cord Injuries of the Emergency Hospital Berlin, headed by Dr. med. Andreas Niedeggen. The study was funded by Manfred-Sauer-Foundation.
Objective: The German Spinal Cord Injury Survey is part of the International Spinal Cord Injury Survey, which aims to collect data about the life experience of persons with spinal cord injury worldwide. This paper reports on the perceived environmental barriers of the German study population and their associations with quality of life.
Design: Cross-sectional explorative observational study using survey data.
Participants: A total of 1,479 persons with spinal cord injury aged 18 years and older.
Methods: After descriptive analyses, exploratory factor analysis was used to build groups of environmental barriers. Logistic regressions were performed to assess correlates of perceived environmental barriers. Spearman’s correlations were used to analyse the association between perceived barriers and quality of life.
Results: Barriers regarding infrastructure had a relatively large impact. Barriers in relation to people’s attitudes towards spinal cord injury and the equipment of people with spinal cord injury had a relatively small impact on the lives of people with spinal cord injury. Several subpopulations showed a higher risk in experiencing barriers. Quality of life decreased with increasing experience of barriers.
Conclusion: The most life-hardening barriers were identified related to infrastructure, a category in which most barriers are modifiable, for example, buildings or transportation.
Key words: spinal cord injury; community survey; environmental barriers; quality of life.
Accepted Jun 18, 2020; Epub ahead of print Jul 30, 2020
J Rehabil Med 2020; 52: jrm00090
Correspondence address: Andrea Bökel, Hannover Medical School, Department of Rehabilitation Medicine, Carl-Neuberg-Str. 5, DE-30625 Hanover, Germany. E-mail: boekel.andrea@mh-hannover.de
Environmental barriers influence the lives of people with spinal cord injury. This study measured the perception of environmental barriers like inadequate accessibility, insufficient transportation, lack of technical aids or other services, as well as attitudes of other people towards spinal cord injury. All these may hinder people with spinal cord injury to do whatever they want or to get where ever they want to. The participants perceived a large number of barriers, which made their lives a lot harder. The most life hardening barriers were inaccessibility of public and private buildings, weather conditions and long-distance transportation. Furthermore participants perceived problems with disability insurance, a lack of equality promotion or financial problems which made their lives a lot harder. Since most of these barriers are man-made, target political interventions should be developed to reduce these barriers.
The United Nations Convention on the Rights of Persons with Disabilities characterizes disability as resulting from “the interaction between persons with impairments and attitudinal and environmental barriers that hinders their full and effective participation in society on an equal basis with others” ((1), preamble, e). Research focusing on environmental factors is important for social policies, since many environmental barriers and their impact on participation of people with SCI can be detected and modified (2–8). SCI is a complex and life-changing health condition. Despite increasing medical care and higher survival rates in high-income countries, living with SCI is still an individual and societal challenge (2).
Barriers that hinder the full participation of people with SCI in the context of this study are the inaccessibility of places, limitations due to a lack of technology, transport options or services and restrictions due to the attitudes of people in the immediate vicinity of respondents (e.g. prejudice, overprotective behaviour) (4, 9). Furthermore unfavourable climatic conditions such as disagreeable weather, temperature, season and humidity are referred in terms of participation (4, 9).
Data from a Swiss study in 2013 and an international survey in 2017 showed that the most frequently mentioned barriers were climate, inadequate accessibility, transportation and services (4, 10). Older participants in the Swiss sample more frequently perceived barriers of short-distance transportation and communication devices. Females were more likely to experience negative impacts of climate, attitudes and accessibility of private homes (4). In the international sample people with low income, paraplegia, complete lesion and more health problems perceived more barriers, while the experience of barriers decreased with better mental health and better self-care ability (10). Several authors found, that people with SCI reported barriers due to mobility and equipment issues as well as man-made environmental barriers (11, 12). Xu et al. also found that increased numbers of perceived environmental barriers were strongly associated with decreased quality of life (QoL) (7).
In Germany the working group of social services of the Deutschsprachige Medizinische Gesellschaft für Paraplegiologie (DMGP) collected data about the social situation of people with SCI after discharge from inpatient rehabilitation in 1990 (13). However, they did not use a questionnaire, and therefore, to date, there are no systematic data about perceived barriers of people with SCI in Germany (14). The subject of this study was to analyse for the first time the perceived impact of environmental barriers on the lives of people with SCI in Germany. The specific aims of this study were: (i) to describe the prevalence of perceived environmental barriers in the German study population; (ii) to analyse determinants of experienced environmental barriers across relevant subpopulations based on demographic data and SCI characteristics; and (iii) to identify the influence of environmental barriers on QoL.
Study design
The German Spinal Cord Injury (GerSCI) Survey is part of the International Spinal Cord Injury (InSCI) community survey, which was led and initiated by the International Society of Physical and Rehabilitation Medicine (ISPRM) and the International Spinal Cord Society (ISCoS) as part of the World Health Organization (WHO) Collaboration Plan and coordinated by Swiss Paraplegic Research. The InSCI study protocol is described elsewhere (15). The Learning Health System concept should create the opportunity to improve long-term quality of care. Respective information should help to improve health, function, well-being and, in the end, QoL, for people with SCI (15).
The survey was conducted between March and December 2017. Depending on the preferences of study participants, questionnaires were completed on paper or via web-based data entry.
The study was conducted by the Department of Rehabilitation Medicine at Hannover Medical School (MHH) and was approved by the ethics committee of the MHH, in accordance with the Declaration of Helsinki 1975 (number 7374), as well as the Commissioner for Data Protection at MHH.
Inclusion criteria and participant recruitment
The study sample was derived from the nationwide GerSCI community survey (15).
The GerSCI survey was a cross-sectional, explorative observational study without intervention in people with SCI treated at specialized SCI rehabilitation centres. Out of a total of 27 invited centres within Germany, 8 centres agreed to participate. The hospital databases of those centres were used to compile a sample of patients diagnosed with SCI (traumatic and non-traumatic). Inclusion criteria consisted of inpatient or outpatient contact with the participating SCI centre between 1 January 2000 and 31 December 2016, completion of initial rehabilitation with at least 12 months since the onset of SCI, current residence in Germany, German speech comprehension and a minimum of 18 years of age. Patients with congenital malformations, amyotrophic lateral sclerosis or multiple sclerosis were excluded. A total of 5,598 eligible participants were identified and received a letter with a questionnaire via post. Invited participants who did not respond within 4 weeks were sent a reminder by post. Data were collected using a self-reported questionnaire, which was completed via paper and pencil or a web-based form.
Measurement
To ensure comparability with the international research project, the InSCI questionnaire was translated from English into German. The underlying InSCI data model and the InSCI questionnaire are described elsewhere (16). The GerSCI questionnaire consisted of 86 items on 22 pages and included additional questions regarding the German rehabilitation system. Two instruments out of the GerSCI questionnaire were examined more closely to obtain a full picture of barriers as well as their influence on the QoL.
Nottwil Environmental Factors Inventory Short Form
The Nottwil Environmental Factors Inventory Short Form (NEFI-SF) consisted of 14 items to assess the perceived impact of environmental barriers on the lives of people with SCI. The questionnaire contained questions on the inaccessibility of places, limitations due to a lack of technology, transport options or services and restrictions due to the attitudes of people in the immediate vicinity of respondents (e.g. prejudice, overprotective behaviour) as well as climate (4, 9). The questionnaire was a validated, interviewer-administered questionnaire and was based on the International Classification of Functioning, Disability and Health Core Sets for SCI; it was administered to assess the perceived impact of 14 environmental barriers on social participation during the previous 4 weeks (9, 17). The short form was developed for use in postal or web-based questionnaires and focused on the perceived impact of environmental barriers on participation in general (9). Participants were asked to answer the following question: “In daily life one is exposed to diverse external influences (so-called environmental factors) that can make every day easier or more difficult. Which factor made your participation in society a little, or considerable more, difficult in the last four weeks?” (9). Items were rated as: “not applicable”, “no influence”, “made my life a little harder” or “made my life a lot harder”. It is recommended that “not applicable” could later be re-coded as “no influence”, since something that is not applicable will not be a barrier. Internal consistency of the NEFI-SF was good with α = 0.82 (4, 9, 18, 19).
Measuring quality of life (WHOQoL-BREF)
WHOQoL-BREF is an instrument for recording subjective QoL. The instrument is based on the definition of QoL, as the individual perception of one’s own life situation in the context of respective culture and value systems as well as in relation to personal goals, expectations, assessment criteria and interests. The WHOQoL-BREF questionnaire consisted of 26 items that focused on the dimensions of physical well-being, psychological well-being, social relationships and environment (20). Six items from the WHOQOL-BREF were used in the GerSCI questionnaire. However, regarding environmental barriers, the only item used was: “How would you rate your quality of life in the last 30 days?”, which was rated on a scale with 5 ratings from very poor to very good.
Covariates
In order to analyse for associations, sociodemographic data and lesion characteristics were used, which were age, sex, lesion characteristics (paraplegia vs tetraplegia and complete vs incomplete), aetiology (traumatic vs non-traumatic), time since injury, marital status (single, separated, divorced, widowed vs married, living together), employment status (unemployed vs employed), participation in a lifelong follow-up programme (not participating vs participating) and injury related to a work accident (no vs yes).
Statistical analysis
Sociodemographic data and SCI characteristics are presented as percentages or means with a standard deviation (SD). The key focus of this study was the perception of the impact of environmental barriers on people with SCI in Germany. NEFI-SF frequencies of barriers are presented as sum totals in addition to percentages. Only data from participants with less than 30% missing values were included in the statistical analysis.
The NEFI-SF structure was analysed using exploratory factor analysis with the aim of building groups of perceived barriers and describing prevalence of perceived barriers within these groups (21). A correlation matrix of the Pearson bivariate correlation and Bartlett test, in addition to the Kaiser-Meyer-Olkin measure of sampling adequacy, was conducted. Factors were identified using eigenvalues greater than 1.0 and a scree plot. Since it cannot theoretically be assumed that the combined groups of barriers were completely uncorrelated, a major axis analysis with oblimin rotation was conducted.
To analyse determinants of experienced barriers and identify disadvantaged groups covariates associated with the perception of barriers were assessed using multivariable logistic regression and estimated odds ratios (OR) with a 95% CI. For each group of barriers identified in the exploratory factor analysis, a separate regression analysis was conducted and included the following variables: sex, age, marital status, employment status, lesion height, completeness of lesion, time since injury, participation in lifelong follow-up programme, SCI cause and work accident. The same variables were included in each analysis to directly compare their association with perceived barriers. The 4 rating categories of the NEFI-SF were dichotomized into “0”, which corresponded with “not applicable” and “no influence” and “1”, which corresponded with “made my life a little harder” and “made my life a lot harder”.
In order to identify the influence of environmental barriers on QoL associations of perceived environmental barriers with the WHOQoL item were explored using Spearman’s correlations between the NEFI-SF factor scores and the first item of the WHOQoL-BREF.
Results were considered statistically significant if p-values were less than 0.05. Statistical analyses were performed with SPSS IBM 26.0.
Participants
The response rate was 31.3% (n = 1,754). After exclusion of questionnaires based on unfulfilled inclusion criteria (n = 79), discontinued online questionnaires (n = 56), double questionnaires (n = 2) and those with greater than 30% of values missing (n = 138), 1,479 questionnaires were taken into account for the data analysis. The analysis sample comprised 26.4% of persons who were contacted.
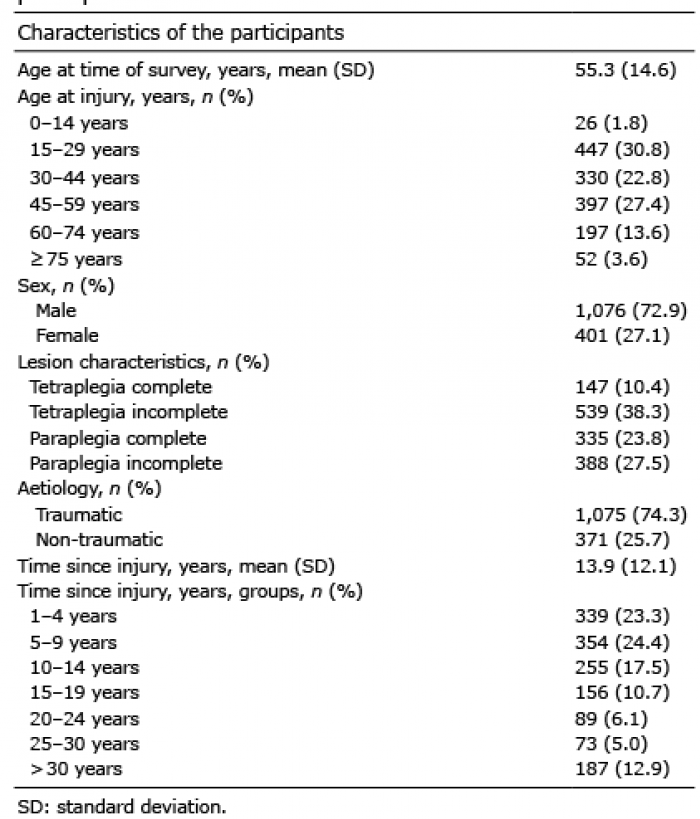
The mean age of the respondents was 55.3 years (SD 14.6) with ages ranging from 19 to 90 years. In addition, most participants were male (72.9%). The largest age group (51–65 years) accounted for 43.5% of the total population of respondents. The mean time since injury was 13.9 years (range 1–62 years, SD 12.0). Men were more likely to have incomplete paralysis (66.3%). Of all study participants, 51.2% had paraplegia and 48.8% had tetraplegia. Most of the participants were married or in a partnership (Table I). Further details are published elsewhere (22). The cohort profile of the InSCI survey can be found elsewhere (23).
Table I. Sociodemographic and lesion characteristics of study participants
Overall, 74.3% of study participants had had traumatic SCI. Of these, 42.2% reported a traffic-related accident and 24.4% reported a sport or recreational activity-related accident (24.4%). In 25.7% of participants, a non-traumatic aetiology was reported and included spinal cord ischaemia (21.8%), neoplasms (21.8%), degenerative spine disease (18.9%), infections (14.0%) and other diseases (20.8%). Work-related accidents were reported by 10.5% of respondents. Further results are published elsewhere (22, 24).
Quality of life (WHOQoL-BREF)
The majority of study participants rated their QoL in the 4 weeks prior to the survey as very good (9.0%) or good (41.0%). Approximately 35.9% of participants reported their QoL as “neither poor nor good”. Few participants described their QoL as poor (10.9%) or very poor (3.3%) (24).
Perceived environmental barriers (NEFI-SF)
A ranking system was created based on the frequencies of perceived environmental barriers. The most frequently experienced environmental barrier was inadequate access to the homes of family members or friends (61.9%). Due to the inadequate accessibility of public buildings or places, the lives of 56.7% of participants became more difficult. The third most often mentioned barrier (62.9% of participants) was climate, which included unfavourable conditions, such as weather, temperature, season and humidity. Missing or inadequately adapted transportation for long-distance travel (such as public transportation or lack of an adapted car) made the lives of 39.3% of participants a little or a lot more difficult. Respondents were affected by inadequate or missing transportation aids (such as stair lifts, walkers or wheelchairs) with regard to short-distance transportation (31.2%). More than one-quarter of study participants indicated a negative impact regarding political decisions, such as issues with insurance or lack of equality promotion, as well as their financial situation (including a shortage of money or a lack of governmental support). More than one-fifth of participants reported issues regarding social attitudes of people towards SCI, such as prejudice or ignorance. A small proportion of study participants perceived inadequate personal care assistance or medical supplies, negative attitudes of family, friends and colleagues and a lack of communication devices, such as writing devices or computers. Table II provides exact numbers and percentages of the perceived barriers.
Table II. Frequencies of experienced environmental barriers for each Nottwil Environmental Factors Inventory Short Form item in total numbers and percentages
NEFI-SF structure analysis, groups of barriers and frequencies in barrier groups
The starting point for exploratory factor analysis is considered ideal if there are separate groups of highly correlated variables. In this study, the correlation matrix of the Pearson bivariate correlation showed that all variables were highly correlated (p < 0.000). The effect sizes ranged from weak to strong. The Bartlett test (χ2 (91) = 7,971.49, p < 0.001) in addition to the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO = 0.879) indicated that the variables were suitable for factor analysis. The exploratory factor analysis indicated the presence of 3 factors with eigenvalues greater than 1.0, which explained 62.02% of the variance. The scree plot also indicated the presence of 3 factors. Since it cannot be assumed that the combined groups of barriers were completely uncorrelated, a major axis analysis with oblimin rotation was carried out. The component transformation matrix confirmed this assumption (Table III).
Table III. Factor values and factor allocation of the exploratory factor analysis
Although 3 factors were identified by exploratory factor analysis, named equipment, attitude and infrastructure, it was decided to separate the item climate from the factor infrastructure, because weather, ambient temperature and humidity are physically and sensorial experienced in contrast to the other items in the infrastructure factor. Furthermore, it is not a man-made factor and cannot be addressed as infrastructural barriers in recommendations to decision-makers.
Fig. 1 displays the median of the sum scores for each group of barriers. The median of infrastructure was higher compared with the others. It showed a mean value of 0.91 (SD 1.25) out of 5 barriers for equipment, while attitude had a mean of 0.55 (SD 1.04) out of 4 barriers. The mean for infrastructure is clearly above this level with a mean of 1.93 (SD 1.46) out of 4 barriers. The mean of climate was 0.46 (SD 0.50) out of 1 (Fig. 1).
Fig. 1. Means of perceived barriers in the 4 groups of barriers.
Odds ratios for factors associated with the perception of barriers
The results of multivariable logistic regression showed that male sex, not living alone, unemployment, non-traumatic SCI, and no work accident were associated with the experience of equipment barriers. The perception of infrastructure barriers was associated with unemployment and a complete lesion. Experiencing the climate barrier was associated with tetraplegia and participation in the lifelong care programme. The model for attitude barriers was not significant (Table IV).
Table IV. Logistic regression for factors associated with the perception of environmental barriers (n = 974); p<0.05 are in bold
Associations of perceived environmental barriers and quality of life
Table V illustrates the association of NEFI-SF factor sum scores with the first WHOQoL-BREF item. All associations were negative (p<0.01), indicating decreased QoL with increased perception of all barriers. However r = –0.275 as the highest value corresponds to a small effect according to Cohen (25).
Table V. Spearman’s correlation coefficients and probabilities of perceived environmental barriers (sum scores) with quality of life
In this study on the perceived impact of environmental barriers using NEFI-SF for people with SCI in Germany, infrastructural barriers especially had a negative impact on lives of the participants. People who were unemployed and those with a complete lesion were more likely to experience infrastructural barriers. The perception of barriers was significantly associated with QoL.
Accessibility of homes of relatives and friends, climate and public access, in addition to long-distance transportation were identified as barriers with the most life-hardening impact on people with SCI. The 3 most common barriers with the most negative impact were nearly identical to the results of a study of the Swiss population in 2013 (9). In the German population, the accessibility of homes of relatives and friends was the most often chosen option regarding “made my life a lot harder”; however, in the Swiss population this option was chosen third most often. The impact of climate was chosen the second most often in the German population, but was chosen as first in the Swiss population. The German population chose public access third, whereas the Swiss population chose this as second (4). The values of both countries were similar regarding the financial situation, with one-third of both populations describing their financial situation as problematic. Consequently, the values of the 2 countries do not deviate substantially from each other.
We hypothesize a large number of people affected by inadequate or missing transportation aids (such as stair lifts, walkers or wheelchairs) over shorter distances might indicate a mismatch between individual expectations and requirements of the respondents and the medical and technical aids that are provided. Moreover, these aids are essential for people with SCI to maintain independent mobility.
Factor analysis showed a large number of barriers in infrastructure compared with attitudes, equipment or climate. Participants experienced 1.93 out of 4 barriers. These results indicated that inaccessibility and inadequate public transport are the most life-hardening barriers. Since they are man-made barriers, it is necessary to check what kind of barriers these are and how they could be adapted to prevent further exclusion of people with SCI.
Non-traumatic SCI were significantly associated with the experience of equipment barriers. Reinhardt et al. also found that people with non-traumatic SCI were more often affected by insufficient financial resources, which is also an equipment barrier (4). We hypothesize that the association between aetiology of non-traumatic SCI and the experience of an equipment barrier could be explained by the German Statutory accident insurance, which supports people after a traumatic, but not after a non-traumatic occurrence of SCI.
Another disadvantaged group regarding equipment barriers are people who had no work-related accident. In Germany treatment after work related accidents is founded by German Workmen’s compensation, which here seems to be an advance regarding equipment (Table V).
In particular, people with a complete lesion perceived infrastructure barriers 4.3 times more often than people with an incomplete lesion. Also, respondents with complete lesions from the study of Reinhardt et al. reported more negative impact of inaccessible public and private buildings and transportation (4). This suggests a considerable restriction on participation in public life for this group. This could be the case, because people with incomplete lesions might be able to use stairs by walking on crutches. This is not possible for people with complete lesion who rely on a wheelchair. These barriers could be reduced by a consequent realization of adequate accessibility in all areas of public and private places, buildings and transportation.
But why do employed participants who live with partners or family experience significantly more equipment barriers? This could be explained by what Whiteneck & Dijkers (26) called the ‘paradox of measurements of environments’. Especially relating to participation it may be the people who live a more active and social life who report the most perceived barriers, because they have an occasion to perceive these barriers (26). In our sample those respondents who were employed or lived with partners or family reported significantly more equipment barriers, than people who were unemployed or lived alone. It could be hypothesized that the social integration in the partnership or family, as well as at work, offered opportunities to experience barriers and lack of resources.
The associations with the factor climate showed disadvantages for people with tetraplegia. It has been hypothesized that this could be related to insufficient thermoregulation of people with tetraplegia (27). Another surprising result was that those who participated in the lifelong follow-up programme had a significantly higher risk for experiencing climate as having a negative impact on participation. We hypothesize that they might be somewhat stronger focused on body awareness or could be more active, due to the programme.
Since the significant negative association between the experience of each group of barriers with a negative impact on participation and QoL was not surprising and was also found by Xu et al., a more detailed evaluation of QoL should be conducted in a further study (7).
Study strengths
This is the first study to provide data about barriers experienced by people with SCI in Germany. It identified problems of lives of people with SCI regarding their participation. Now medical societies, as well as patient societies, are able to perform recommendations, based on these as well as the GerSCI study results, to political decision-makers, healthcare providers and clinicians in order to improve life and supply situations of people with SCI in Germany. A policy brief, written on the basis of this study, has already been presented to the Federal Ministry of Health, while a regular political dialogue and sharing information was consented. This could aid in the future development of a learning health system for people with SCI.
An additional strength was the sample size of GerSCI, which was the largest sample size of all countries in the InSCI survey.
The key concepts, such as WHOQoL-BREF and NEFI-SF, used for the analysis were assessed using questionnaires validated for people with SCI.
Study limitations
The recruiting strategy included possible selection bias because it exclusively involved people treated in specialized SCI centres and excluded all persons who were treated in centres and hospitals without a specialization in SCI. Another limitation of the study was that only 8 out of 27 centres participated. This large number of centres that did not participate led to regional “blind spots”, i.e. people in the west and north of Germany were not included in the analysis. Furthermore, the response rate (32.6%) was lower compared with the SwiSCI study conducted in 2013. This lower response rate could be due to the very extensive questionnaire utilized for this study.
Since answering the questionnaire itself is a motor activity, this also creates a selection bias. Although the questionnaire was available in paper form in addition to an online version, people with impairments of the upper extremity did not have the chance to participate if they were lacking technical aids or further assistance. The perceived barriers of a lack in communication devices are low in this data collection; however, this may be due to those with a lack of communication devices not having the ability to answer the questionnaire.
Even though the GerSCI sample was the largest in the InSCI survey with 1,479 participants in this analysis, it is small in the context of the prevalence of traumatic SCI in Germany (50/100,000) and the incidence of approximately 1,000 cases/year (28). Taking all of these limitations into account, the representativeness of the study is therefore limited.
Conclusion
Contextual factors, such as infrastructure, showed a high negative impact on the lives of people with SCI, even though Germany is a high-income country. Regarding the fact that infrastructural barriers, such as public transport and accessibility of buildings, are usually man-made and therefore modifiable, these should be changed in favour of people with SCI as well as those with other mobility restrictions. The future outlook of GerSCI should focus on policy briefs and dialogues with stakeholders, in order to recommend further actions according to the learning health system.
This study is part of the International Spinal Cord Injury (InSCI) Community Survey. InSCI provides the epidemiological evidence for the Learning Health System for Spinal Cord Injury (LHS-SCI, see also Am J Phys Med Rehabil 2017; 96 (Suppl): S23–S34). InSCI and the LHS-SCI are efforts to implement the recommendations of International Perspectives on Spinal Cord Injury (IPSCI, Bickenbach JE, Officer A, Shakespeare T, von Groote P. Geneva: WHO Press; 2013).
The members of the InSCI Steering Committee are: Julia Patrick Engkasan (ISPRM representative), James Middleton (ISCoS representative, Australia), Gerold Stucki (Chair Scientific Committee), Mirjam Brach (Representative Coordinating Institute), Christine Thyrian (Representative Study Center), Marcel W.M. Post (Scientific Advisor, The Netherlands), Jerome Bickenbach (Scientific Advisor), Linamara Battistella (Brazil), Jianan Li (China), Brigitte Perrouin-Verbe (France), Christoph Gutenbrunner (Germany), Christina-Anastasia Rapidi (Greece), Luh Karunia Wahyuni (Indonesia), Mauro Zampolini (Italy), Eiichi Saitoh (Japan), Bum Suk Lee (Korea), Alvydas Juocevicius (Lithuania), Nazirah Hasnan (Malaysia), Juan Manuel Guzmán González (Mexico), Abderrazak Hajjioui (Morocco), Johan K. Stanghelle (Norway), Piotr Tederko (Poland), Jorge Laíns (Portugal), Daiana Popa (Romania), Conran Joseph (South Africa), Mercè Avellanet (Spain), Michael Baumberger (Switzerland), Apichana Kovindha (Thailand), and Reuben Escorpizo (USA)
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize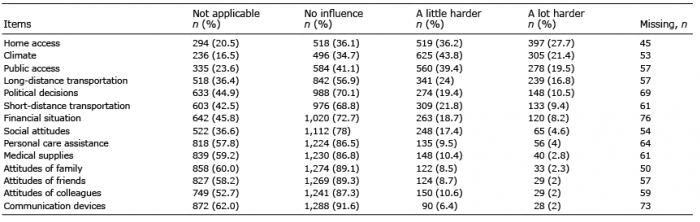 Click to show fullsize
Click to show fullsize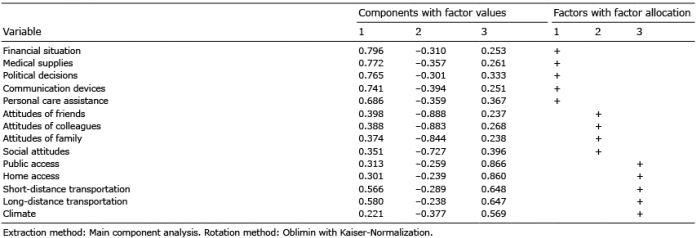 Click to show fullsize
Click to show fullsize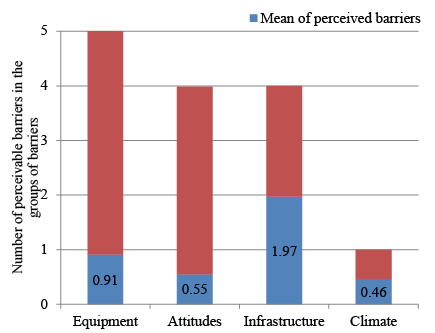 Click to show fullsize
Click to show fullsize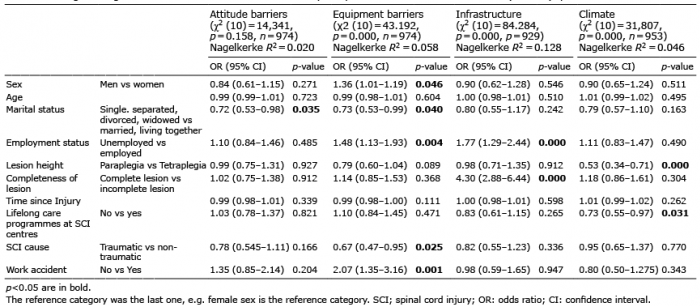 Click to show fullsize
Click to show fullsize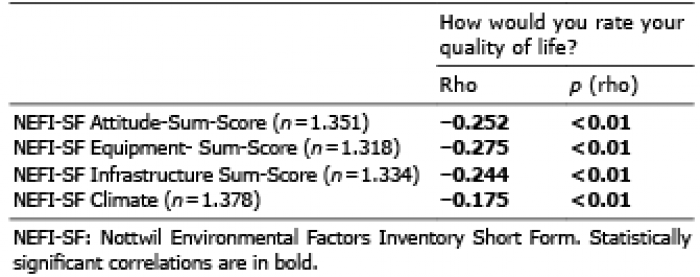 Click to show fullsize
Click to show fullsize