
From the 1Institute of Neuroscience and Physiology, Rehabilitation Medicine, University of Gothenburg, 2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital and 3Rehabilitation Medicine, Neurocare, Sahlgrenska University Hospital, Gothenburg, Sweden. *These authors contributed equally to this work.
Objective: Depression and impaired cognition are common consequences of stroke. The aim of this study was to determine whether cognitive impairment 36–48 h post-stroke could predict self- reported feeling of depression 3 months post-stroke.
Design: A longitudinal, cohort study.
Patients: Patients aged ≥ 18 years at stroke onset.
Methods: Cognition was screened using the Montreal Cognitive Assessment, 36–48 h after admission to the stroke unit at Sahlgrenska University Hospital. Information about self-reported feeling of depression 3 months post-stroke was retrieved from Riksstroke (the national quality register for stroke in Sweden). Bootstrapped binary logistic regression
analyses were performed.
Results: Of 305 patients, 42% were female, median age was 70 years, and 65% had mild stroke. Three months post-stroke, 56% of patients had self-reported feeling of depression; of these, 65% were female. Impaired cognition at baseline could not predict self-reported feeling of depression 3 months later. The odds for self-reported feeling of depression were twice as high in female patients (odds ratio 2.01; 95% confidence interval, 0.20–1.22; p < 0.01).
Conclusion: Impaired cognition early after stroke could not predict self-reported feeling of depression 3 months post-stroke. Compared with male patients, female patients had twice the odds of self-reported feeling of depression
Key words: stroke; cognition; assessment; depression; self-perceived; prediction; bootstrapping.
Accepted Mar 2, 2021; Epub ahead of print Mar 19, 2021
J Rehabil Med 2021; 53: jrm00170
Correspondence address: Tamar Abzhandadze, Institute of Neuroscience and Physiology, Rehabilitation Medicine, University of Gothenburg, Per Dubbsgatan 14, fl. 3, 413 45 Gothenburg, Sweden. E-mail: tamar.abzhandadze@gu.se
Doi: 10.2340/16501977-2816
Depression and impaired cognition are common consequences of stroke. This study investigated whether screening for cognitive function 36–48 h after stroke could predict self-reported feeling of depression 3 months later. Of the 305 patients with mild stroke, 56% had self-reported feeling of depression. Cognitive impairment could not predict self-reported feeling of depression. Therefore, cognitive screening within the first 2 days after stroke might be too early to predict self-reported feeling of depression 3 months after stroke. However, the high proportion of patients with self-reported feeling of depression indicates the severity of the problem that needs to be addressed.
Post-stroke depression (PSD) is a common condition identified in up to 40% of patients, 3 months after stroke (1–3). Since approximately only 17% of patients with PSD have a previous history of depression, PSD can primarily be considered a consequence of stroke (4). A previous study showed a high number of patients developing PSD in the first month after stroke (5). The prevalence of depression in the acute phase after stroke was 25%, with a slight increase of to 31% after 3 months (5). PSD is associated with increased mortality, decreased quality of life, physical disability, and poor functional outcomes after stroke (6). Therefore, timely detection of depression is important (1), but can be hindered by various factors, such as short duration of hospitalization, insufficient healthcare resources, and poor communication between healthcare facilities (7). Thus, the availability of other information gathered early after stroke that can help predict PSD will be of clinical value.
The mechanisms underlying PSD are complex and associated with multiple factors; including patients’ pre-stroke characteristics, stroke-related risk factors, and post-stroke conditions (8). Impaired cognition has been linked to PSD (9, 10). Executive dysfunction, language impairment, and orientation deficits were also related to PSD (11). However, the cause–effect relationship between cognition and depression is unclear. Neurobiological pathways, such as vascular depression and neuroinflammation can cause PSD (12, 13). Nevertheless, none of these can be considered more dominant or the leading cause of PSD. However, these pathways could still be possible causes of PSD, together with cognitive impairment.
Unlike cognitive function, female sex is a well-known predictor of PSD (14, 15). Female patients are also more likely to be widowed before stroke, have a high mean age, more severe stroke, and a higher level of post-stroke disability (14). However, the results regarding patients’ age and risk of PSD are conflicting, indicating that both young and old patients have a high risk of PSD 3–12 months after stroke (14, 16, 17). Furthermore, patients younger than 70 years have a high risk of PSD (16, 18). Other well-known predictors of PSD are severe stroke, stroke localization, high dependency level, and social isolation post-stroke (15, 16).
The predictive value of cognitive function for PSD remains unclear. Moreover, no studies were found that assessed the association between screening of cognition very early post-stroke and self-reported feeling of depression (SRFD) 3 months after stroke, when the first post-stroke follow-up is commonly done. Thus, the primary aim of this study was to explore the association between cognitive function screened very early after stroke and SRFD 3 months later. The secondary aims were to study the influences of sex and age on cognition and SRFD 3 months post-stroke.
Study sample
In this longitudinal, cohort study, baseline data were obtained from a research database that was created as a consequence of the Gothenburg Very Early Supported Discharge study (GOTVED) (19). For GOTVED, patients admitted to a stroke unit at Sahlgrenska University Hospital (SU) from May 2011 to April 2016 were screened and registered (19). The SU was, at the time, the only hospital in Gothenburg performing thrombolysis and the only hospital in the Region Västra Götaland performing thrombectomy. Baseline data were merged with data in the Swedish national quality register for stroke care (Riksstroke) (20, 21). The primary aim of Riksstroke is to gather data for the assessment of stroke care quality and rehabilitation at stroke units. However, another aim is to make data available for research. The statistician at Riksstroke merged the data by using the patients’ personal identification numbers. The data file received was anonymized. The acute and 3-month follow-up forms of Riksstroke were used. The study was approved by the Regional Ethics Review Board in Gothenburg (number 042–11, amendments 392–17 and 966–17).
Inclusion criteria were: patients with ischaemic and/or haemorrhagic stroke, who were aged ≥18 years at stroke onset; who spoke and understood Swedish; had been cognitively screened using the Montreal Cognitive Assessment (MoCA) within 36–48 h after admission, and returned the 3-month follow-up questionnaire with data on SRFD. Patients with other concomitant neurological diseases were excluded.
Procedure
Research database. Occupational therapists in the stroke unit screened the patients’ cognitive function and the ability to perform basic activities of daily living (ADL) within 36–48 h after admission to the stroke unit. The occupational therapy department at SU collaborated with the research group during the screening period of the GOTVED study (19). Data on stroke type and neurological status at stroke onset were gathered from the patients’ charts. Stroke-related neurological status at arrival was assessed by trained staff (a nurse or a doctor).
Riksstroke. Data in the acute modulus were registered by personnel in a stroke unit. The 3-month follow-up was completed with self-administered questionnaires.
Variables
The outcome variable was SRFD, estimated from Riksstroke’s 3-month follow-up module. The question “do you feel depressed?” had multiple-choice responses, which were dichotomized for the analysis in this study. There were 4 options: never/nearly never, sometimes, often, or constantly. The option “never/nearly never” was categorized as “do not have SRFD” and coded as 0. The options “sometimes”, “often”, and “constantly” were categorized as “have SRFD” and coded as 1 (22).
The primary explanatory variable was cognitive function screened by the MoCA: the maximum score on MoCA was 30, and a cut-off score ≥ 26 indicated normal cognitive functioning (23). For the binary logistic regression analyses, the MoCA was dichotomized into normal cognition (MoCA score ≥ 26) and impaired cognition (MoCA score ≤ 25) (23). The secondary explanatory variable was the patients’ sex.
Subgroup analyses were performed based on the patients’ age at stroke onset. For the binary logistic regression analyses, age was dichotomized as follows: group 1 included patients aged 19–69 years, and group 2 included patients aged 70–100 years. The cut-off was chosen based on a previous study showing that patients younger than 70 years have a high risk of depression (18).
Other variables used in the study
The neurological status at hospital admission was assessed using the National Institutes of Health Stroke Scale (NIHSS) (24). The NIHSS is a clinical assessment scale used to evaluate stroke severity. The score ranges from 0 to 42, with a higher score indicating more severe stroke. For the logistic regression analyses, the NIHSS score was dichotomized as mild stroke (NIHSS score ≤ 2) and moderate to severe stroke (NIHSS score ≥ 3) (24).
The patients’ independence in P-ADL was assessed using the Barthel Index (BI) (25), a standardized tool for measuring a patients’ ability to perform P-ADL. The total score on the BI ranges from 0 to 100, with higher scores indicating higher independence in ADL. For the logistic regression analyses, the BI was dichotomized as ADL-independent (BI ≥ 95) and ADL-dependent (BI ≤ 90).
Moreover, data on comorbidities (diabetes and previous stroke, yes/no), living conditions and ADL before stroke onset, stroke type (ischaemic and haemorrhage), reperfusion treatment (coded as yes for patients who received thrombolysis and/or thrombectomy and no for those who did not receive reperfusion treatment), hospitalization duration, and discharge destination from the hospital were registered and analysed.
Statistical analysis
The characteristics of the study sample are presented with descriptive statistics. Significant differences between included and excluded patients, as well as those between male and female patients were studied using the Mann–Whitney U test and χ2 test for continuous/ordinal variables and nominal variables, respectively.
Binary logistic regression analyses
The outcome variable was SRFD 3 months after stroke, coded as “do not have SRFD “ = 0 or “have SRFD “ = 1. The following independent variables were analysed: cognitive function assessed with the MoCA (primary explanatory variable, dichotomized), sex (secondary explanatory variable), age (dichotomized), stroke severity as assessed with the NIHSS score (dichotomized), living alone, diabetes, previous stroke, ADL assessed with BI (dichotomized), and stroke type (Table SI). The independent variables were chosen based on previous literature and the authors’ clinical experience.
Assumption checking. Independent variables were checked for ≥ 10 observations per outcome category. In addition, the collinearity between independent variables was studied with phi correlation coefficients, since all independent variables were binary. The independent variables with a correlation coefficient of ≥ ±0.7 were not entered in the same model.
Model building. Three binary logistic regression models were built. In model 1, the primary independent variable, MoCA, was entered. In model 2, patients’ sex and MoCA were entered. Finally, the third model was based on 9 independent variables, including the primary and secondary explanatory variables (model 3). B coefficients and odds ratios (ORs) were presented for each independent variable.
Model stability. The sample size was relatively small. To investigate the model stability, simple bootstrapping was performed with 2,000 samples with replacement from the original dataset (23–25). Bootstrapped standard errors (SE, lower values were better), bias-corrected and accelerated 95% confidence intervals (95% CIs), and p-values were reported.
Evaluation of binary logistic regression models. The fit of the binary logistic regression model was evaluated with the Hosmer–Lemeshow test (p > 0.05 indicates good fit). The explained variance of the models was evaluated with Cox & Snell’s R2 and Nagelkerke’s R2 tests (higher values were desired), and the Omnibus test (χ2 test, p-value ≤ 0.05 was desired).
Data were analysed using SPSS (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.); for bootstrapped logistic regression, the SPSS professional demo version was used. All tests were two-sided at a 5% significance level.
Subgroup analyses
Subgroup analyses for predicting SRFD were also performed. The patients’ sex and age were used as control variables.
Study participants
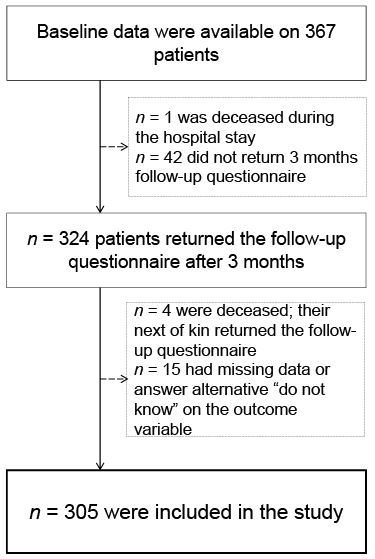
Baseline data were available for 367 patients (Fig. 1). Of these, 305 met the inclusion criteria. The excluded patients (n = 62) and included patients (n = 305) showed no significant differences in terms of sex (p = 0.82), age (p = 0.38), or stroke severity (p = 0.35) (Fig. 1). However, the excluded group contained a greater proportion of patients with severe cognitive impairment (median MoCA score, 22; p = 0.001) and patients who were ADL-dependent (median BI, 87.5, p = 0.05) 36–48 h post-stroke.
Fig. 1. Flow chart of the study participants with stroke.
Of the 305 patients included in this study, 58% were female, and the median age was 70 years (range 19–100 years); 199 (65%) patients had mild stroke, 184 (60%) had impaired cognition (MoCA score ≤ 25), and 127 (42%) were ADL-dependent (BI ≤ 90). A significantly greater proportion of females were living alone before stroke, and a significantly greater number of males had prior stroke (Table I).
Three months after stroke, 170 (56%) patients reported that they did not need assistance from relatives, 251 (82%) patients were living in their own homes without community services, and 112 (37%) were living alone. Regarding SRFD, 135 (44%), 145 (47%), 18 (6%), and 7 (3%) patients reported feeling depressed never/nearly never, sometimes, often, or constantly, respectively. There was no significant difference in SRFD between the patients who were cognitively impaired (MoCA score ≤25) and the remainder (MoCA score ≥26); p = 0.46 (Fig. 2). The proportion of female patients (65%) who felt depressed sometimes, often, or constantly was significantly higher than that of male patients (48%; p = 0.002). No significant difference was found between the age groups (p = 0.06), (Fig. 2).
Table I. Characteristics of patients with stoke in the study
Fig. 2. Bar chart showing the proportional distribution between patients’ cognitive function, sex, age, and self-reported feeling of depression. In total, data from 305 patients with stroke were included. MoCA: Montreal Cognitive Assessment.
Prediction of self-reported feeling of depression 3 months after stroke
The number of observations between the categories of independent and dependent variables was >10 patients (Table SI); thus, they could be pooled into the binary logistic regression model. Furthermore, phi correlation coefficients between independent variables were ≤ ± 0.40, indicating no collinearity between the variables (Table SII).
Cognitive function screened 36–48 h after stroke was not a significant predictor for SRFD in the univariable and multivariable models (Table II). Furthermore, the odds of SRFD were high in female patients. Patients ≥ 70 years had decreased odds of SRFD. The patients who were living alone before stroke had higher odds of SRFD than those not living alone (Table II).
Table II. Binary logistic regression analysis models predicting self-reported feeling of depression in 305 patients with stroke
Sex differences in relation to cognitive function and self-reported feeling of depression 3 months post-stroke
Cognitive impairment could not predict SRFD 3 months post-stroke in the simple and adjusted models (Table SIII). Male patients who lived alone before stroke had two times higher odds for SRFD 3 months post-stroke (OR = 2.35; 95% CI, 0.01–1.95; p = 0.02) than female patients. Furthermore, the odds for SRFD were 71% lower in older (≥ 70 years) female patients (OR = 0.29; 95% CI, –2.41 to –0.39; p = 0.02) compared with the younger female patients (Table SIII).
Age differences in relation to cognitive function and self-reported feeling of depression 3 months post-stroke
Cognitive impairment could not predict SRFD in the univariable or adjusted models for either age group (Table SIV). The models with all explanatory variables showed that, in the age group < 70 years, patients had 3-fold higher odds of SRFD 3 months after stroke if they were living alone before stroke (OR = 3.69; 95% CI, 0.20–3.19; p = 0.007) and three-fold higher odds of SRFD if they were female (OR = 3.56; 95% CI 0.20−2.82; p = 0.008). No significant attributes were identified in the patient group ≥ 70 years of age (Fig. 3). Detailed information is presented in Table SIV.
Fig. 3. Forest plot showing the odds ratios (OR) and 95% confidence intervals (95% CIs) for predicting self-reported feeling of depression 3 months after stroke; 305 patients were stratified on the basis of age. 95% CI and p-values are derived from bootstrapped binary logistic regression analyses. NIHSS: National Institutes of Health Stroke Scale; ADL: activities of daily living; BI: Barthel Index; MoCA: Montreal Cognitive Assessment.
This longitudinal cohort study showed that cognitive function screened with the MoCA could not predict SRFD either in the total sample or in the analyses stratified by sex and age. The current study results differ from those of earlier studies (10, 26, 27), which showed a positive association between impaired cognitive function and depression. According to previous studies (10, 26), depressive patients had severe neurological impairment and were more likely to be ADL-dependent. In these studies, cognitive impairment was assessed using either the Scandinavian Stroke Scale or the Mini-Mental State Examination and the Trail Making test. The patients in the current study had mostly either mild or moderate stroke, which can, in turn, explain why the current results differ from those of previous studies. Theoretically, the inclusion of patients with more severe neurological impairment could have shown a significant relationship between poor cognitive function and SRFD 3 months after inclusion.
Female patients generally had higher odds for SRFD 3 months post-stroke, and younger females (< 70 years) had 3-fold higher odds. These results are in line with those of earlier studies, showing that the female sex is a risk factor for developing PSD (28, 29). In Sweden, approximately every fifth person is diagnosed with depression during their lifetime, and the number of women with this diagnosis is almost double that of men (30). The results of the current study are consistent with this finding; they further validate the generally high odds for depression among women as well as among female patients after stroke.
Patients living alone before stroke showed higher odds of SRFD after stroke in the total sample. This result was consistent with previous findings showing that patients living alone before stroke show increased odds of PSD (1). Moreover, when sensitivity analyses were performed based on sex, the current study found that male patients who were living alone before stroke had higher odds for SRFD 3 months post-stroke. This phenomenon has not been reported previously to the same extent and could be regarded as new information. The reason living alone is a risk factor for SRFD among male patients remains poorly understood and should be assessed more closely in future. There was no significant difference identified among patients aged 70 years. Previous studies reported conflicting results regarding age as a possible risk factor for PSD (16, 17). However, the current study showed that younger patients had higher odds for SRFD, which could be due to disappointment with unexpected change in their aspirations and frustration with loss of their earlier healthy life (31).
Study limitations and strengths
This study has several limitations. The dropout rate between baseline and 3-month follow-up was 17%. The excluded group contained patients with more severe cognitive impairment as well as greater dependency in ADL. A further limitation was that the variable “depression” was extracted from Riksstroke’s 3-month follow-up data, and was based on self-reported feelings. Moreover, it is possible that cognitive impairments identified within 36–48 h after admission to the stroke unit reflect other stroke-related consequences, such as acute delirium, tiredness, and health-related stress reaction; this, in turn, could lead to insignificant results.
The current study also had several strengths. The study sample was relatively large and included a wide age range with verified stroke diagnosis. Most of the patients had mild to moderate stroke (NIHSS score ranged from 0 to 19). The study sample was representative of the Swedish population with stroke, where most patients have mild to moderate stroke at hospital admission. The Riksstroke’s question about depression used in this study has been validated previously by Eriksson et al. (28). However, in their study, different dichotomizations were used for logistic regression analyses. The MoCA has been considered the most valid and clinically practical screening tool for identifying cognitive impairment in stroke patients (31). In summary, the results of the current study can be generalized to the stroke population with mild to moderate stroke.
Conclusion
The results of this study showed that cognitive impairment 36–48 h after stroke, screened using the MoCA could not predict SRFD 3 months after stroke. Moreover, patients aged < 70 years, either female or living alone, had higher odds ratios for SRFD. These findings are clinically important and provide new information about the groups with high odds of developing PSD. A high proportion of patients reported feeling depressed, indicating that the prevalence of depression might be high in stroke survivors. Thus, mood screening is an important aspect of regular follow-up after stroke.
The authors thank the study participants, and would like to acknowledge the occupational therapists at Sahlgrenska University Hospital, who screened the patients.
Study funding. This study was supported by grants from the Swedish Research Council (VR2012-3523, VR2017-00946), the Swedish Brain Foundation, the Swedish Heart and Lung Foundation, Iris Jonzén-Sandblom and Greta Jonzén Foundation, King Gustaf V’s and Queen Victoria’s Freemasons’ Foundation, the Swedish National Stroke Association, the Local Research and Development Board for Gothenburg and Södra Bohuslän, Hjalmar Svensson’s research foundation, FRF foundation, and Promobilia foundation. The study was financed by grants from the Swedish state under an agreement between the Swedish government and the county councils, the ALF agreement (ALFGBG-718711, ALFGBG-877961).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize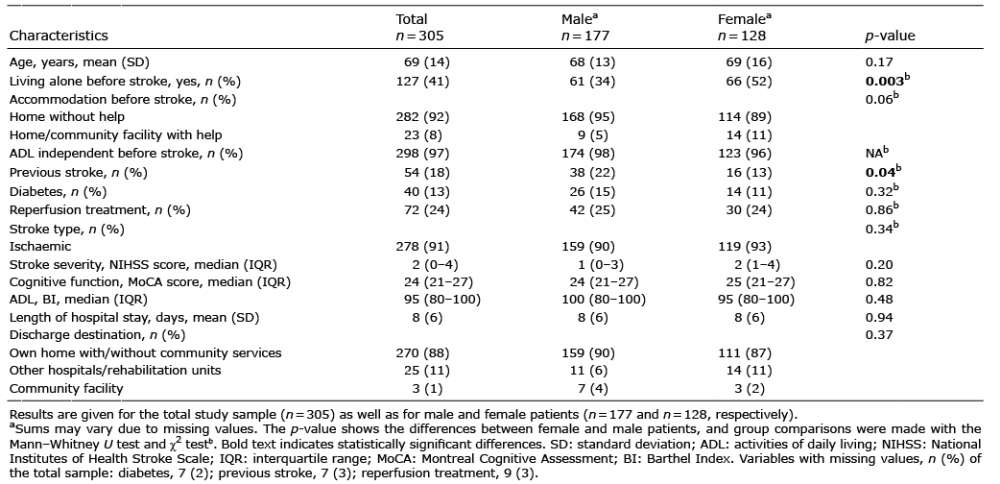 Click to show fullsize
Click to show fullsize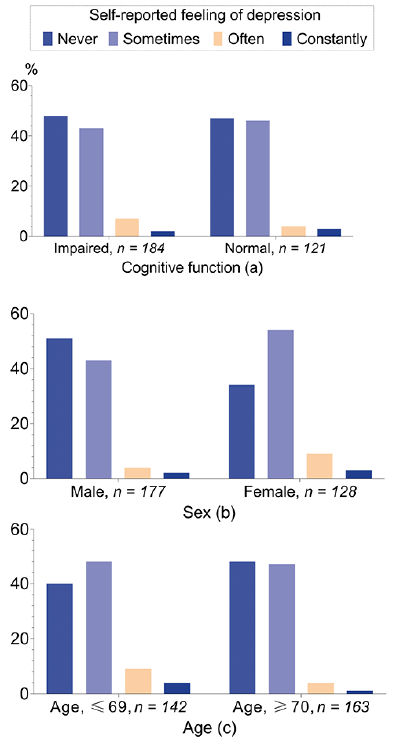 Click to show fullsize
Click to show fullsize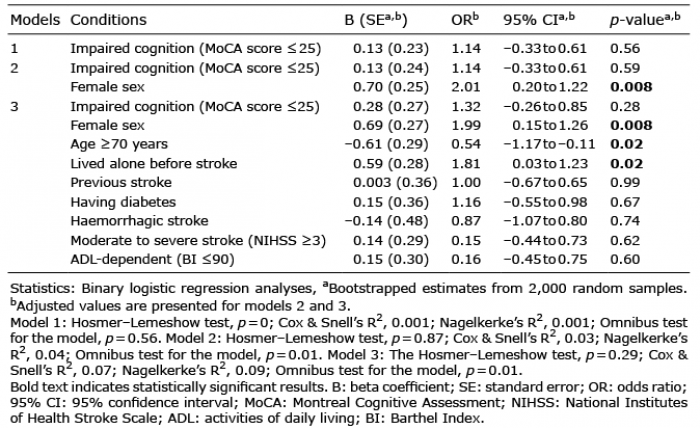 Click to show fullsize
Click to show fullsize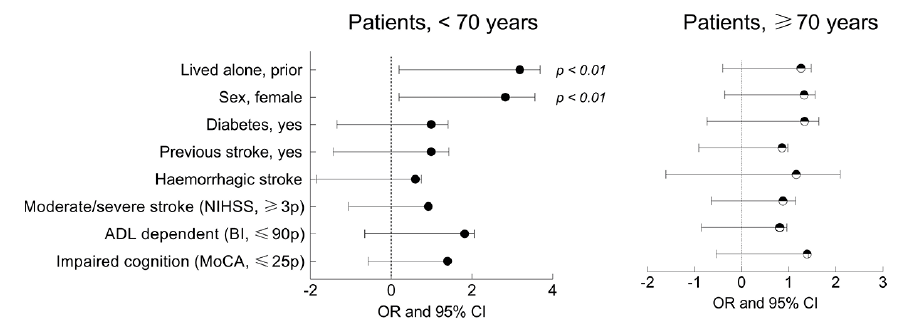 Click to show fullsize
Click to show fullsize