
1Rehabilitation and Physical Medicine, Medical University of Łódź Chair of Nephrology and Hypertension, Łódź, Poland
2Medical Magnus Clinic in Łódź, Medical Magnus Clinic in Łódź, Łódź, Poland
Osteoarthritis is a group of multiple overlapping pathological conditions that cause destruction of articular cartilage and other structures of the joint. It is a progressive disease that leads to limitations of physical activity. New forms of treatment are therefore sought to alleviate the clinical symptoms of osteoarthritis and avoid surgery. Stem cell based therapy is an emerging field in orthopaedics. This study describes the treatment of knee osteoarthritis with CD34+ stem cells at the Medical Magnus Outpatient Clinic in Lodz, Poland, together with the treatment and rehabilitation algorithm developed for maximum effectiveness of this procedure. The algorithm includes 3 rehabilitation stages: preoperative, hospitalization and outpatient periods.
Key words: osteoarthritis; stem cell; knee joint.
Accepted Nov 14, 2018; Published Dec 19, 2018
JRM-CC 2018; 1: 1000012
Correspondence address: Paulina Klimkiewicz, Rehabilitation and Physical Medicine, Medical University of Łódź, 90-647 Lodz, Poland. E-mail: anna.kubsik@wp.pl
Osteoarthritis of the knee joint is a chronic disease that mainly affects people over 50 years of age. The main symptoms include pain and limitation of range of motion of the joint, which prevent patients from participating in physical activity. Stem cell therapy has been developed in orthopaedics in recent years for the treatment of gonarthrosis. Rehabilitation is necessary after stem cell transplantation in patients with gonarthrosis in order to restore the proper range of joint mobility, for anti-oedematous action, muscle strength improvement, and for elimination of pain. This article describes the physiotherapy algorithm used for patients
after stem cell transplantation. Kinesitherapy and physical
therapy enabled a more rapid return of the patient to physical or professional activity.
O
steoarthritis (OA) is a group of multiple overlapping pathological conditions that lead to the destruction of articular cartilage. OA is one of the most common diseases of the musculoskeletal system and is termed a civilization disease of the 21st century. The years 2000–2010 were designated by the World Health Organization (WHO) and the United Nations Organization (UNO) as the bone and joint decade. The clinical manifestations of OA include joint pain, locomotor restriction, pain on palpation, joint crepitation, exudates, and inflammation without systemic symptoms. OA is a chronic disease with periods of exacerbation and remission. The above definition of OA was set out by experts of the American Academy of Orthopedic Surgeons; National Institute on Aging; National Institute of Arthritis and Musculoskeletal and Skin Diseases (1).
Gonarthrosis (GA) is the most frequent form of osteoarthritis. Three forms of the disease are distinguished according to the location of degenerative changes:
Based on the aetiopathogenesis of the disease, primary (idiopathic) and secondary forms are distinguished. Genetic factors, hormonal changes (menopause), nutritional neglect (a diet lacking vitamin D, C, E and mineral supplements, excess carbohydrates and trans-fats), previous knee injuries, physical (recreational or professional) activity involving the knee joints or requiring a forced position of the body may contribute to degenerative changes (2, 3). The correct biomechanics of the knee joint protects the joint against excessive strain. With age, cartilage loses the ability to regenerate, resulting in inflammation, pain and limitation of joint mobility. Modifications in the subchondral tissue also occur, in which, in the course of GA, thickening of the subchondral layers and sclerosis (hardening) are observed (4, 5). Age-related chondropaenia (glycation of collagen and deposition of pyrophosphate crystals) leads to an increase in the susceptibility of cartilage to injury. Ageing chondrocytes lose their synthetic ability, resulting in the production of irregular aggrecan molecules (6–8). Excessive loads cause destruction of cartilage tissue, which, over time, leads to apoptosis and changes in the cartilage structure. These changes initiate a local immune response at the site of injury, leading to synovitis and development of degenerative changes (9). Unloading, particularly immobilization, the pathogenic mechanism of which consists mainly of insufficient nutrition of the cartilage, may be an inverse factor in the damage. Deficiency of interleukin 10 (IL-10), secreted during motion, may also contribute to the pathogenesis of degenerative changes in this mechanism (10).
GA is a progressive disease and new treatments or rehabilitation strategies are needed to reduce functional impairment of the joint. Stem cell therapy has been developed for treatment of GA and is an alternative to well-known pharmacotherapy, surgical methods or physiotherapy. Stem cells used for treatment of GA are derived from peripheral blood. These cells are drawn from the patient prior to the procedure and injected at the site of the injury or lesion. CD34+ stem cells are used in the procedure because they demonstrate repair capacity. Furthermore, these cells have the ability to promote apoptosis; thus, if abnormal cells are present the organism itself destroys them, thereby protecting the patient against transformation of the given cell into, for example, a tumour cell. The use of CD34+ stem cells primarily helps to relieve pain, regenerate articular cartilage, and improve joint function, including the range and muscle strength, which improves the quality of life of patients and their return to daily physical activity. CD34 is currently recognized as a marker of many other non-haematopoietic cell types, including vascular endothelial progenitor cells and embryonic fibroblasts. Structurally, CD34 is a transmembrane phosphoglycoprotein, first identified in 1984 (11). In general, CD34 is commonly used as a marker of human and mouse myocardial cells. The properties of CD34+ endothelial cells are often associated with haematopoietic cells, because both types of cell can be isolated from peripheral blood using CD34 as an antigen (12, 13).
Full therapeutic efficacy is achieved with the contribution of physiotherapy, which includes preoperative, early and late inpatient hospital care, and outpatient periods. Selected physiotherapy procedures are applied in particular treatment processes, as determined by the Medical Magnus Clinic, Łódź, according to the algorithm of treatment and rehabilitation for knee osteoarthritis with the use of CD34+ stem cells (Tables I–III). This algorithm was developed on the basis of many years’ experience in physiotherapy. Approximately 500 patients with GA have already been treated with stem cells.
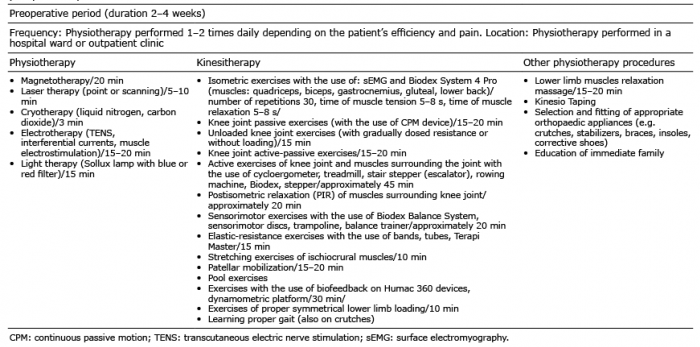
The application of preoperative procedures aims at improving the strength and endurance of muscles surrounding the knee joint (quadriceps, biceps, gastrocnemius, gluteal, and lower back), and isometric and stretching exercises for muscles surrounding the knee joint. In addition, it is necessary to perform exercises to improve the elasticity of the articulo-ligamentous apparatus of the knee joint. These include passive exercises (with the use of a continuous passive motion (CPM) device); unloaded knee joint exercises (with gradually dosed resistance or without loading); knee joint active-passive exercises; active exercises of the knee joint and muscles surrounding the joint with the use of cycloergometer, treadmill, stair stepper (escalator), rowing machine, and stepper lower limb muscle relaxation. Other types of exercise aim at increasing the range of knee joint motion: elastic-resistance exercises with the use of bands, tubes, Terapi Master (Redcore, Canada), and stretching exercises for the ischiocrural muscles. Other exercises restore physiological patellar tracking, which enables the patient to learn to walk using crutches. These include patellar mobilization, sensorimotor exercises with the use of the Biodex Balance System (Biodex, Shirley), sensorimotor discs, trampoline, balance trainer, and exercises for symmetrical lower limb loading. Physiotherapy applied in the inpatient hospital care period aims to prevent the effects of immobilization of the limb after surgery. This includes the introduction of anti-oedematous therapy, exercises that increase the range of mobility of the knee joint and the force of quadriceps muscle, ischiocrural muscles, gluteal muscles, as well as exercises that improve elasticity of the articulo-ligamentous apparatus of the knee joint. In this period, limb loading is prohibited for 6 weeks following surgery. Rehabilitation in the early outpatient period is conducted in outpatient settings for 6 weeks, and from week 7 to 3 months the patient can continue to be rehabilitated on an outpatient basis or, depending on their state of health, in the gym. In this period previous exercises are continued and attention is paid to the improvement of proprioception and to learning proper limb loading, which is fostered by exercises with the use of biofeedback on Humac 360 devices, dynamometric platform. The therapy can be assisted by physical therapy, which parameters are included in Tables I and III.
Table I. Algorithm of treatment and rehabilitation in degenerative arthritis of the knee with the use of CD34+ stem cells in the preoperative period
Table II. Algorithm of treatment and rehabilitation in degenerative arthritis of the knee with the use of CD34+ stem cells in the inpatient period
Table III. Algorithm of treatment and rehabilitation in degenerative arthritis of the knee with the use of CD34+ stem cells in the outpatient period
Stem cells are an important source of information on cellular differentiation, molecular processes and tissue homeostasis, but also one of the biological tools with most potential to treat degenerative diseases. They also exhibit high plasticity, i.e. the complex ability to adopt the expression profile and functional phenotypes of the cells that are typical of other tissues. The plasticity can be explained by transcription (direct or indirect) and fusion. Transcription consists of the acquisition of phenotypic identity of another tissue through the expression of the gene pattern (direct) or through the achievement of a more primitive state and the successive differentiation to another cell type (indirect). By fusion with a cell of another tissue, a cell can express a gene and acquire a phenotypic element of another parenchyma (14). From the physiological point of view, adult stem cells maintain tissue homeostasis as they are already partially committed, whereas embryonic stem cells are pluripotent and can generate all specific types of cells; they are derived from the placenta, membranes, amniotic fluid, or foetal tissues (15). Two sources of stem cells are found in the umbilical cord: umbilical epithelium and umbilical cord blood. The umbilical cord epithelium expresses a cytokeratin pattern similar to the human epidermis and is able to reproduce the tissue for dermatological application. In umbilical cord blood, hematopoietic and mesenchymal types of stem cells can be found, and they are characterized by a higher immunological tolerance (16–18). Moreover, foetal mesenchymal stem cell (FSCs) demonstrate greater expansion potential and differentiation abilities compared with stem cells from adult tissues (19). Adult stem cells can be obtained from mesodermal tissues of muscles, adipose tissue, synovial membranes and periosteum, from endodermal tissues of intestines and from the ectodermal tissues, such as nerve tissue or skin (20). Multipotent adult stem cells have been identified in almost all human organs and, for instance, human bone marrow is a reservoir for several progenitor stem cells, including haematopoietic stem cells (HSC), multipotent stromal stem cells, and endothelial stem cells (21). Stem cell therapy is used increasingly in many diseases, sometimes giving patients the only hope of recovery as, for example, in the case of spinal cord injuries. Studies have shown that olfactory cells are the source of progenitor stem cells for nerve repair. After transplantation, minor improvement was achieved in the function of upper limbs in tetraplegia and in the function of lower limbs in paraplegia (22, 23). Furthermore, stem cell therapy is used in autoimmune diseases of the central nervous system (CNS), in multiple sclerosis (MS) or amyotrophic lateral sclerosis. In MS a decrease in inflammation foci with disease stabilization was observed in patients under 40 years of age (24), whereas stem cell therapy in amyotrophic lateral sclerosis (ALS) is a promising strategy that can combine neuroprotection with recovery of neuromotor function (25, 26). Beneficial results have also been observed in patients with Parkinson’s disease in whom human embryonic brain tissue was implanted unilaterally, resulting in improved motor function (27). Promising results have been obtained in the treatment of ischaemic stroke. The use of a cell suspension consisting of immature nervous and haemapoietic tissues in patients with brain stroke consequences significantly improved functional activity in patients with consequences of brain stroke (28).
In other publications studies can be found on the use of stem cells in diseases such as heart failure (29, 30), ocular surface disorders (31, 32), and oncological diseases, in which stem cell therapy often prolongs life, especially in patients with metastases (33–36).
The use of stem cells in cell therapy is considered promising, due not only to the high proliferative capacity and the differentiation potential of various cells, but also to their functionality in secreting trophic molecules and counteract oxidative stress. To contribute effectively to organ repair, stem cells are expected to produce desirable therapeutic properties, e.g. minimal side-effects, integration into host tissue, differentiation to desired cell lines, immunomodulation or activation of endogenous repair mechanisms. However, although stem cell grafts may have therapeutic effects, they also have side-effects. Despite the initial enthusiasm for their potential therapeutic application, stem cells are associated with several problems in clinical practice. Firstly, self-renewal and plasticity are properties that primarily characterize cancer cells, and it is hypothesized that control could be lost in transplanted stem cells, or may act as a substrate for tumour development. Secondly, in case of allogeneic stem cell grafts, several cases of immunorejection of the graft have been reported despite the necessary immunosuppressive treatment to avoid immune response against the transplant and the consequent risk of infection (37, 38).
Modern methods of treating joint diseases in orthopaedics include minimally invasive surgery, arthroscopy, and biological treatment using stem cells found in the body. Stem cells are proliferative, so they can transform into the desired tissue, which should be capable of regeneration and self-repair. Autologous cells are used in orthopaedic surgery. For years they have been collected from bone marrow, but now they are more often removed from adipose tissue. In order to repair chondral or osteochondral defects, stem cells may be able to provide an abundant cell source, preventing the iatrogenic damage associated with the invasive isolation of chondrocytes used in autologous chondrocyte implantation strategies.
Stem cell therapy cannot be used in all patients. Firstly, the therapy works only when the joint is not completely damaged; secondly, it requires full involvement of the patient in the postoperative rehabilitation process; thirdly, existing risk factors for osteoarthritis, i.e. advanced age and obesity can affect stem cell properties. Indeed, adult stem cells derived from visceral adipose tissue of obese patients exhibit decreased cell proliferation, more rapid cell ageing and reduced cell differentiation (39).
The application of stem cell treatment in orthopaedics is a developing field that may have a significant effect on the future of orthopaedic surgery. However, it has tremendous potential to change the approach from reconstructive to regenerative and preventive treatment. One motivation for the direct injection of stem cells is that their anti-inflammatory function may be effective at preventing or delaying OA if delivered at early stages of the disease process. Percutaneous injection of mesenchymal stem cells into the knee joint with symptomatic and radiogra-phic degenerative joint disease resulted in decreased pain, increased joint mobility and improved cartilage growth (40). Jo et al. injected autologous adipose tissue-derived mesenchymal stem cells into the knee joint of patients with GA (40). After 6 months, the volume of cartilage in the femoral and tibial condyles increased, which contributed to improvement in knee joint function and decreased pain. Wakitani et al. were the first to report the regeneration of articular cartilage after transplantation of autologous MSCs embedded in a collagen gel (39). Based on the current state of clinical studies related to autologous stem cell therapy for OA of the knee, some authors have expressed concern about the stem cell type. Therefore, there is a need for a gold standard for autologous stem cell therapy for knee OA, which will be the goal of future clinical studies.
The use of stem cells is effective in the treatment of degenerative knee joint disease, with which the regeneration and restoration of cartilage and other periarticular structures is possible, enabling return to daily physical activity. The entire treatment process is associated with the application of an appropriate rehabilitation programme that allows the patient to be adequately prepared for stem cell transplantation.


 Click to show fullsize
Click to show fullsize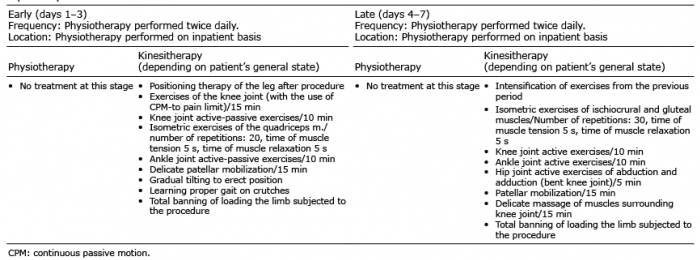 Click to show fullsize
Click to show fullsize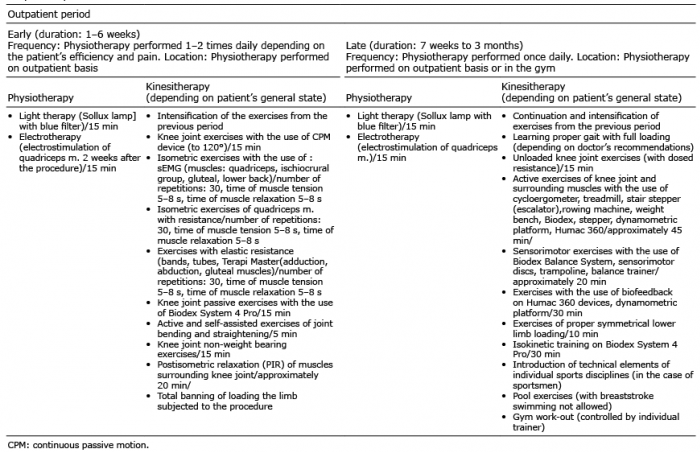 Click to show fullsize
Click to show fullsize