
From the 1Centre for Physiotherapy and Rehabilitation Sciences, Jamia Millia Islamia, Delhi, 2Actio Prehab, Indrapuram, UP, India and 3Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
Objective: Athletes with chronic ankle instability tend to develop hip abductor muscle weakness. Kinesio taping may help this muscle perform its functions, thus preventing injury. The aim of this study was to assess the effects of Kinesio taping on hip abductor muscle strength and electromyography (EMG) activity.
Subjects: A total of 34 athletes, mean age 22.08 years (standard deviation 2.71 years) participated in the study.
Methods: A pre-test–post-test experimental design was used. For the experimental group, Kinesio tape, and for the control group, Micropore tape, was applied over the gluteus medius muscle. Gluteus medius muscle strength and EMG activity were noted in supine and during the single-leg squat test (SLST), respectively, before and after the intervention. Strength was measured through maximum voluntary isometric contraction (MVIC) force with a handheld dynamometer, and muscle activation measured through EMG.
Results: In the experimental group, there was a significant increase in gluteus medius strength, by 10.27% (p = 0.00), and a significant decrease in EMG activity (p = 0.00), by 8.38%. In the control group, there was a significant increase in gluteus medius strength, by 2.89% (p = 0.01) and a not statistically significant decrease in EMG activity, by 0.80% (p = 0.15).
Conclusion: Kinesio taping is effective in increasing hip abductor muscle strength in athletes with chronic ankle instability.
Key words: ankle injury; hip abductors; Kinesio taping; muscle strength, electromyography.
Accepted May 10, 2021; Epub ahead of print May 20, 2021
J Rehabil Med 2021; 53: jrm00204
Correspondence address: Masood Khan, Building 24, G095-1, Rehabilitation Research Chair, College of Applied Medical Sciences, King Saud University, PO Box, 10219, Riyadh-11433, Saudi Arabia. E-mail: masoodkhan31@rediffmail.com; mkhan4.c@ksu.edu.sa
Doi: 10.2340/16501977-2845
Athletes with chronic ankle instability tend to develop hip abductor weakness, which further predisposes them to injuries in the lower limb and hinders their athletic performance. Kinesio taping may help this muscle perform its functions. The aim of this study was to determine the effects of Kinesio taping, applied over the hip abductors, on muscle strength and activation. A total of 34 athletes with chronic ankle instability were recruited to the study. Kinesio taping was found to be effective in increasing the strength of the hip abductor muscle and reducing its activation. Kinesio taping can be used by athletes with chronic ankle instability to prevent injury to the lower limb, for rehabilitation, and to enhance their athletic performance.
One of the most common injuries, occurring not only in sports, but also in everyday activities, is ankle sprain (1, 2). Incomplete recovery of ankle sprain is very common, and the majority of individuals after initial ankle sprains experience residual symptoms, such as repeated sprains, pain, and a sensation of “giving way” (3). This condition is called chronic ankle instability (CAI) (4). CAI is highly prevalent in high-school/ collegiate athletes, and occurs in up to 70% of athletes with initial ankle sprains (5–8). CAI is associated with reduced health-related quality of life, reduced physical activity levels, and suboptimal functional levels (9). In individuals with chronic ankle sprains the ipsilateral hip abductor muscles are weak in comparison with the uninjured side (10, 11). Beckman & Buchanan observed a significant delay in muscle activation of the gluteus medius (GM) in individuals with CAI (12).
Weak hip musculature and comparatively stronger hip adductors further predispose the ankle joint to sprains, because hip joint stability and hip musculature strength are crucial for foot positioning during the heel strike phase of the gait cycle and overall proper gait mechanics (11, 13). This becomes a vicious cycle, in which CAI causes hip abductor muscle weakness and weak hip abductor muscles cause ankle injuries. Therefore, to prevent future problems in the foot and ankle complex in such individuals, this vicious cycle should be broken, either through strengthening the weak hip abductors or by reinforcing the actions of these muscles. Application of Kinesio tape (KT) (3B Scientific®tape, Burnham-on-Sea, UK) is also a method for improving muscle functions, and thus can be used to reinforce the actions of hip abductors. KT is a thin elastic tape that has stretchability up to 120–140% of its original length, and hence provides less mechanical constraint during movement. KT is considered to prevent injuries during sports and to reduce muscle spasms, swelling, and pain (14).
A recent study has examined the effects of KT on hip abductor muscle strength in athletes with and without functional ankle instability (FAI) and reported an increase in muscle strength after application of KT (15). However, in that study, KT was applied over both the peroneus longus and the GM, not over the GM only. To the best of our knowledge, no study has examined the effects of KT on muscle strength and electromyography (EMG) activity of GM when KT is applied over the GM only.
The aim of this study was to examine the effects of KT on muscle strength and EMG activity of GM in athletes with CAI. If KT is found to have significant effects on muscle strength and EMG activity then it can be used to improve lower limb kinematics, improve athletic performance, prevent and treat lower limb injuries. It has been hypothesized that muscle strength would increase and EMG activity of GM decrease after the application of KT over GM in athletes with CAI.
Study design
The study has a 2-arm comparative pre-test–post-test experimental research design, with random allocation of subjects into groups (experimental and control), using the lottery method and the website randomization.com. A total of 34 chits, numbered 1–34, were placed in a box. For each participant included in the study the examiner picked a chit from the box and that number was allocated to that participant. Random permutation of integers from 1 to 34 was generated for 2 groups using the website randomization.com and participants were allocated into the experimental or control group accordingly.
The study conformed to “The Code of Ethics of the World Medical Association (Declaration of Helsinki)”. Approval was obtained from the ethics committee of the institutional review board (file id: RRC-2019-27). The study was conducted in the research laboratory of the university (Centre for Physiotherapy and Rehabilitation Sciences, Jamia Millia Islamia, Delhi, India) and registered in clinicaltrial.gov (ID: NCT04728672).
Participants
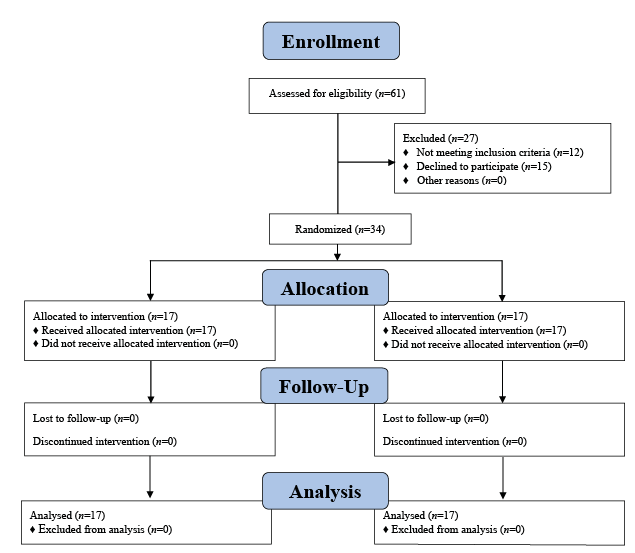
Before conducting the study, the sample size was calculated using G*Power Software1 using data regarding changes in strength from a similar study by Lee et al. (16), and 17 participants per group (including 12% dropout) were shown to be necessary, based on an effect size of 0.86, an alpha level of 0.05 and power (1 – beta) of 0.80. Therefore, a total of 34 collegiate male athletes (mean age 22.08 years, standard deviation (SD) 2.71) were selected for the study (Fig. 1 and Table I). Inclusion criteria for selected athletes were: repeated episodes of giving way after an initial ankle sprain; a history of at least 2 ankle sprains to the same side without injury to the contralateral ankle in the last 2 years; and no history of other trauma to the lower extremities for the past 3 months before the study. Participants also needed to be capable of full weight-bearing without pain and subjectively reported that functional use of ankle had plateaued since the last injury. Exclusion criteria were: participants with a history of ankle fracture, knee ligament injury, back or lower limb surgery or neuromuscular disease; current neurological deficits; or receiving ankle rehabilitation.
1G*Power has been developed by these people: Dr. Franz Faul, Department of Psychology, Christian-Albrechts-University, Olshausenstr. 62, 24098 Kiel, Germany. Dr. Edgar Erdfelder, Professor of Psychology, Department of Psychology, Mannheim University, Schloss, Ehrenhof-Ost68131 MannheimGermanyDipl.-Psych. SAE-Diplom Audio Engineer Albert-Georg Lang, Department of Experimental Psychology, Heinrich-Heine-University, 40225 Dsseldorf, Germany. Dr. Axel Buchner, Professor of Psychology, Department of Experimental Psychology, Heinrich-Heine-University, 40225 Dsseldorf, Germany.
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) flowchart of the study showing recruitment of participants.
Table I. Respondent’s demographic and variables data, n=17 in each group, p-values for Shapiro–Wilk tests of normality
According to the inclusion and exclusion criteria of the study, participants were selected and randomly allocated into either of the 2 groups using the website Randomization.com (http://www.randomization.com) by an expert physiotherapist with 17 participants in each group: experimental group and control group. The participants were unaware of the random sequence. The outcome assessor was also kept blinded to the allocation. In the experimental group, KT was applied over GM of the involved lower extremity; however, in the control group placebo Micropore tape (MT) (3M India Ltd, Gurugram, Haryana, India) was applied. Before the application of any intervention, the risks and benefits of the study were discussed with participants, and informed consent was obtained.
Instrumentation
Protocol
This study consisted of 3 phases: pre-intervention evaluation; intervention; and post-intervention evaluation.
Pre-intervention evaluation.
Intervention. KT and MT were applied over the GM region in the experimental and control group, respectively.
Post-intervention evaluation. Immediately after the application of KT and MT in the experimental and control groups, respectively, MVIC force and EMG activity were measured similarly, as for pre-intervention evaluation.
Data analysis
Data were analysed using SPSS statistical software version 26 (SPSS Inc., Chicago, IL, USA). The normal distribution of baseline data of variables (ipsilateral hip abductors MVIC force, and electromyography root mean square value (EMGrms) values) was assessed using the Shapiro–Wilk test of normality. The difference between ipsilateral and contralateral hip abductors’ strength was compared using paired samples test in both groups. For within-group analyses of dependent variables (pre-intervention and post-intervention comparison) paired samples test and for between-group analyses, independent samples test was performed. Results were considered significant for p < 0.05.
Fig. 2. Application of Kinesio tape over gluteus medius muscle.
Shapiro–Wilk test of normality revealed normal distribution for both variables data (df = 17, p > 0.05) (Table I). The paired samples test revealed a significant difference between contralateral and ipsilateral hip abductor muscle strength in both groups (control group, df = 16, p = 0.012; experimental group, df = 16, p = 0.010), which meant that the affected limb was weaker than the normal limb in both groups (Table II). Independent samples test, performed to compare demographic and pre-intervention variables data, revealed no significant difference between the groups, which meant that both groups were comparable in terms of age, height, weight, body mass index (BMI), number of sprains, ipsilateral hip abductor strength, and EMGrms values (Fig. 3).
Table II. Comparison between ipsilateral and contralateral hip abductors strength
Fig. 3. Graph depicting the change in maximum voluntary isometric contraction (MVIC) force and electromyography (EMG) mean values in both groups.
Within-group analysis (paired samples test)
Experimental group. There was a significant increase in hip abductor MVIC force, by 10.27% (df=16, p = 0.000, Cohen’s d = 2.642) and a significant reduction in EMG activity, by 8.39% (df=16, p = 0.000, Cohen’s d = 1.322) after the application of KT (Table III).
Control group. There was a significant increase in hip abductor MVIC force, by 2.90% (df = 16, p = 0.019, Cohen’s d = 0.634) and a reduction in EMG activity, by 0.8%; however, this reduction was not statistically significant (df = 16, p = 0.155, Cohen’s d = 0.362), after application of MT (Table III).
Between-group analysis (independent samples test)
There was a significant difference between the groups for changes in MVIC force (F = 0.481, t = –4.989, df = 32, p = 0.000, Cohen’s d = 1.711) and EMGrms values (F = 14.265, t = 4.673, df = 32, p = 0.000, Cohen’s d = 1.602) before and after the intervention (Table IV).
Table III. Maximum voluntary isometric contraction (MVIC) force and electromyography root mean square value (EMGrms). p-values for the paired samples test
Table IV. Independent samples test p-values for between-group comparison of dependent variables
This study aimed to examine the effects of KT on muscle strength and EMG activity of GM muscle. The results show that GM muscle strength increased and EMG activity decreased after application of KT over GM muscle in athletes with CAI. Placebo MT application also increased the muscle strength of GM; however, this increment was less in comparison with KT. However, placebo MT did not result in any change in the EMG activity of GM muscle. To the best of our knowledge, no study has examined the effects of KT on muscle strength and EMG activity of GM when KT was applied over the GM only. Therefore, comparison of this study with other studies is difficult, and thus a sufficient review of literature is unavailable to support these findings. However, one recent study examining the effects of KT on hip abductor muscle strength in athletes with and without functional ankle instability (FAI) reported an increase in muscle strength after application of KT (15). However, in that study, KT was applied over both peroneus longus and GM muscles, not over GM only. Another study, by Elshemy et al., reported improvement in eversion to inversion concentric strength ratios in children with functional ankle instability after application of KT over the ankle (23).
Several mechanisms have been suggested for the beneficial effects of KT on muscle strength. First, the tactile stimulation of KT affects muscle activation levels. Konishi reported that this tactile stimulation alleviates muscle weakness (24). The ability to enhance muscle activity was attributed to Ia afferents. Afferent feedback from mechanoreceptors via sensory stimulation is sent to gamma motor neurones, which are important for Ia afferent modulation. Therefore, increasing inputs to gamma motor neurones can reverse muscle weakness (24). Secondly, it is hypothesized that, depending upon the way tape is applied over the muscle belly, it inhibits or facilitates muscle function. The tape draws the origin of muscle towards its insertion when it is applied under tension in the direction of muscle fibres. It is proposed that, due to this shortening of a lengthened muscle, the length-tension relationship of the muscle is optimized, and thus the force-generating capacity is increased (25). However, muscle function is thought to be inhibited when the tape is applied across the muscle belly (26).
Lastly, the applied direction of KT also influences muscle tone. There are 2 ways to apply KT in the direction of muscle fibres; from muscle origin to its insertion and muscle insertion to its origin. If KT is applied from origin to insertion then muscle function is facilitated, and contraction is improved, thus muscle strength is increased; however, if KT is applied from insertion to origin then muscle function is inhibited (27, 28). The wrinkles of the skin (convulsions) formed after the application of KT, in combination with the direction of the tape, pull the insertion of the muscle towards the direction of the contraction. This causes a change in shear force, pressure, and stretch load that triggers mechanoreceptors present in subdermal fascia and soft tissues. The central nervous system integrates the sensory input and modulates gamma-motor firing, which, in turn, leads to increased muscle tone (29). KT may also improve self-confidence and sense of stability, leading to better athletic performance (15). Additional benefits of KT application are also reported, such as acceleration of healing process in injured tissues by promoting subcutaneous blood and lymphatic reflux (30).
Another important finding of the present study was that the application of KT on GM muscle significantly reduced its EMG activity during SLST. This decrease in EMG activity of GM muscle may be the result of greater maximal muscle contraction and less neuromuscular recruitment during SLST. A decrease in EMG activity may imply that KT is having a supportive effect and fewer muscle fibres were activated to perform the same task; hence the muscle appears to be working more efficiently. This finding is supported by a few earlier studies. For example, a study by Lee et al. (16) found decreased EMG activities of vastus medialis obliquus (VMO) and vastus lateralis (VL) during stair ascent and descent in patients with patellofemoral pain syndrome (PFPS) after application of KT. Also, Keet et al. (31) applied tape around the knee joint in patients with PFPS and reported a significant reduction in EMG activity of VMO during stair ascent and descent. Further similar findings were reported by Parsons & Gilleard (32), who found a significant reduction in muscle activity of VMO and VL during stair ascent and descent after tape application.
However, some studies do not support the findings of the current study concerning muscle strength, e.g. a study by Cai et al. and Au et al. did not report any significant difference in grip strength and EMG activity between facilitatory KT, inhibitory KT, sham KT, and tapeless conditions (33, 34). Concerning muscle activity, some studies have reported findings contrary to the present study, e.g. Mak et al. and Briem et al. reported no significant difference in muscle activity between KT and tapeless conditions (35, 36). A study by Gomez-Soriano et al. reported a short-term increase in EMG activity of the gastrocnemius medialis after the application of KT (37), which is contrary to the findings of the current study, in which a decrease in EMG activity was observed.
In the current study, KT produced significant changes in muscle strength and EMG activity in comparison with placebo MT. One of the reasons for this difference may be that the thickness and weight of the KT are similar to that of human skin (38). Also, the elastic property of KT allows better shortening of the muscle and unrestricted range of motion, thus it offers less mechanical constraint compared with MT. KT also has lifting effects that enhance muscle tone. These properties of KT together may have contributed to better results compared with MT.
This study has clinical relevance for individuals with CAI. The function of KT to facilitate GM muscle can be used in sports rehabilitation to improve athletic performance, prevent injuries, and improve lower limb kinematics. Thus, KT can be useful in providing therapeutic and prophylactic assistance to weak hip abductor muscles in subjects with CAI.
This study also has scope for future research. It is unknown whether the improved functions of GM muscle will stay for a long time; thus further research is needed to investigate the long-term effects of KT. It may be inappropriate to extrapolate the activation of one subdivision of GM muscle to the whole muscle, owing to the functional subdivisions within each muscle. Activation levels in all 3 GM subdivisions may differ in amplitude and duration during functional tasks. Further research is needed to investigate the muscle activity levels in all 3 GM subdivisions during functional tasks.
The current study has some limitations. First, the study includes the use of subjective self-reports of instability only; however, objective functional assessment tools/scores should also be included in inclusion criteria along with activity profile (e.g. current activity/sports level) and the nature of the previous or current treatment taken. This would enable better understanding of the correlation of results with the physical activities of participants. Another limitation of this study was the use of surface electrodes rather than fine-wire electrodes. In the current study, there may be contamination of the signals by the gluteus maximus muscle. As the sample included only male collegiate athletes with CAI, the generalizability of the current findings to other populations, such as female athletes and sports professionals, is inappropriate. Also, females have greater ligamentous laxity and are more prone to ligamentous injury; therefore the efficacy of the KT on female athletes may be more advantageous. In conclusion, application of KT is effective in increasing muscle strength and reducing the EMG activity of GM muscle in athletes with CAI with ipsilateral hip abductor weakness. Thus, the application of KT can be used as an effective tool in combating hip abductor weakness. KT can be used to prevent injuries, for rehabilitation, as well as enhancing athletes’ performance.
The authors are grateful to the Deanship of Scientific Research, King Saud University for funding through Vice Deanship of Scientific Research Chairs.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize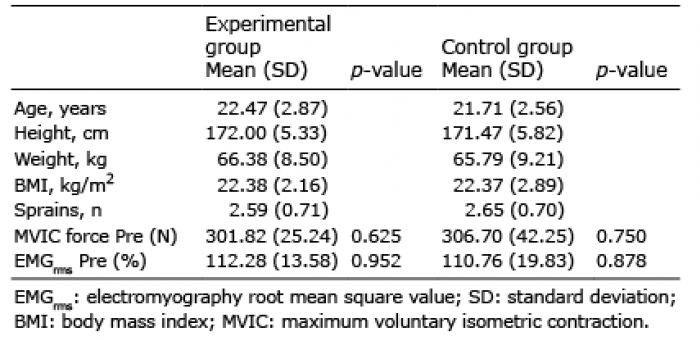 Click to show fullsize
Click to show fullsize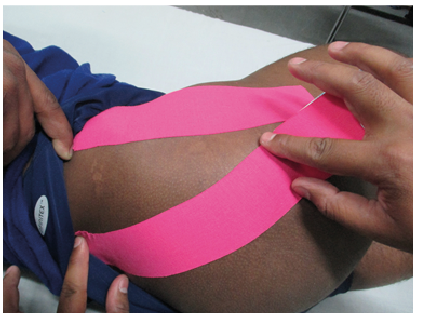 Click to show fullsize
Click to show fullsize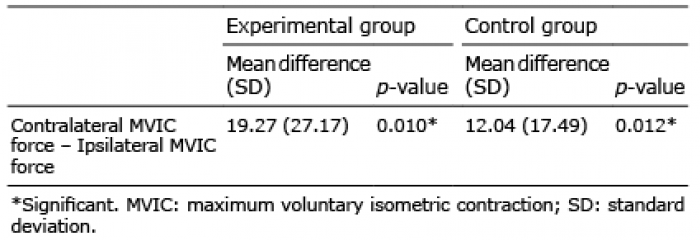 Click to show fullsize
Click to show fullsize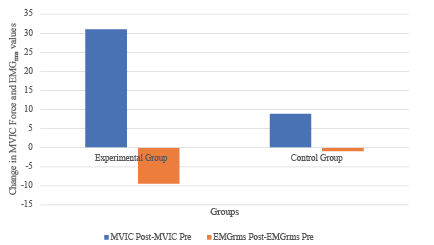 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize