
From the Department of Community Medicine and Rehabilitation; Umeå University, Umeå, Sweden
Background: The long-term impact of transient ischaemic attack is largely unknown.
Objectives: To assess the long-term perceived impact of transient ischaemic attack and explore the influence of sex and age on these perceptions; and to evaluate the relationships between activities of daily living, participation and overall recovery, and the other domains of the Stroke Impact Scale 3.0 (SIS).
Methods: A retrospective study among adult community-dwelling individuals from 6 months up to 10 years after onset of transient ischaemic attack. A total of 299 survivors of transient ischaemic attack responded to the SIS.
Results: Most self-reported disabilities involved emotion, strength, and participation domains of SIS and remained stable until 10 years post-transient ischaemic attack. Women reported significantly more disabilities for emotion and hand function. Elderly subjects (age > 65 years) reported more disabilities for strength, mobility, hand function, activities of daily living/instrumental activities of daily living, and participation. The activities of daily living/instrumental activities of daily living, participation, and overall recovery demonstrated significant, although low-to-moderate, associations with other SIS domains after transient ischaemic attack.
Conclusion: The broadly perceived disabilities were demonstrated consistently and played a significant meaningful role in everyday life and recovery among community-dwelling individuals up to 10 years after a transient ischaemic attack. These findings indicate the need for long-term multi-professional follow-up with holistic rehabilitation to improve overall recovery among survivors of transient ischaemic attack.
Key words: transient ischaemic attack; perceived impact; Stroke Impact Scale; long-term outcome; daily activity; participation.
Accepted Feb 16, 2021; Epub ahead of print Mar 3, 2021
J Rehabil Med 2021; 53: jrm00167
Correspondence address: Xiaolei Hu, Department of Community Medicine and Rehabilitation, Umeå University, 901 85 Umeå, Sweden. E-mail: xiaolei.hu@umu.se
Doi: 10.2340/16501977-2808
The long-term impact of transient ischaemic attack is largely unknown. The aims of this study were to assess the long-term patient-reported impact of transient ischaemic attack and explore the influence of sex and age on these perceptions. A further aim was to evaluate the relationships between activities of daily living, participation, and overall recovery with the other domains of the Stroke Impact Scale 3.0 (SIS). This study assessed various patient-reported disabilities among 299 survivors of transient ischaemic attack, from 6 months until 10 years after onset of transient ischaemic attack, using patient-reported SIS outcome measures. The results showed that most self-reported disabilities involved the emotion, strength, and participation domains of SIS and remained stable until 10 years post-transient ischaemic attack. Women reported higher levels of disabilities than men. There was a correlation between increased age and levels of self-reported disabilities for both men and women. These patient-reported disabilities showed significant, although low-to-moderate, associations with activities of daily living, participation, and overall recovery. The findings suggest a long-term need for general follow-up and rehabilitation among individuals after transient ischaemic attack.
A transient ischaemic attack (TIA) is defined as a sudden focal neurological deficit that completely resolves within 24 h (1). The incidence of TIAs in Sweden is approximately 10,000 each year (2). Due to the increased occurrence of ischaemic stroke following a TIA, increasing attention has been focused on stroke prevention after a TIA. This may lead to an underestimation of the remaining disabilities and the need for rehabilitation after a TIA (3). Although a TIA is transient by definition, previous studies have suggested that some patients experience persistent problems, including motor impairments, cognitive and psychological impairments, mental fatigue, and problems in daily life (4–6). However, definitive descriptions of TIA disabilities remain elusive. Furthermore, most long-term studies on TIA impact have often been reported within the first year after onset of TIA (5, 7). Thus, there is a need to evaluate long-term disabilities after a TIA.
The Stroke Impact Scale 3.0 (SIS) is a self-reported outcome measure designed to assess 8 physical aspects and dimensions of health-related quality of life: strength, memory and thinking, emotions, communication, mobility, hand function, activities of daily living/instrumental activities of daily living (ADL/IADL), and social participation (8). SIS has also been commonly used with both stroke and mild-stroke patient populations (9–11). Thus, SIS may provide a holistic view of TIA impacts, since it covers body function, activity, and participation, 3 first-dimension components of the International Classification of Functioning, Disability and Health (ICF) (12).
Considerable evidence has demonstrated a decline in daily activities and social participation among persons following a stroke, and this decline has been influenced by a variety of functional components, including cognition, motor, and emotion (13–15). Some studies have shown that demographic factors, such as older age and female sex, are related to less favourable outcomes after stroke (16–18). Compared with stroke, TIAs often result in similar, but subtle, disabilities. Little is known about whether these subtle disabilities and demographic factors could be connected to ADL/IADL limitation, participation restriction, and overall recovery after TIA.
To identify potential risk factors for unfavourable outcomes and provide more targeted rehabilitation interventions for patients after a TIA, this study aimed to assess the long-term perceived impact of TIA, and explore the influence of sex and age on these perceptions. The study also evaluated the relationships between the ADLs, participation, and overall recovery with the other SIS domains.
Ethics
Ethics approval was obtained from the regional Ethical Review Board in Umea, Sweden (Dnr 2016-355-32M). Written consent was obtained from all participants prior to inclusion in the study.
Study design and participants
This retrospective study included only individuals after their first-ever TIA. The study was conducted at the Department of Neurological Rehabilitation, University Hospital of Umeå, Sweden. All patients, 18 years or older, admitted to the Stroke Centre, University Hospital of Umeå, Sweden, between 2008 and 2018, and diagnosed with a TIA, were assessed for study eligibility. Exclusion criteria were: (i) recurrence of TIA, early stroke/TIA, or stroke after TIA; (ii) brain tumour, epilepsy, or sinus thrombus; (iii) death; and (iv) inability or unwillingness to provide written consent or answer the questionnaires.
Data collection and questionnaires
The questionnaires, information about the study, and written consent were sent to all eligible participants who were 6 months to 10 years after TIA onset during the autumn of 2018. The questionnaires and signed consent were returned before the end of 2018. In cases of missing data, complementary information was collected through phone calls with patients. However, the questionnaires were re-sent to a participant if a large amount of data was missing. All participants provided written informed consent to participate in the study. Demographic data that included age, sex, and co-morbidities were obtained from patient records.
Modified Rankin Scale questionnaire
The Modified Rankin Scale questionnaire (mRSq) is a standardized, pragmatic, validated tool to help reliably score a person’s disability (19, 20). Five questions are answered “yes” or “no” by the patient. A scale rating from 0 (no symptoms) to 5 (total physical dependence) is then rated by following the mRSq flowchart. mRSq scores ≤ 2 are considered to represent total independence (19).
Stroke Impact Scale 3.0
The Stroke Impact Scale 3.0 (SIS) comprises 59 questions representing 8 domains: strength, memory and thinking, emotions, communication, mobility, hand function, ADL/IADL, and social participation (8). Each question is answered using the Likert scale, ranging from 1 to 5 (8, 21), with higher scores indicating better outcomes. For the strength domain, the ratings range from “no strength at all” to “a lot of strength;” for emotions and participation, choices range from “none of the time” to “all of the time;” for the remaining domains, the ratings range from “extremely difficult/cannot do at all” to “not difficult at all” (9). Also, the SIS includes a visual analogue scale, where 0 represents no perceived stroke recovery and 100 represents full recovery (8). Scores < 100 were defined as not fully recovered from the TIA.
Data presentation and statistics
All data processing was conducted blinded. The data were inclusive from 6 months to 10 years after onset of TIA. To increase the statistical power for comparing SIS domain differences over time, participants were divided into 3 groups: < 1 year post-TIA, 1–5 years post-TIA, and > 5 years post-TIA. The no-limitation percentages were calculated based on the number of full-recovery participants (SIS scores of 100) divided by the total number of participants. Age > 65 years was defined as “old,” and ≤ 65 years was defined as “young.” Since there were no significant differences in SIS domains between the 3 time-groups, all time-group participants were included when analysing the influences of age and sex on SIS domains, as well as correlations between SIS domains and ADL/IADL, participation and recovery.
SIS data were converted to scores between 0 and 100 for each domain (standardized score = [(actual raw data−1)/(5−1)] × 100), where 100 represented the best condition and 0 the worst (8). Here, standardized scores between 90 and 100 in any individual domain were defined as mild/subtle impairments, limitations, and restrictions. The continuous variables in demographic characteristics and converted SIS scores were presented as mean (standard deviation; SD). The categorical variables in demographic characteristics were presented as numbers and percentages. Differences in SIS scores between the 3 time-groups were compared using an ordinary 1-way analysis of variance (ANOVA). Differences in demographic and clinical characteristics between groups were compared using an ordinary 1-way ANOVA for continuous variable data or a χ2-squared test for categorical variables. Two-group differences were compared with t-tests for independent samples.
Correlations between various SIS domains and respective ADL/IADL, participation, and overall recovery were analysed with Pearson’s correlation coefficients. All participants were included in the analyses. The correlation coefficient strengths were defined as: < 0.5 = low correlation, 0.5–0.7 = moderate correlation, and > 0.7 = high correlation (22).
Statistical analyses were performed using GraphPad Prism, v.8 (San Diego, CA, USA). A p-value < 0.05 was considered statistically significant.
Participant recruitment and their characteristics
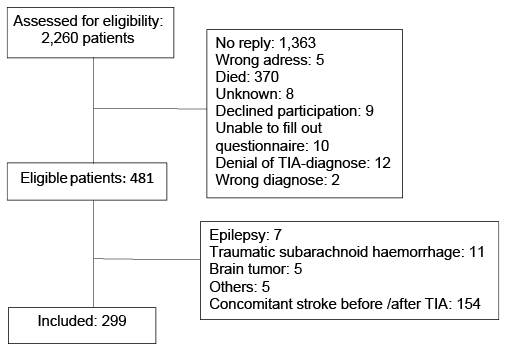
A total of 2,260 patients with a diagnosis of TIA were assessed for study eligibility. Of these, 481 eligible individuals consented to participate after having received written information about the study. The response rate was 26%. The most common reasons for exclusion were recurrence of TIA, early stroke/TIA, or stroke after TIA (n = 154). A final total of 299 participants, each with a first-ever TIA between 2008 and 2018 and meeting the other inclusion criteria, were recruited to participate in the study (Fig. 1).
Fig. 1. Flowchart of study inclusion process. TIA: transient ischaemic attack.
Participant characteristics are summarized in Table I. Their mean age was 72 years, with more than 80% of participants older than 65 years. Males represented 56% of participants, and females 44%. Hypertension was the most common co-morbidity. Functional outcomes, assessed by the mRSq, showed that approximately 91% (271/299) of participants were independent and able to live alone without any help from other people (mRSq values 0–1), and only 9% (27/299) were dependent (mRSq values 2–5). No significant difference in mRSq was observed between females and males, or between younger and older participants (Table II).
Table I. Demographic and clinical characteristics of all participants
Table II. Differences in various Stroke Impact Scale (SIS) domains and Modified Rankin Scale questionnaire (mRSq) score between sex and age groups
There were no statistically significant differences between the 3 time-groups (i.e. < 1 year post-TIA, 1–5 years post-TIA, and > 5 years post-TIA) for age, sex, co-morbidities, or mRSq values (Table I).
SIS domains
More than four-fifths of participants reported emotional problems (mean value 80.6) when all time-group participants were included (Table III), and almost half reported reduced strength (mean value 84.2). More than one-third of participants reported participation restrictions (mean value 89.1) among the SIS domains even though most (78%) were living independent lives, as demonstrated by mRSq scores (Table I). Other SIS domains, including memory and thinking, communication, ADL/IADL, mobility, hand function, and recovery, were also reported to have subtle perceived difficulties (mean value > 90). No significant differences were found in all SIS domains between the 3 time-groups up to 10 years after the TIA. There were 198 participants (66.5%) who experienced full recovery after their TIAs, and their perceived disabilities were stable without significant differences between the 3 time-groups (Table III).
Table III. Degree of disability presented by Stroke Impact Scale (SIS) scores (Mean (standard deviation; SD)). p-value tested by analysis of variance (ANOVA) test between 3 groups
As shown in Table II, female participants reported significantly more emotional disabilities than male participants (p = 0.03), male participants had better hand function than females (p = 0.03), and older TIA survivors reported significantly more disabilities for strength, mobility, hand function, ADLs, and participation compared with younger survivors.
The associations between ADL/IADL, participation, and overall recovery, and the other SIS domains are shown in Table IV. Perceived limitations of mobility showed moderate significant correlations between ADL/IADL (r = 0.62 and p < 0.0001) and participation (r = 0.67 and p < 0.0001). Moreover, the perceived difficulties for hand function also showed a moderate significant correlation with ADL/IADL (r = 0.55 and p < 0.0001) (Table IV), and the correlation between daily activities and participation was also moderate (r = 0.70 and p < 0.0001). The patient-reported reduced strength, limitations of memory/thinking and emotion demonstrated low, but significant, correlations with ADL/IADL and participation. The overall recovery demonstrated a significant moderate correlation with participation, while other SIS domains only showed low, but significant, correlations (Table IV).
Table IV. Correlations between Stroke Impact Scale (SIS) domains and activities of daily living/instrumental activities of daily living (ADL/IADL), participation and recovery
Using the SIS, this study demonstrated that patient-reported disabilities mostly involved emotion, strength, and participation, whereas only subtle perceived difficulties were found for memory/thinking, mobility, hand function, and communication among community-dwelling individuals after TIA. These perceived disabilities remained stable, with a similar prevalence from 6 months to 10 years after TIA. Women reported significantly more disabilities for emotion and hand function, while elderly subjects (age > 65 years) reported more disabilities for strength, mobility, hand function, ADL/IADL, and participation. The ADL, participation, and overall recovery demonstrated significant, although low-to-moderate, associations with other SIS domains after TIA.
Emotional problems were the most common patient-reported disability by almost four-fifths of the participants during the 10-year range of follow-ups in the study. The current results confirmed those of previous studies, in which TIA increased psychological impairments 6–48 months after TIA onset (4, 23, 24). Meanwhile, the current data extend the time course for perceived emotional problems up to 10 years after TIA. This indicates that a TIA may cause emotional problems long after its onset among community-dwelling individuals (25). Compared with the male TIA participants, female participants reported significantly more emotional difficulties no matter their age. This is in line with a previous study, in which female stroke survivors experienced more emotional difficulties than men (26), which implies that the sex difference regarding the emotional issue may occur because women express their emotional issues better than men. The current findings indicate that more attention should be paid to emotional issues among TIA survivors, since a TIA increases the vulnerability to late-life emotional difficulties.
Even though a TIA does not, by definition, result in permanent motor impairments, reduced strength was the second-most perceived impairment among more than 40% of participants up to 10 years post-TIA. This finding confirms and extends the time-course for reduced strength reported at 12 months after TIA (27). Together with undiagnosed minor stroke and reduced physical activity (27), the reduced strength may partly contribute to mobility limitations reported by one-third of participants, mostly the elderly participants, in the current study. These results suggest that long-term rehabilitation focusing on physical activity is needed to improve motor impairment and to delimitate their long-term negative impacts on daily life among individuals after a TIA, especially among elderly subjects.
More than 90% of participants lived independently (mRSq values 0–1), with only 20% having subtle ADL/IADL limitations. This is not surprising, since previous studies have reported that the majority of TIA survivors are generally independent in their ADL/IADL (4, 5, 7, 28). Despite the high level of independence, more than one-third of participants reported participation restrictions without full recovery after TIA, especially among elderly subjects. These results indicate that one-third of individuals after TIA may struggle with more complex activities, including various family, social, and work situations, although they live an independent life. Furthermore, the self-reported participation restrictions demonstrated more association with the perception of incomplete recovery than the other SIS domains. This is consistent with the finding among persons after stroke, who consider social participation as a major aspect of their recovery (29). The results of the current study imply a need for rehabilitation interventions focusing on participation issues among TIA survivors for improving their recovery (30).
The current study demonstrates that elderly subjects (age > 65 years), no matter their sex, report more disabilities for strength, mobility, hand function, ADL/IADL, and social participation. This indicates that higher age is a potential risk factor for the deterioration of outcomes after a TIA. In addition, the limitations on mobility and hand function were moderately related to limitations of ADL/IADL. This, again, emphasizes the importance of physical activity for a person after a TIA. Moreover, impairment of strength, limitations on memory and thinking, emotion, and communication also demonstrated weak, but significant, associations with limitations of ADL/IADL tasks and participation restrictions. The present findings suggest that the various subtle disabilities after TIA may play a significant meaningful role in everyday life and recovery from 6 months to 10 years after onset of TIA. Consistent with similar findings among stroke patients (13–15), the current data indicate that a multi-professional follow-up using holistic rehabilitation may be required to reduce these negative consequences on ADL/IADL, participation, and to improve overall recovery (31). To date, however, there have been no clinically routine rehabilitation interventions provided to TIA survivors in Sweden.
Study strengths and limitations
The main strengths of the current study were the relatively large sample size and the long-term follow-up period, which made it possible to study TIA-impact differences between survivors up to 10 years after onset of TIA. On the other hand, very long-term follow-ups may also have weaknesses. The possibility that other comorbidities may have influenced SIS domains cannot be ruled out. Various comorbidities, such as hypertension, diabetes, and heart disease among participants, may have partially affected the outcomes of SIS domain assessments in addition to the TIAs. Furthermore, possible changes in the SIS data could not be studied over time, since the individuals were recruited at different time-points after TIA onset. Caution should also be exercised due to the low total-response rate, lack of a control group, and inclusion in the study only of survivors living in the community. Another caveat is that no objective assessments of cognitive or motor functions were performed by the medical staff, even though the use of the SIS has been well-validated in both stroke and TIA patients. Given these limitations, the assessments in the current study have been made with due caution.
Conclusion
In conclusion, broadly perceived disabilities were demonstrated consistently and played a significant meaningful role in the everyday life and recovery of community-dwelling individuals from 6 months up to 10 years after TIA. Women and elderly people were more likely to report more disabilities. These findings indicate a need for long-term multi-professional follow-up with holistic rehabilitation interventions, including physical activity, to improve overall recovery among survivors of TIA.
This study was supported by the Västerbotten County Council and Umeå University (ALF Foundation), the Swedish Stroke Foundation (Stroke Riksförbundet), and the Northern Swedish Stroke Fund (Strokeforskning i Norrland Insamlingsstiftelse).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize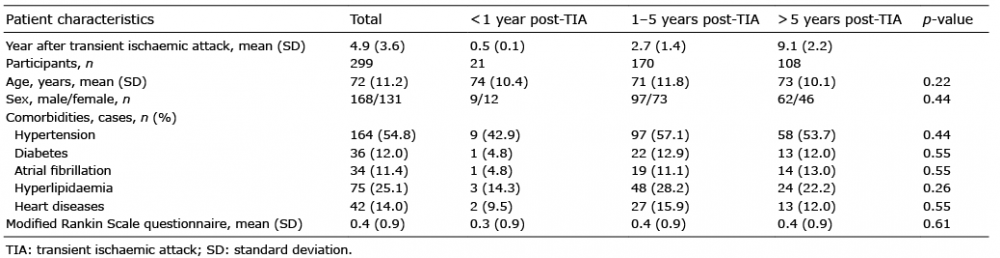 Click to show fullsize
Click to show fullsize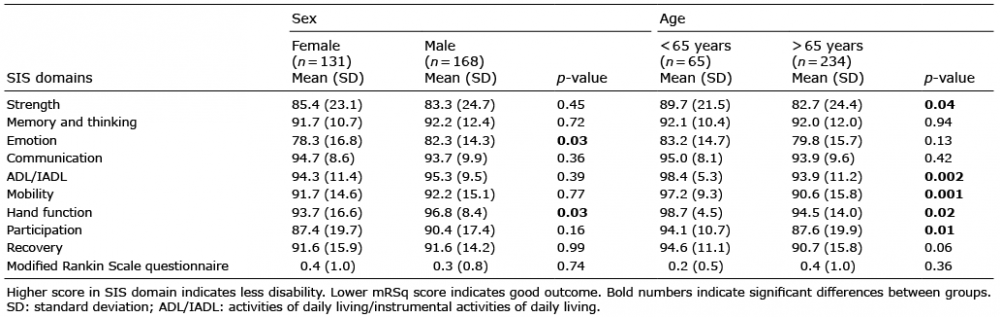 Click to show fullsize
Click to show fullsize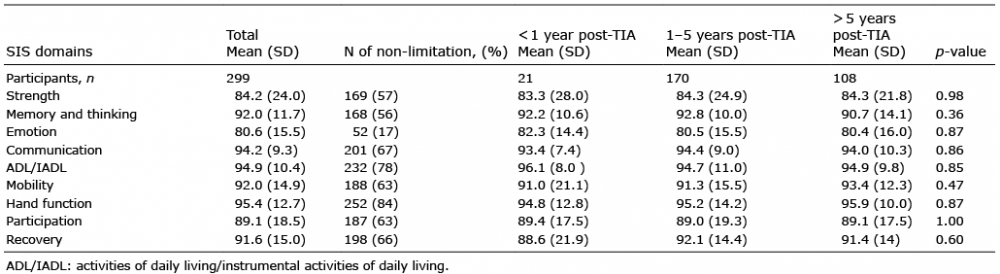 Click to show fullsize
Click to show fullsize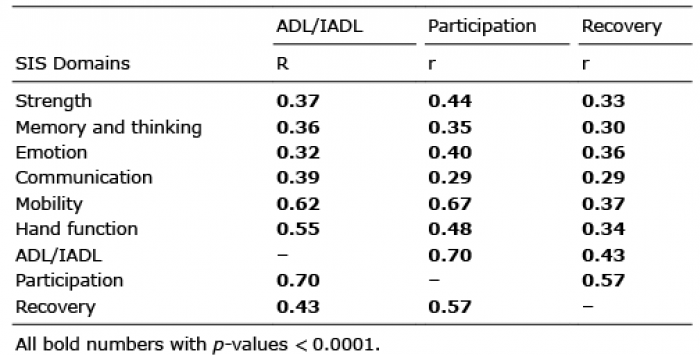 Click to show fullsize
Click to show fullsize