
From the 1Department of Physical Education, National Kaohsing Normal University, Kaohsiung City, Taiwan, 2Institute of Physical Education, Health, and Leisure Studies, Tainan City, Taiwan, 3Department of Kinesiology, National Tsing Hua Universtiy, Hsinchu City, Taiwan
Objective: To determine the joint position sense of the lower extremities and its relationship with motor function in children with developmental coordination disorder and typically developing children.
Methods: A total of 56 participants were recruited; 28 children with developmental coordination disorder (mean age 10.86 years (standard deviation (SD) 1.07) ; 13 females, 15 males) and 28 typically developing children (mean age 10.96 years (SD 1.18); 12 females, 16 males). Knee and ankle joint position sense were assessed using a Biodex isokinetic dynamometer. Joint position acuity was measured by position error (PE) and position error variability (PEV). Motor function was examined using the 2nd edition of Movement Assessment Battery for children (MABC-2) and quantified via sub-scores from 3 MABC-2 domains.
Results: Both PE and PEV at knee and ankle joints were significantly greater in children with developmental coordination disorder compared with typically developing children. In addition, both PE and PEV were significantly greater at the ankle joints than the knee joints in children with developmental coordination disorder. For children with developmental coordination disorder only, joint position acuity in the lower extremities significantly and negatively correlated with MABC-2 balance sub-score.
Conclusion: This study verifies that lower limb proprioception is impaired in children with developmental coordination disorder. Also, children with developmental coordination disorder displayed greater proprioceptive deficits at the ankle compared with the knee joint. Children with developmental coordination disorder who had poorer joint position acuity, i.e. greater PE and PEV, in the lower extremities tended to perform less well in balance function.
Key words: joint position sense; balance function; knee; ankle; developmental coordination disorder.
Accepted Jun 5, 2020; Epub ahead of print Aug 6, 2020
J Rehabil Med 2020; 52: jrm000088
Correspondence address: Fu-Chen Chen, 116 Heping 1st Road, Lingya District, Kaohsiung City 802, Taiwan. Email: fcchen@mail.nknu.edu.tw
This is the first study to investigate joint position sense (the awareness of the postion of a joint in space) of the lower limbs and its relationship with motor func-tion in children with developmental coordination disorder and typically developing children, while addressing limitations in previous studies. The results show that children with developmental coordination disorder have: (i) impaired joint position sense at both knee and ankle joints; (ii) poorer joint position sense at ankle than knee joints; and (iii) decreased balance function with increasing impairment in joint position sense in their lower extremities. These findings suggest that lower limb proprioception is impaired as well as joint position acuity of lower extremities plays a role in balance function in children with developmental coordination disorder.
Developmental coordination disorder (DCD) is a common neurodevelopmental motor condition with a prevalence of 5–6% in children ages 5–11 years worldwide (1). The motor coordination deficits of DCD crucially interfere with activities of daily living (e.g. buttoning, tying shoelaces, using utensils), as well as poor participation and performance in school (e.g. painting, handwriting, sports) (1). Children with DCD show coordination difficulties across a variety of motor domains, such as manual dexterity, aiming and catching, and balance (2). To date, the aetiology and pathogenesis of DCD are unknown. Proprioceptive information does not only affect the detection and correction of movement errors, regulation of coordinated movement, motor learning, and balance control, but also impacts individual function and independence in daily life (3, 4). Therefore, the current study was particularly concerned with testing proprioceptive sense and exploring its relationship with motor function in children with DCD.
Recently, studies have begun to adopt a joint position matching paradigm to evaluate proprioceptive characteristics in children with DCD. One study using an “active” matching test reported that the joint position sense of both elbows and wrists is impaired in children with DCD compared with typically developing (TD) children (5). Also, the study unexpectedly demonstrated that elbow/wrist joint position sense was not correlated with motor function in either the DCD or the TD groups. Similarly, another study employing an identical test protocol found significantly poorer proprioceptive acuity of the wrist joints in children with DCD compared with TD children, and no correlation between wrist joint position sense and motor function between the DCD and TD groups (6).
In these studies, upper extremity joints were moved passively from the neutral joint position to a target position by an experimenter, at an approximate velocity of 20−25°/s, and held there for 3 s before returning to the neutral position. Children were then required to actively reproduce the target position with no visual or auditory feedback. However, several factors should be considered in this “active” joint position matching test. Firstly, limb velocity was passively and manually controlled by an experimenter and actively moved by the children themselves. Joint angular velocity can impact proprioceptive sense, with higher joint velocities showing decreased detection threshold (increased sensitivity) to proprioception, and vice versa (7, 8), varied limb movement velocity can confound the perception of joint position sense. Secondly, an “active” matching test using volitional control of limb movement showed that, during active movement, an efferent copy of the motor command is yielded and transmitted to the central nervous system (CNS) to anticipate the consequences of the movement itself (9). In this case, the active joint position matching test is not a “pure” test of proprioceptive sense, and matching test performance is influenced by the integration of both internal prediction information and external sensory signals (10). Furthermore, a core feature of DCD is poor motor control, as shown in altered movements and postures leading to abnormal motor function (e.g. 11, 12). This means that the active joint position matching test may be suboptimal for estimating proprioception. Lastly, to the best of our knowledge, no research has yet investigated proprioception in the lower extremities using a joint position matching paradigm in children with DCD. Furthermore, little is known about the specific association between joint proprioceptive acuity in the lower extremities and motor function in children with and without DCD.
Hence, the objectives of this study were to determine the joint position sense of lower extremity joints, as well as correlations between lower extremity joint proprioceptive acuity and motor function performance in children with DCD and TD children. The study controlled for suspected confounding factors, such as inconsistent joint angular velocity and active control of limb movement.
Written informed consent was obtained from all participants and their parents, and ethics approval was provided by the Institutional Review Board at Antai-Tian-Sheng Memorial Hospital in Pingtung County, Taiwan (IRB No. 19-020-A). The study methods complied with the principles of the Declaration of Helsinki for human subject research.
Participants
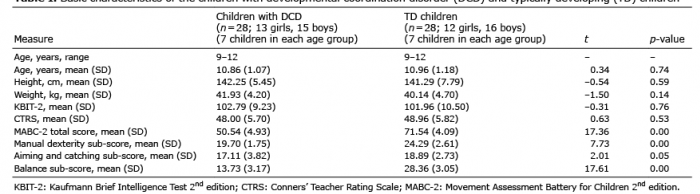
A total of 56 participants, age range 9–12 years, were recruited from local schools; 28 children with DCD (7 in each age group; mean age 10.86 years (standard deviation (SD) 1.07); 13 females, 15 males) and 28 TD children (7 children in each age group; mean age 10.96 years (SD 1.18); 12 females, 16 males). Motor function was assessed with the 2nd edition of Movement Assessment Battery for Children (MABC-2), which has 4 age bands, each with 8 test items nested in 3 motor domains (manual dexterity, aiming and catching, and balance) (13). In accordance with the MABC-2 manual, the raw score of each item was converted to a standard score based on normative data, and the MABC-2 total score was the sum of the standard sub-scores of the 3 domains. For children with DCD, motor coordination and balance function were significantly below that expected for their age, as confirmed by a < 5th percentile total score and a < 5th percentile balance sub-score from MABC-2. In addition, in children with DCD motor coordination difficulties substantially interfered with activities of daily living and school activities, as confirmed by a > 95th percentile score on the checklist of MABC-2. TD children had a > 15th percentile total score and a > 15th percentile balance sub-score on the MABC-2 test, as well as a < 85th percentile score for the MABC-2 checklist. Both the DCD and TD groups were not comorbid for ADHD (Attention-deficit/hyperactivity disorder), as confirmed by a < 70 score on Conners’ Teacher Rating Scale (CTRS) (14). All participants showed normal intelligence, as confirmed by a > 80 score on the 2nd edition of the Kaufmann Brief Intelligence Test (KBIT-2) (15). A history of severe lower extremity injuries, e.g. muscle tear, ligament rupture, or fracture, or neurological disorders, e.g. epilepsy, cerebral palsy, and Tourette’s syndrome, which may affect children’s motor function and development, were excluded based on parents’ reports. All participants were right-foot dominant, as determined by the preferred leg used to kick a ball (16). Table I shows the basic data for the children with DCD and TD children.
Table I. Basic characteristics of the children with developmental coordination disorder (DCD) and typically developing (TD) children
Procedures
The study was conducted at the Sport Biomechanical Laboratory, National Kaohsiung Normal University, Kaohsiung City, Taiwan. The laboratory was kept quiet and free from distraction throughout the experimental procedure. Details of the experimental procedures were explained to participants by a researcher before commencing the study. Participants were seated on a Biodex isokinetic dynamometer (Biodex System 3, Biodex Medical Systems Inc., Shirley, NY, USA), leaning their back against a rigid backrest (Fig. 1). Subjects were stabilized with foam rubber straps across the trunk and hip joints. Participants were asked to wear sport shorts with no shoes during the execution of the “passive” ipsilateral joint position matching test. To prevent mental fatigue resulting from the prolonged test time, only the dominant leg was assessed. Children were blindfolded to eliminate external visual cues. They also listened to pink noise through headphones, to mask external auditory cues.
To measure knee joint position sense, the Biodex dynamometer was adjusted so that participants were seated in the chair (backrest inclined at 85° from horizontal), with the hip flexed at 90° and the popliteal fossa situated approximately 5 cm from the edge of the seat. The participant’s thigh was strapped, and the lower leg was secured to the lever arm immediately above the lateral malleolus. The rotational axis of the dynamometer lever arm was aligned with the knee joint axis of flexion and extension (lateral femoral epicondyle) with a knee flexion at 90° (Fig. 1A). To measure ankle joint position sense, participants were seated in the chair (backrest inclined at 70° from horizontal), with the hip flexed at 90° and knee flexed at 20°, while the foot was fixed to the footplate using Velcro and elastic straps. The rotational axis of the dynamometer lever arm was positioned to be coaxial with the ankle joint axis of plantarflexion and dorsiflexion (fibular malleolus), with ankle dorsiflexion at 0° (Fig. 1B).
To discourage participants from using timing cues, the starting position and target angle were not constant among test trials, based on previous work (17–20). To begin, the participants’ limb was passively moved from a starting position (knee flexed 80°, 90°, or 100° for the knee matching test; ankle dorsiflexed at 0°, 5°, or plantar flexed at 5° for the ankle matching test) to a target angle (30° or 60° flexion of knee joint and 10° or 15° dorsiflexion of ankle joint in an open kinetic chain by the isokinetic dynamometer). The joint angular velocity was set to a constant 1°/s. The presentation order of the combined starting position and target angle varied across participants following a Latin square design. The limb was then maintained at the target angle for 5 s to allow children to memorize the position. Afterwards, the limb was returned to the starting position. The dynamometer then again passively moved the leg from the starting position toward the target angle and participants were instructed to replicate the target angle as closely as possible. Participants had to indicate when the “perceived” target angle had been reached, by pressing a button to stop the motion of the dynamometer. Participants could attempt to fine-tune the perceived angle until they were satisfied with their adjustments and matches. Subsequently, participants’ lower limb was passively returned to the starting position for the next trial. No verbal feedback was provided by the experimenter.
There were 20 trials in total, 10 for the knee joint position matching test (5 for each target angle) and 10 for the ankle joint position matching test (5 for each target angle). Trials were blocked and counter-balanced, such that half the children with DCD and TD children first performed the knee joint matching test, followed by the ankle joint matching test. The other half of the subjects performed the tests in the reverse order. There was a 10-s inter-trial interval and a 10-min resting interval between blocks. Prior to formal measurements, 2 practice trials confirmed that all participants were familiar with the testing procedures. If any participants seemed unsure, additional instruction, demonstration, and practice were provided. Participants took approximately 30–40 min to complete the entire experimental procedure. Fig. 2 shows the experimental procedures.
Fig. 1. Experimental setup for joint position matching for: (A) knee joint and (B) ankle joint. Permission has been given to publish the photo from the patients
Fig. 2. Experimental procedures. DCD: developmental coordination disorder; TD typically developing children.
Statistical analysis
All measurements were summarized as means with standard deviation (SD). Dependent variables were basic data and proprioceptive acuity data, including position error (PE) and position error variability (PEV). The PE was calculated by taking the absolute value of the difference between the perceived angle and target angle in degrees (formula 1). The PEV was calculated as SD of the PE across trials (formula 2). Normality and homogeneity of variance were checked using Kolmogorov–Smirnov and Levene’s tests. Basic data were compared using an independent t-test. Proprioceptive acuity data (PE and PEV) were analysed using a Group (2 levels: children with DCD and TD children) × Joint (2 levels: knee and ankle) mixed analysis of variance (ANOVA) model. Significant interactions were further investigated using the Bonferroni post-hoc analysis to demonstrate the simple main effects of either Group or Joint. Partial eta-squared (ηp2) was calculated for ANOVA effects to indicate effect size. Pearson product-moment correlations were conducted between proprioceptive acuity data (PE and PEV) and sub-score in 3 motor domains of the MABC-2 (manual dexterity, aiming and catching, and balance) for children with DCD and TD children, separately. Significance was accepted for p-values < 0.05. Statistical analysis was performed with SPSS version 18.0 software package (SPSS Inc., Chicago, IL, USA).
PE=|P–T|
Formula 1. Calculation of PE measures, where P=degree of the perceived joint angle; T=degree of the target joint angle.
Formula 2. Calculation of PEV measures, where N=total number of trials; Pi=degree of the perceived joint angle on trial i; P, =mean degree of the perceived joint angle.
Basic data
No significant differences were found between groups for age, height, weight, or scores on CTRS and KBIT-2 (p > 0.05). However, the DCD group were significantly lower than the TDC group for the manual dexterity sub-score (t (54) = 10.82, p < 0.05), aiming and catching sub-score (t (54) = 15.13, p < 0.05), balance sub-score (t (54 = 12.29, p < 0.05), and total score for MABC-2 (t (54) = 21.68, p < 0.05).
Proprioceptive acuity data
Fig. 3 demonstrates the data regarding PE for the 2 groups of participants at both knee and ankle joints. In terms of PE, the ANOVA identified an interaction effect between Group and Joint (F (1, 54) = 18.23, p < 0.05, ηp2 = 0.25). Bonferroni post-hoc analysis revealed a significant simple main effect of Group for the knee joint (F (1, 54) = –2.85, p = 0.01) and ankle joint (F (1, 54) = –10.37, p < 0.01), indicating that DCD children showed larger position error compared with TD children for both knee (DCD = 6.21±3.45°, TD = 4.27±1.06°) and ankle joints (DCD = 8.77±2.19°, TD = 3.73±1.36°). Furthermore, Bonferroni post-hoc analysis revealed a significant simple main effect of joint in the DCD group (F (1, 54) = –4.01, p < 0.01), but not in the TD group (F (1, 54) = 1.57, p = 0.13), indicating a larger position error in the ankle than in the knee joint for the DCD group only (knee = 6.21±3.45°, ankle = 8.77±2.19°). Detailed PE data are provided in Appendix I.
Fig. 3. Position error of knee and ankle joints in children with developmental coordination disorder (DCD) and typically developing (TD) children. Asterisks denote significant differences in position error between the DCD and TD groups. Daggers denote significant differences in position error between knee and ankle joints within the DCD group. Error bars show standard deviation.
Fig. 4 shows data regarding PEV for 2 groups of participants for both knee and ankle joints. For the PEV, ANOVA identified an interaction effect between Group and Joint (F (1, 54) = 16.72, p < 0.05, ηp2 = 0.24). Bonferroni post-hoc analysis revealed a significant simple main effect of Group at the knee joint (F (1, 54) = –2.73, p = 0.10) and at the ankle joint (F (1, 54) = –9.90, p < 0.01), indicating that DCD children showed larger position error variability compared with TD children for both knee (DCD = 2.92±1.66°, TD = 2.02±0.50°) and ankle joints (DCD = 4.31±1.01°, TD = 1.91±0.78°). In addition, Bonferroni post-hoc analysis revealed a significant simple main effect of joint in the DCD group (F (1, 54) = –4.53, p < 0.01), but not in the TD group (F (1, 54) = 0.61, p = 0.55), indicating larger position error variability in the ankle than in the knee joint for the DCD group only (knee = 2.92±1.66°, ankle = 4.31±1.01°). Detailed PEV data are shown in Appendix II.
Fig. 4. Position error variability of knee and ankle joints in children with developmental coordination disorder (DCD) and typically developing (TD) children. *Significant differences in position error variability between the DCD and TD groups. †Significant differences in position error variability between knee and ankle joints within the DCD group. Error bars show standard deviation.
Fig. 5 demonstrates correlations between proprioceptive acuity data (PE and PEV) and MABC-2 balance sub-score for both the ankle and knee joints in DCD children. Within the DCD group, there were significantly negative correlations between PE and MABC-2 balance sub-scores for the knee joint (r = –0.47, p = 0.01, Fig. 5A) and ankle joint (r = –0.41, p = 0.03, Fig. 5B), as well as significant negative correlations between PEV and MABC-2 balance sub-scores for the knee joint (r = –0.44, p = 0.02, Fig. 5C) and ankle joint (r = –0.42, p = 0.03, Fig. 5D). However, the proprioceptive acuity data did not significantly correlate with either manual dexterity sub-score (p > 0.05) or aiming and catching sub-score (p > 0.05) in children with DCD. Furthermore, within the TD group, no significant correlations were detected (p > 0.05). Detailed correlation data are shown in Appendix III.
This study investigated the characteristics of joint position sense in the lower extremities for children with and without DCD. The major findings were that children with DCD have: (i) inferior proprioceptive acuity, measured in terms of position error and position error variability, in the knee and ankle joints; (ii) poorer proprioceptive acuity in the ankle joint compared with the knee joint; and (iii) negative correlations between the impaired joint position sense in their lower extremities and balance function. The results are discussed below.
Joint position sense acuity is reduced in both knee and ankle joints in developmental coordination disorder
Firstly, the present study demonstrated, for the first time, significantly reduced knee and ankle proprioceptive acuity in children with DCD relative to TD children. Overall, the current study extended the findings of previous studies by demonstrating that proprioceptive deficits in children with DCD is not only localized to upper extremity joints, e.g. elbow and wrist, but also influences lower extremity joints, e.g. knee and ankle. Previous studies observed that the PEV (not PE) of the DCD group was larger compared with the cohort group (5, 6). In line with previous studies, the present study showed that PEV was larger in children with DCD than in TD children, demonstrating a variable perceptual judgment about lower extremity joint position in children with DCD. However, contrary to previous studies, the present study showed that PE was larger in children with DCD compared with TD children, indicating that children with DCD have a reduced ability to identify joint position through proprioception. These variable-dependent differences in proprioceptive performance can be reasonably explained by the different approaches used to determine joint position sense among studies. Previous studies (5, 6) employed an active joint position matching test, which requires voluntary control over skeletal muscle and did not strictly control active and passive limb movement velocity. In contrast, the present study purposely minimized confounding effects from participants’ active movement control and altered movement velocity by implementing a passive joint position matching test and applying a constant-velocity mode from the Biodex dynamometer. Based on current and previous studies, for children with DCD, an active joint position matching test with varied movement velocity may not be sensitive enough to detect any proprioceptive deficits, but a passive joint position matching test with constant joint angular velocity is sufficiently sensitive to identify proprioceptive deficits for children with DCD. One may argue that active movements are closely related to activities of daily living, but passive movements are less functionally connected. The question then arises: why does performance on the passive joint position sense test matter? In fact, studies have indicated that a proprioceptive test demanding volitional control of bodily movement may not appropriately reflect the sense of joint position (21). Moreover, anaesthetic block of the joint does not affect active proprioceptive acuity, but merely reduces performance in the passive joint position test, demonstrating that passive joint matching test is more appropriate to examine the function of proprioceptive receptors in the joint (22). Asthon-Miller et al. (23) and Deshpande et al. (24) also suggested using a test not associated with motor control for measuring changes in proprioceptive acuity. Here, the present study uses a passive matching test to better control for confounding variables when assessing joint position sense, i.e. inconsistent joint angular velocity and active control of limb movement, thus more clearly demonstrating the characteristics of lower extremity proprioceptive deficits in children with DCD.
At present, the mechanism underpinning proprioceptive abnormalities in children with DCD remains poorly understood. Afferent signals coming from both muscle spindles and skin receptors play crucial roles in the sensation of limb movement and position (25). Notably, there is a lack of empirical research concerning the fusimotor sensitivity of muscle spindles in children with DCD. However, a number of studies have shown that children with DCD tend to have hypotonia (26, 27). With low muscle tone, the length of skeletal muscle fibre is longer than normal when the muscle is at rest and/or during a sustained voluntary contraction. Here, the internal force generated by muscle contraction and position or movement of body limbs may not be sufficient to trigger muscle spindle activation. It could, therefore, result in a low firing rate of proprioceptive afferents, which can further lead to joint position sense deficits in children with DCD. Also, joint rotation can result in strains of adjacent skin, i.e. stretched on one side of the joint and slackened on the other side, and stimulate tactile mechanoreceptors in the skin, thus potentially contributing to limb position sensation. Studies have indicated that children with DCD show an elevated threshold for tactile-related sense, e.g. light touch (28) and haptic discrimination (29). A higher tactile-related threshold could, at least in part, account for reduced proprioceptive performance at the knee and ankle joints for children with DCD. Furthermore, similar generalized proprioceptive impairments influencing both knee (30) and ankle joints (31) are seen in patients with Parkinson’s disease, which affects the cortico-basal ganglia-thalamo-cortical circuitry. Although there is no direct evidence for anatomical and physiological changes in the sensory area of the brain responsible for proprioception, recent imaging studies reveal that functional connectivity between the motor cortex and primary/secondary somatosensory cortex (postcentral gyrus, parietal operculum, and supramarginal gyri), as well as between the motor cortex and basal ganglia regions (caudate, putamen, and globus pallidus) are altered in children with DCD (32, 33). Future research should systematically investigate the possible causes of impaired proprioception in children with DCD in the peripheral nervous system, e.g. muscle spindle sensitivity, total number of joint mechanoreceptors, intrafusal, and chain fibres, as well as the central nervous system, e.g. neural activity in the premotor cortex, cerebellum, and the proprioceptive regions of the basal ganglia and grey matter volume in the precentral gyri, postcentral gyri, insula, and angular gyri.
Joint position sense in the ankle is affected more than the knee in developmental coordination disorder only
Secondly, the present study demonstrated differences between joints, with larger PE and PEV in the ankle joint compared with the knee joint in children with DCD. These results corroborate previous studies reporting greater proprioceptive impairment in distal joints than proximal joints in patients with stroke and intracranial disorders (34, 35). The theoretical basis for this proximal-distal disparity may involve altered functional connectivity in regional brain networks. Proprioceptive information from the proximal joint is transmitted to and mediated bilaterally by both the ipsilateral and contralateral hemispheres, while afferents from the distal joint are projected to and processed in the contralateral hemisphere only (36). Thus, the significant difference found in proprioceptive acuity between joints may explain possible lesions in certain afferent pathways and/or atypical activations in the proprioceptive-processing neural area in children with DCD.
Proprioceptive acuity in lower extremity joints negatively correlates with balance function in developmental coordination disorder only
Thirdly, the present study found significant negative correlations between proprioceptive acuity in the lower extremity joints (knee and ankle) and balance function in children with DCD. The ankle joint is crucial in maintaining stability, especially for modulating body sway in the anteroposterior direction (37). Furthermore, the knee joint provides stability while standing upright or on an unstable surface, e.g. foam pads (38). Not surprisingly, the present findings demonstrate that children with DCD who display more impaired joint position sense tend to have worse balance performance. This implies that the proprioceptive status in the lower extremities can predict balance function in children with DCD. However, previous studies did not show correlations between proprioceptive acuity in upper extremity joints (elbow and wrist) and manual dexterity sub-score (5, 6). The question then becomes, why is proprioception in lower extremities significantly associated with gross balance function, but proprioception in upper extremities not related to fine motor skills? A reasonable explanation may be that fine motor skills draw on a wider range of abilities, e.g. visual control, visual perception, and eye hand coordination, so joint position sense in upper extremities contributes less to fine motor performance. Furthermore, the knee joint matching test resembled a sitting position with the angular range required for sit-to-stand. Studies have documented the knee joint largely contributes to lifting body weight during sit-to-stand (39). Without effective knee joint control, i.e. desired trajectory of joint angle, it is difficult to smoothly transfer centre of mass upward from a stable seated position to a relatively less stable standing position, while simultaneously maintaining body equilibrium. Proprioceptive acuity of the knee joint may be related to functional sit-to-stand movement. However, data on sit-to-stand performance were unavailable in this study. Further studies could investigate the relationship between sit-to-stand performance and position sense acuity of the knee joint in children with DCD.
Due to strict inclusion criteria for children with DCD, balance sub-score data were not normally distributed in this study. Considering the inclusion criteria, as well as the high heterogeneity of DCD (2), the results of the current study cannot be generalized to all children with DCD. Also, the balance domain of the MABC-2 is a relatively narrow distribution for the standard score for some tests. Take “hopping on the mat” for example. For the 10–12-year age group, 5 consecutive hops with the preferred leg gives a standard score of 11, while 0–4 hops yields an identical standard score of 1. However, participant ages were spread across 2 age bands of the MABC-2, i.e. age band 2 (7–10 years), and age band 3 (11–16 years). Given the number of participants in each group and that test items differed between age bands, it was not appropriate to compute correlation coefficients for the DCD and TD groups using the raw score for each test item. To further this research line, prospective studies should consider all these aspects, i.e. recruiting various subtypes of DCD, focusing on a single age band for children, and calculating correlation between proprioceptive acuity and raw score on test items for MABC-2.
Limitations and future directions
A major limitation is the possible reliance on working memory. The contralateral joint position test involves matching a reference angle with the opposite limb, which requires no memory demands, whereas the ipsilateral joint position test requires remembering a previous joint angle. The ipsilateral joint position matching test inevitably involves working memory. A previous study suggested the effect of working memory on ipsilateral joint position matching performance is minimal, as no differences were detected between ipsilateral and contralateral joint position tests (5). Still, from the ipsilateral joint position matching test, we cannot fully exclude working memory as a potential influence in the current study. More studies should investigate proprioceptive acuity in lower extremities using contralateral joint position matching tests in children with DCD. Moreover, no participants were inattentive or distracted during experiments. However, our study did not measure attention bias between groups before and during the proprioceptive test, and the whole experimental procedure lasted 30–40 min, including set-up, instruction, demonstration, practice, and formal test trials. Therefore, whether or not the results were confounded by between-group differences in attention is speculative. Further investigations comparing how attention impacts proprioceptive acuity between children with and without DCD are recommended. Lastly, a variety of interventions, e.g. vibration, manual therapy, taping and bracing, and exercise, have been used to enhance proprioception (23, 40). However, no such interventions have improved proprioception in children with DCD. Furthermore, enhancing joint position acuity does not automatically adapt or facilitate balance performance. Future research should examine which intervention is more effective and efficient in addressing proprioceptive deficits in lower extremities, as well as whether changes in joint position sense promote motor function and skill in lower extremities in children with DCD.
Conclusion
This study verified that impaired joint position sense of knee and ankle joints occurs in children with DCD. In addition, the position error and position error variability in ankle joints is much larger than in knee joints for the DCD group. Lastly, the severity of proprioceptive deficits in knee and ankle joints is negatively associated with balance performance in children with DCD.
The authors thank Chien-Chu Kao for her assistance with figure production. This work was supported by the Ministry of Science and Technology, Taiwan (108-2410-H-017-018).
Conflicts of interest. The author had no interests which might be perceived as posing a conflict or bias. This work was supported by Ministry of Science and Technology in Taiwan (grant number 108-2410-H-017-018). The author certified that the submission is original work, and is not presented as an abstract/poster/oral or as a full article in any national or international conference.
Appendix I. Position error data in each age group of children with Developmental coordination disorder (DCD), and typically developing (TD) children
Appendix II. Position error variability data in each age group of children with Developmental coordination disorder (DCD), and typically developing (TD) children
Appendix III. Correlation between proprioceptive acuity data and subscore in children with DCD, and TD children


 Click to show fullsize
Click to show fullsize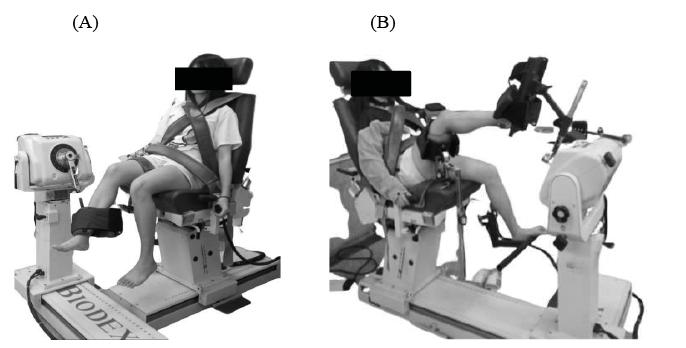 Click to show fullsize
Click to show fullsize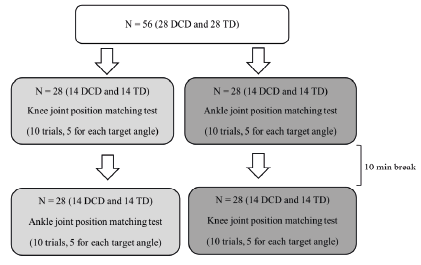 Click to show fullsize
Click to show fullsize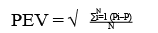 Click to show fullsize
Click to show fullsize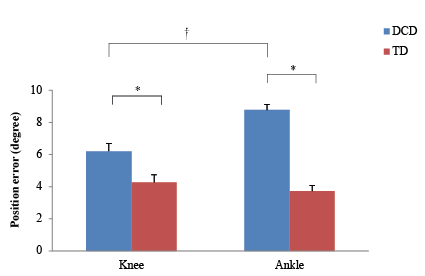 Click to show fullsize
Click to show fullsize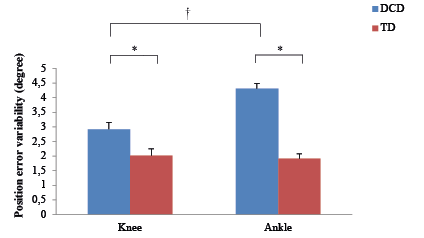 Click to show fullsize
Click to show fullsize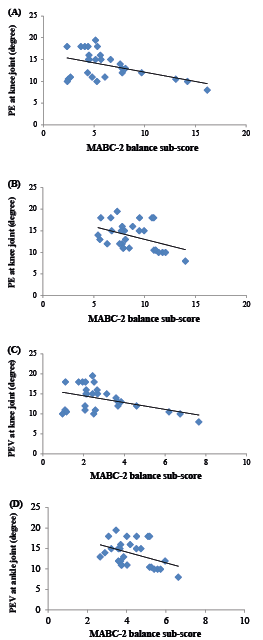 Click to show fullsize
Click to show fullsize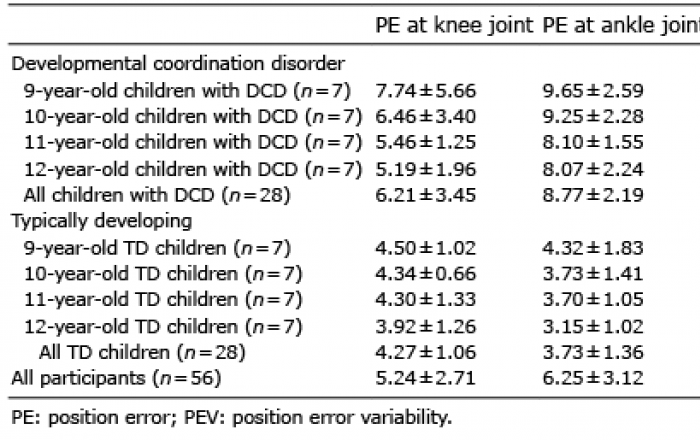 Click to show fullsize
Click to show fullsize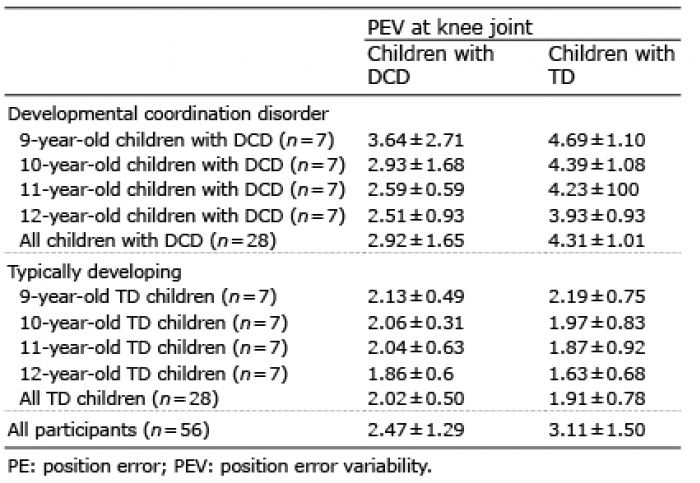 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize