
From the 1Department of Rehabilitation, Shanghai Xuhui Central Hospital, Zhongshan-Xuhui Hospital, Fudan University and 2Department of Medical Technology, Shanghai University of Sport, Shanghai, China
*These authors contributed equally to this manuscript.
Objective: Recent clinical evidence supports that orthopaedic insoles, especially lateral-wedge insoles, can significantly benefit patients with knee osteoarthritis. The aim of this study is to explore the effects of orthopaedic insoles in patients with knee osteoarthritis.
Methods: Randomized controlled trials evaluating the effects of orthopaedic insoles on patients with knee osteoarthritis, published up to 16 February 2021, were reviewed and outcomes quantitatively summarized.
Results: A total of 15 studies from 13 randomized controlled trials that involved 1,086 participants were included in this study. All the included studies exhibited a moderate bias risk and were of acceptable quality. The pooled mean difference of pain determined by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was –1.21 (p < 0.001, 95% confidence interval (95% CI) –2.61–0.18) with a high heterogeneity (I2 = 75%). In the sensitivity analysis, the overall incidence was –0.20 (p= 0.62, 95% CI= –0.87–0.46) with an accepted heterogeneity (I2 = 0%). No difference was observed between the Asian and Caucasian groups (p= 0.28). No significant difference was found in the pain score, Lequesne index or functional improvements.
Conclusion: Meta-analysis revealed that orthopaedic insoles do not provide relief of pain or improve functionality in patients with knee osteoarthritis.
Key words: osteoarthritis; knee; knee joint; systematic review; meta-analysis.
Accepted Mar 23, 2021; Epub ahead of print Apr 27, 2021
J Rehabil Med 2021; 53: jrm00191
Correspondence address: Ying Zhang, Department of Rehabilitation, Shanghai Xuhui Central Hospital, Zhongshan-Xuhui Hospital, Fudan University, No. 966 Middle Huaihai Road, Xuhui District, Shanghai 200031, China. E-mail: ZhangYing032317@163.com
Doi: 10.2340/16501977-2836
Osteoarthritis of the knee joint is a progressive degenerative disease, which is fairly common in older adults, and leads to major pain and disability. The development and progression of knee osteoarthritis is exacerbated by excessive load on the medial knee joint. Various forms of orthopaedic insoles, such as insoles that provide arch support, shock-absorbing insoles, and lateral-wedge insoles, are widely used by patients with knee osteoarthritis, and are claimed to provide comfort and better support during walking. However, this meta-analysis and systematic review of randomized controlled trials evaluating the effects of orthopaedic insoles on knee osteoarthritis patients found that orthopaedic insoles do not provide relief of pain or improve functionality in patients with knee osteoarthritis.
Osteoarthritis (OA) of the knee joint is a chronic degenerative disease, which is progressive and disabling, and is fairly common in older adults. OA of the knee produces major pain and disability is a continuous burden for patients (1, 2). As no cure exists, the aims of clinical management are to minimize pain, improve knee functioning and, crucially, enhance the quality of life of patients. Therefore, conservative non-surgical strategies are normally the first choice for clinical management of knee OA (3).
The development and progression of OA of the knee is exacerbated by an excessive load on the medial knee joint (4). Therefore, reducing this load is a vital management strategy for patients with knee OA. During the stance phase of walking, the knee varus moment has been measured to assess the effects of therapy (5). Non-surgical interventions, including valgus bracing, can effectively improve clinical results and reduce the knee adduction moment (6, 7). These treatments, however, are cumbersome and expensive, and may not be appropriate for long-term therapy. In recent years, footwear modifications have been considered as an extensive palliative treatment for patients with knee OA. Orthopaedic insoles are designed to limit medial knee compartment load and effectively to reduce knee varus moment in patients with OA. Various other forms of orthopaedic insoles, such as insoles that provide arch support, shock-absorbing insoles and lateral-wedge insoles, are widely used by patients with knee OA, and are claimed to provide comfort and better support during walking. In recent years, clinical evidence has shown that orthopaedic insoles, especially lateral-wedge insoles, can significantly benefit patients with knee OA (8, 9).
A previous meta-analysis (10) reported that knee pain was not attenuated by lateral-wedge insoles and did not facilitate improvements in knee functioning in patients with OA compared with healthy control subjects. However, limited by few included studies, the previous study could not perform more stratified analyses and draw strong conclusions. Several recent randomized controlled trials (RCTs) (11, 12) have focused on this topic and provided new evidence. The current meta-analysis and systematic review investigated the potential benefits of orthopaedic insoles in subjects with knee OA.
Literature search
An extensive literature search was performed in the following electronic databases: Embase, MEDLINE, PubMed, Cochrane Library and the Chinese BioMedical Literature (CBM) database, to identify relevant articles published up to 16 February 2021. Bibliographies of the retrieved articles were searched, and potentially missed files were interrogated using Google Scholar. The selection of potential studies was carried out following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (13). Various combinations of search terms were used, including: “knee osteoarthritis”, “orthopedic insole”, “orthopedic insoles” and “wedged insoles” to find relevant articles (peer-reviewed papers or reviews).
Criteria for inclusion and exclusion of studies
Studies were included as follows: (i) RCTs that assessed the effect of orthopaedic insoles on patients with knee OA; (ii) patients had been diagnosed with medial compartment knee OA after X-ray imaging; (iii) necessary data was available or could be calculated from the published articles; (iv) articles were published in English or Chinese; (v) if authors published multiple papers using overlapping sample data, only the most inclusive publication or the last-published paper was included in the analysis.
Case reports, letters, review articles, studies conducted in animal models, studies focused on experiments in vitro, and studies in languages other than English or Chinese were excluded.
Data extraction
Two authors (LY and YW) independently reviewed all retrieved articles and reached a consensus on all relevant items. For each article, a standardized form was used to extract the relevant information, including: authors; year of publication; type of study; population characteristics (e.g. age, sex, nationality); intervention/therapy characteristics; and outcome assessments.
Assessment of risk of bias
Each study was assessed for its risk of bias according to the 7-category Cochrane bias tool (14). The results were graded into: unclear, low- or high-risk categories of bias, based on the following criteria: (i) sequence generation; (ii) concealment of allocation; (iii) personnel blinding to study data; (iv) outcome assessor blinding; (v) outcome data not complete; (vi) outcome reporting that was selective; and (vii) other factors that could have led to bias. For each included article, every analysed factor was judged to be uncertain if the author(s) did not provide either sufficient information or if there was no reported assessment of risk of bias for a particular variable.
Assessment of study quality
Jadad scoring (15) was employed to establish the quality of each article. The process was independently performed and cross-checked by the 2 authors (LY and YW). Each included study was scored 0–5 by the performance of 3 key methodological items, namely randomization, blinding and accountability of all patients. One or 2 points were accumulated for the answer “yes” to each of the randomization and blinding items. Another point was accumulated for the answer “yes” to the item of accountability for all patients. To set a minimum standard for inclusion of a paper’s results, a Jadad score < 3 points was used as the cut-off value for excluding targeted papers (16).
Statistical analysis
An inverse variance method with a random-effect model was used to collect dichotomous outcomes. For continuous variables, mean differences (MDs) and 95% confidence intervals (95% CIs) were extracted and pooled. Meta-analysis was undertaken when 2 or more articles reported the same factor or outcome in a comparable manner.
The I2-squared statistic was used to quantify heterogeneity and to assess the reliability of effect values. This statistical value indicated the variability percentage in the effects estimate. If I2 values were 25%, 50% or 75%, heterogeneity was deemed to be low, moderate or high, respectively (17). When I2 was > 50%, to explore sources of heterogeneity, each study was sequentially excluded one by one to determine its overall impact. Potential bias in a publication was further assessed using Begg’s correlation (18) and Egger regression (19) methodology. Stratified analyses were subsequently performed according to the research study population characteristics and outcomes. Review Manage (version 5.3, The Cochrane Collaboration, Oxford, UK) was used for the generation of forest plots and statistical analyses. Begg’s and Egger’s analyses were evaluated using STATA ver. 15.0 software (Stata Corporation, College Station, Texas, USA). p-values < 0.05 were deemed significant for all data analysed.
Selection of studies
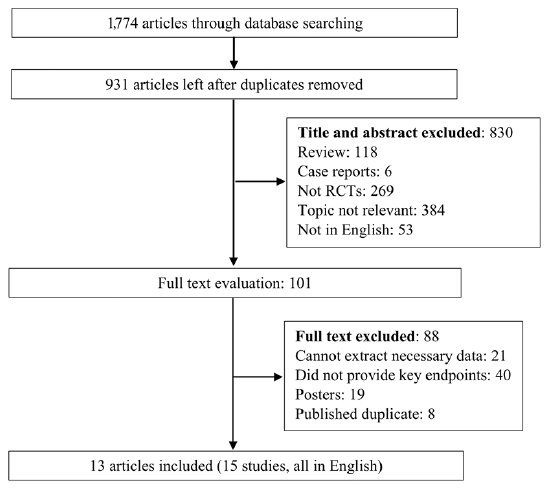
The search strategy originally identified 1,774 citations, and 931 studies remained after had been removed duplicates. Of these, 830 were excluded after title or abstract screening. Finally, 15 studies from 13 RCTs (11, 12, 20–30) were eligible for data extraction and meta-analysis after retrieving 101 full-length manuscripts. A schematic illustration of the selection criteria for the included studies is shown in Fig. 1.
Fig. 1. Schematic illustration of study selection criteria. RCT: randomized controlled trials.
Study characteristics
A total of 15 studies involving 1,086 participants were included. The characteristic features of the studies and individuals involved are summarized in Table I. The sample sizes of the included studies were between 30 and 200 participants, published between 2004 and 2016. The mean age of subjects was > 60 years except for one study (28); the majority of studies included more females than males. Two RCTs were performed in Chinese Taipei (12, 25), 2 in Japan (30, 31), 3 in USA (20, 21, 24), 2 in Brazil (23, 27), and 1 in each of Australia (22), Iran (28), France (26), and Canada (11). Most studies investigated differences between the effects of lateral wedge and flat control insoles, and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) were documented in 11 studies. Other indices were pain scores, the Lequesne index (31), the femorotibial angle and functional improvements.
Risk of bias and quality assessment of studies
Most of the included studies exhibited a moderate risk of bias, but were of acceptable quality. The overall risk of bias and quality of the studies are shown in Fig. 2 and Table SI. Five studies were evaluated as full scores and the other studies were assessed as 3, as some did not conduct a blind method according to the Jadad scale.
Table I. Study participants’ characteristics of the included studies
Fig. 2. Overall bias risk and quality of the included studies.
Pain assessment
Five studies reported pain scales, including the visual analogue scale for pain (VAS), the Knee injury and Osteoarthritis Outcome Score (KOOS), WOMAC OA index, and WOMAC pain index. The pooled MD for pain scores was –1.25 (p = 0.24, 95% CI –3.34–0.85) with a moderate heterogeneity (I2 = 59%). When one study was removed from the model (22), the heterogeneity disappeared with a pooled MD of –2.34 (p = 0.63, 95% CI –3.97–0.72). The results are shown in Fig. 3 and Fig. S1.
Of the 15 studies, 9 provided data about WOMAC pain. The 9 studies included 410 subjects in the experimental and 393 in the control group, respectively. There was a moderate heterogeneity across studies, with I2 = 75%. The MD of the 2 groups in each study ranged from –11.79 to 2.80, and according to the pooled result, the control group was observed to have a stronger WOMAC pain score than the experimental group, with a MD of –1.21 (p < 0.001, 95% CI –2.61–0.18). More data are shown in Fig. 4A.
Fig. 3. Summarized pain score of the included studies (5 studies). SD; standard deviation; 95% CI: 95% confidence interval; IV: inverse variance method.
Fig. 4. Heterogeneity data of the included studies. (A) Summarized Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain index of the included studies (9 studies); (B) Summarized WOMAC stiffness index of the included studies; (C) Summarized WOMAC function index of the included studies. 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance method.
A sensitivity analysis was carried out to investigate possible sources of heterogeneity, by categorizing studies into 2 groups according to the ethnicity of participants. The Asian group included 3 studies from Chinese Taipei and Japan, and the Caucasian group included 6 studies from the USA, France, Brazil, Australia and Iran. The overall MDs in the Asian group (–5.31, 95% CI –13.76–3.13) and Caucasian group (–0.64, 95% CI –1.58–0.29) were similar (p = 0.09), and the heterogeneities for the 2 groups were I2 = 85% and I2 = 55%, respectively. After further excluding one study from the Asian group (25) and the Caucasian group (28), the overall incidence was –0.20 (p = 0.62, 95% CI –0.87–0.46) without heterogeneity (I2 = 0%). Further data are shown in Fig. 4A and Fig. S2.
WOMAC stiffness and WOMAC function indexes
The pooled WOMAC stiffness index and WOMAC function index are shown in Figs 4B and 4C, respectively. The pooled mean different of the 2 indexes were 0.01 (p = 0.64, 95% CI –0.54–0.56) and 0.34 (p = 0.60, 95% CI –2.66–3.34) with heterogeneity of I2 = 0%, respectively.
Lequesne index
Five studies provided the results on Lequesne index and the pooled MD was –1.29 (p=0.02, 95% CI –3.43–0.85) with a moderate heterogeneity (I2 = 66%). After removal of one study (30) from the model, the heterogeneity decreased to I2 = 34%, with a pooled MD of –0.41 (p = 0.21, 95% CI –2.14–1.32). The results are shown in Fig. 5A and Fig. S3.
Fig. 5. Heterogeneity data of the included studies. (A) Summarized Lequesne index of the included studies (5 studies); (B) Summarized femorotibial angle of the included studies; (C) Summarized functional improvements of the included studies (6 studies). 95% CI: 95% confidence interval; SD: standard deviation; IV: inverse variance method.
Femorotibial angle
The result of the femorotibial angle are shown in Fig. 5B and the pooled MD was –1.49 (p = 0.39, 95% CI –2.63 to –0.36) without heterogeneity (I2 = 0%).
Functional improvements
Six studies provided data on improvements in functioning. The results are summarized in Fig. 5C. The pooled result was –1.32 (p < 0.01, 95% CI –6.99–4.35) with a higher heterogeneity (I2 = 86%). After removing 2 studies (25, 28) from the analysis, the pooled result was –0.26 (p = 0.74, 95% CI –2.92–2.40) without heterogeneity (I2 = 0%) (Fig. S4).
Publication bias
After Begg’s and Egger’s analyses, potential publication bias was detected (each p-value of the analysis was > 0.05). The detailed potential publication biases for each analysis are shown in Table SII.
The current meta-analysis explored the effects of orthopaedic insoles in patients with knee OA. A total of 15 studies from 13 RCTs involving 1,086 participants were included and the data summarized. The pooled MD of WOMAC pain was –1.21 (p < 0.001, 95% CI –2.61–0.18) with a higher heterogeneity (I2 = 75%). In the sensitivity analysis, the overall incidence was –0.20 (p = 0.62, 95% CI = –0.87–0.46) without heterogeneity (I2 = 0%). No significant difference was found between the Asian and Caucasian groups in the pain scale, Lequesne index or functional improvement.
The most recent previous meta-analyses (10) that focused on the topic of the current review concluded that there was virtually no credible evidence that lateral wedge insoles reduce the knee varus angle. Furthermore, in 8 RCTs, lateral wedges were shown to be no more effective than neutral inserts in improving pain and functionality in individuals with knee OA. Although the current study included more RCTs and larger sample sizes, the results were similar to previously published data. Orthopaedic insoles, especially lateral-wedge insoles, are one of the most commonly used methods for non-surgical treatment of patients with knee OA. A number of previous studies have reported that orthopaedic insoles, especially lateral-wedge insoles, can improve physical functionality in patients with knee OA by increasing the walking speed and reducing pain levels (32, 33). However, when the current study systematically assessed their effects on pain and functionality, the data did not show that orthopaedic insoles benefited patients with knee OA. The type, quality, and even the raw materials, from which the orthopaedic insoles were fabricated may have influenced the results.
Previous studies have suggested that a younger age (34) and lower body mass index (BMI) (20) might contribute to the degree of knee OA. However, the mean age of the participants in the studies was > 60 years, except for one study, and the BMIs were all significantly higher than in the general population. Moreover, none of the included studies undertook subgroup analysis of the BMIs of participants. This could be another reason that no effect was found. In the current study of Asian and Caucasian groups, no differences were found in pain assessment scores. To date, no convincing evidence has demonstrated a causal relationship between race and the role of orthopaedic insoles in pain management. However, different body forms and daily living habits might be reasons for the variations in the conclusions drawn. Further research is needed, stratified according to the subjects’ daily living habits and other factors, which may affect the control of balance.
The current meta-analysis has various limitations. First, the majority of studies had low patient numbers. Therefore, due to the limited sample size of the studies, there were not enough participants to perform more subgroup or sensitivity analyses. Secondly, most of the studies did not match the participants according to age and sex. Therefore, the sex ratio of each RCT was highly variable, and might have cause heterogeneity and reduced the stability of the results. Moreover, most of the RCTs did not report the duration of the knee OA condition or its severity, which may also cause heterogeneity of the results. Thirdly, the assessment of outcomes was relatively heterogeneous. More than 7 scores or methods were employed to assess outcomes. Therefore, only a limited number of studies could be included in the combination of outcomes. Fourthly, the majority of the studies did not stratify the participants by daily wearing time, which might also cause heterogeneity among the studies. Fifthly, the current meta-analysis is based on published studies and all the analyses were conducted according the published results. The innovation might be insufficient. However, the results might provide suggestions for clinical management of knee OA. Sixthly, potential bias may have been introduced to the current analysis because only research articles published in the English or Chinese languages were analysed.
This meta-analysis systematically assessed the effects of orthopaedic insoles in people with knee OA. Regarding pain assessment, 2 scores were employed; WOMAC pain and a pain scale. No differences were found between the Asian and Caucasian groups after sensitivity analysis of the WOMAC pain and the standard pain scale. The current review found no significance differences in the Lequesne index or functional improvements. To detect potentially important differences, larger sized RCTs, and RCTs that match age, sex and the severity of knee OA, are necessary to address these issues.
Funding. This work was supported by the Medical Scientific Project of Xuhui District (grant number SHXH201901). The funder had no role in the study design, data collection or analysis, the decision to publish or drafting of the manuscript.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize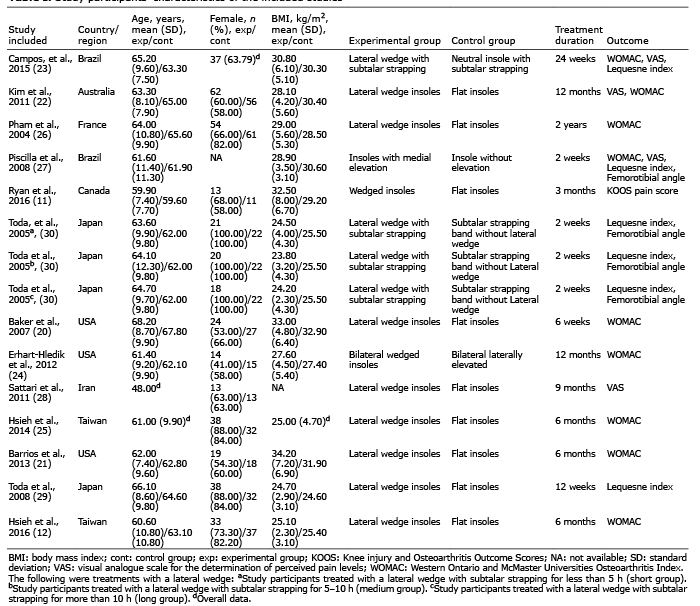 Click to show fullsize
Click to show fullsize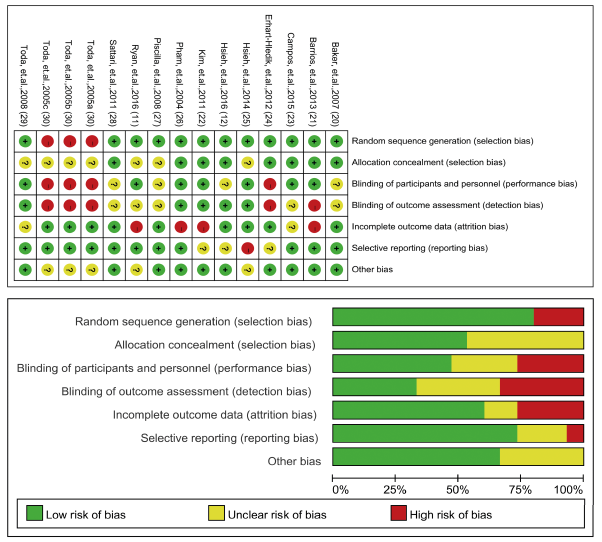 Click to show fullsize
Click to show fullsize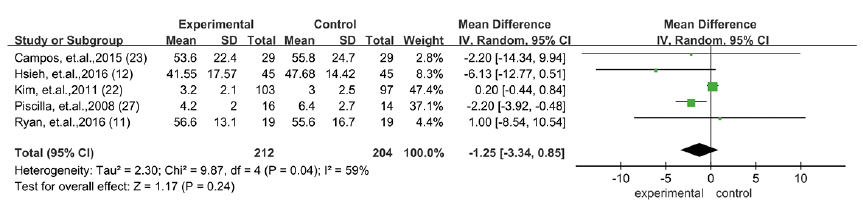 Click to show fullsize
Click to show fullsize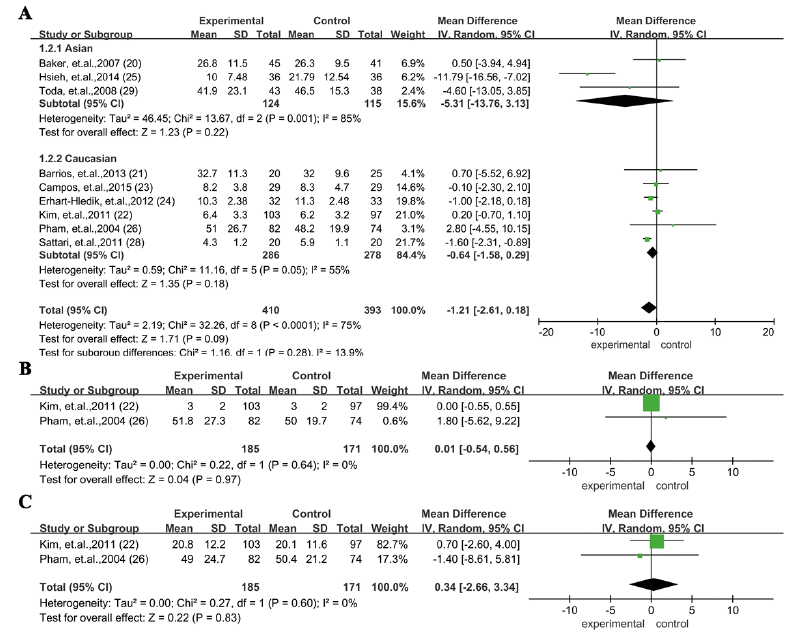 Click to show fullsize
Click to show fullsize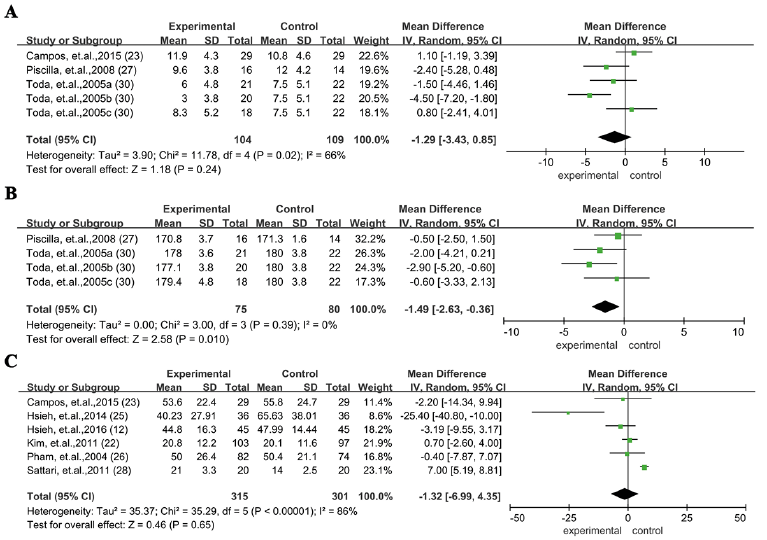 Click to show fullsize
Click to show fullsize