ARE NEURORADIOLOGICAL OR NEUROPHYSIOLOGICAL CHARACTERISTICS ASSOCIATED WITH UPPER-EXTREMITY HYPERTONIA IN SEVERE ISCHAEMIc SUPRATENTORIAL STROKE?
Annette A. van Kuijk, MD1,4, Henk T. Hendricks, MD, PhD1, Jaco W. Pasman, MD, PhD2, Berry H. Kremer, MD, PhD3 and Alexander C. Geurts, MD, PhD1
From the Departments of 1Rehabilitation Medicine, 2Clinical Neurophysiology and 3Neurology, Radboud University Medical Centre, Nijmegen, and 4Rehabilitation Centre Tolbrug, ‘s-Hertogenbosch, The Netherlands
OBJECTIVE: The primary goal was to identify the neuroradiological and neurophysiological risk factors for upper-extremity hypertonia in patients with severe ischaemic supratentorial stroke.
DESIGN: Inception cohort.
Patients: Forty-three consecutive patients with an acute ischaemic supratentorial stroke and an initial upper-extremity paralysis admitted to an academic hospital recruited over a 1.5-year period.
Main outcome measures: Upper-extremity hypertonia was assessed by the Ashworth scale and clinically relevant hypertonia was defined as Ashworth scale ≥2. Any association of (clinically relevant) hypertonia with neuroradiological (lesion side, extent of lesion, and stroke history), and neurophysiological (motor-evoked potential and silent period) characteristics was investigated.
RESULTS: Associations between hypertonia and the selected neuroradiological and neurophysiological risk factors were generally low. Univariate analyses yielded none of the selected neuroradiological or neurophysiological characteristics as significantly associated with hypertonia.
CONCLUSION: Despite the high incidence of hypertonia in these patients, we could not identify any of the selected neuroradiological or neurophysiological characteristics as a risk factor for hypertonia.
Key words: stroke, upper extremity, hypertonia, transcranial magnetic stimulation, computerized tomography, prediction.
J Rehabil Med 2007; 39: 38–42
Correspondence address: A. A. van Kuijk, Rehabilitation Centre Tolbrug, PO Box 90153, NL-5200 ME ‘s-Hertogenbosch, The Netherlands. E-mail: a.v.kuijk@tolbrug.nl
Submitted April 18, 2006; accepted July 11, 2006.
Introduction
Spasticity is a characteristic component of the upper motor neurone syndrome in the post-acute and chronic phases of stroke. The precise relationship between spasticity elicited by passive tendon or muscle stretch and active movement capacity, however, remains unclear. In the upper extremity, spasticity may cause difficulty with basic arm and hand abilities, such as reaching and grasping, as well as with many more complex activities of daily living (ADL) (1–5). Functional effects of spasticity treatment seem to depend highly on a critical selection of subjects, individualized goal setting, and appropriate selection of outcome measures (6–9). In particular, patients after severe stroke with a low potential for motor recovery may profit from a pro-active treatment approach to prevent disabling spasticity and the functional consequences of secondary complications, such as muscles stiffness, contractures and pain. Against this background, it seems clinically relevant to assess, besides the probability of motor recovery, the risk of developing spasticity in these patients early after stroke.
Studies on risk factors for post-stroke spasticity are, however, scarce and complicated by the inability of clinical measures to distinguish between the neural mechanisms and the secondary intrinsic changes in muscle properties. Indeed, the clinical assessment of spasticity incorporates both neural and non-neural mechanisms by grading resistance against passive stretch (hypertonia). As for clinical risk factors, as yet, only modest associations of early muscle weakness and a low initial Barthel Index (BI) with chronic hypertonia have been found (10). In a companion paper describing the same selected study population of patients after stroke with an initial paralysis of the upper extremity and a BI of 0, we were unable to identify any clinical characteristic as an additional risk factor for early or persistent hypertonia, despite the high incidence of hypertonia observed in these patients (11). In this perspective, it is a logical step to investigate whether specific neuroradiological or neurophysiological characteristics might be associated with early or persistent hypertonia.
Neuroradiological assessments (magnetic resonance imaging or computerized tomography (CT) scan) in patients after acute stroke are performed on a routine basis to confirm diagnosis and differentiate lesion type. Some neuroradiological characteristics (lesion type, size and site) have been associated with motor recovery and functional outcome, however, as yet, there remains much debate on whether stroke location or size are associated with hypertonia (12–15). Clinical heterogeneity with regard to both patient-groups and time post-stroke may be an important factor contributing to these inconsistencies in the literature.
Transcranial magnetic stimulation (TMS) has also become appreciated as a diagnostic and prognostic tool in patients after stroke (16). In tonically pre-activated muscles, TMS of the primary motor cortex induces a short-latency motor-evoked potential (MEP) in the electromyogram as an excitatory effect, followed by a transitory suppression of the electromyographic activity, the silent period (SP), as an inhibitory effect (Fig. 1). Although motor recovery can be predicted reasonably well by TMS (17, 18), early prediction of hypertonia based on TMS is much more difficult. In patients with chronic stroke and subacute stroke with focal vascular brain lesions, an association has been found between shortening of the SP and hypertonia as assessed by the Ashworth scale (AS) (19–21). Studies regarding these neurophysiological characteristics as potential risk factors for hypertonia in patients with acute stroke are, however, lacking.
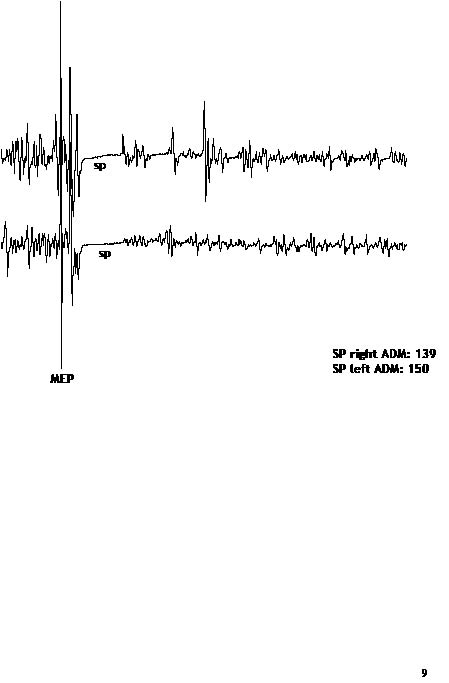
Fig. 1. Example of a motor-evoked potential (MEP) and silent period (SP) in the abductor digiti minimi muscle (ADM).
Against this background, we conducted a prospective cohort study including only acute stroke patients with an initial paralysis of the upper extremity to maximize the likelihood of observing hypertonia and, thus, to optimize the chance of identifying additional risk factors for post-stroke upper- extremity hypertonia. We investigated the association of neuroradiological (lesion side and extent) and neurophysiological characteristics (MEP and SP) with early and late hypertonia, since these laboratory measures can be easily obtained in most hospitals with an acute stroke unit.
Material and Methods
Patients
As part of a larger study on the value of MEP in predicting motor and functional outcome after stroke (18), 43 consecutive acute patients with an ischaemic supratentorial stroke were recruited during a 1.5-year period. These patients were admitted to the Department of Neurology at the Radboud University Medical Centre Nijmegen. The diagnosis of stroke was made clinically by a neurologist according to the World Health Organization (WHO) clinical criteria (22) and confirmed by CT scan.
Only patients presenting at day 1 post-stroke with no voluntary muscle activity and no muscle tone at the elbow, wrist or finger flexors (Brunnstrom stage I (23)) were included within the first 7 days post-stroke. Patients with a poor prognosis for survival (loss of consciousness, severe CT abnormalities, and severe co-morbidity) as well as patients with severe pre-existing impairments of the upper extremity of any type (e.g. rheumatic deformities, contractures) were excluded. Patients with a history of craniotomy, epilepsy, cardiac prosthetic valve or pacemaker implantation, or severe polyneuropathy were also excluded. The local ethics committee approved the study protocol and written informed consent was obtained from all patients before study entry.
Each patient received “best medical treatment” according to the guidelines of the Netherlands Society of Neurology, ensuring that each patient received physiotherapy to maintain optimal passive and active range of motion of all upper extremity joints from day 1 post-stroke. However, for the first 3 weeks post-stroke, no specific therapy was initiated aimed at facilitation of arm-hand function recovery.
Potential risk factors
Neuroradiological assessment. In each patient, a CT scan of the brain was made twice; the first time on the day of admission and the second time at week 1 post-stroke to delineate the structural lesion. Both an independent neuroradiologist and a neurologist (BK) assessed the CT scans of all patients, independently of one another. Evidence of previous stroke (“present” or “absent”) as well as the extent of the (structural) vascular lesions (“extensive” or “focal”) were recorded. Extensive stroke was defined as lesions with a diameter ≥5 cm and/or located in both subcortical and cortical areas. Stroke lesions with a diameter less than 5 cm and restricted to the subcortical areas (subcortical white matter and/or basal ganglia and/or internal capsule) were regarded as focal. Both assessors were blinded with regard to the neurophysiological and clinical assessments. In the case of disagreement between the assessors, consensus was established afterwards.
Neurophysiological assessment. TMS of the motor cortex was performed twice in each patient; at first, within 1 week post-stroke (t1) and, secondly, at 3 weeks post-stroke (t2) by the same experienced clinical neurophysiologist (JP). This clinical neurophysiologist was blinded with regard to the results of the clinical and neuroradiological assessments. Patients were positioned comfortably in a supine position. TMS was performed through a 90 mm circular coil placed in a tangential plane above the vertex and powered by a Magstim 200 magnetic stimulator. The stimulus intensity was set at maximum stimulator output. To obtain a preferential activation of each hemisphere, a clockwise inducing current flow was used for the right hemisphere and a counter-clockwise current for the left hemisphere. MEPs were recorded at t1 and t2 from the biceps brachii muscle (BB) and the abductor digiti minimi muscle (ADM) on both the affected and the unaffected side. SPs were recorded at t1 and t2 from the ADM, as a representative muscle for distal motor function of the upper extremity. Recordings were made using an Oxford Synergy electromyograph with filter settings of 20 Hz and 3 kHz (amplifier range 100 mV and display sensitivity of 0.5 mV/division). A 500-millisecond post-stimulus period was analysed. The MEPs and SPs were preferably recorded when facilitated by a slight voluntary ADM contraction. When patients could not elicit a contraction of the affected hand muscle, they were asked to activate the non-paretic ADM (24). At least 2 responses were obtained to assess the reproducibility. The presence of a MEP was defined as any reproducible response with minimal peak-to-peak amplitude of 200 µmV. The absence of a positive MEP at t2 was regarded as a potential risk factor for post-stroke hypertonia. Responses with the highest MEP amplitude were used for analysis. The SP length was measured from ADM-MEP onset until the return of uninterrupted voluntary electromyography activity. Responses with the shortest SP length were used for analysis. Data from the non-paretic arm were compared with normative data and used as a reference. Finally, the BB and ADM responses (mean MEP amplitude and SP duration) were studied separately for both the paretic and the non-paretic side.
Outcome assessment
Hypertonia was clinically assessed by grading muscle tone through the AS (25). Muscle tone (grade 0–4) was assessed within the first 24 h and consecutively at weeks 1, 2, 3, 6, 12 and 26 post-stroke under standardized test conditions by a rehabilitation specialist (HH). The precise technique of assessment has been described in a companion paper (11). Clinically relevant hypertonia was operationally defined as an AS score equal to or greater than 2 in at least one joint.
Data analysis
The MEP amplitude and SP duration obtained from the ADM and the BB on the paretic side were compared with the corresponding values obtained from the non-paretic side using Student’s t-test.
In addition, from 2×2 contingency tables, positive and negative predictive values for each of the potential risk factors with their 95% confidence interval were calculated. In case of positive outcome of the univariate analysis, multiple backwards logistic regression was planned to determine the explained variance by each characteristic with regard to hypertonia, independent of its possible association with other characteristics.
Results
Neuroradiological and TMS characteristics
Three patients were excluded from the study; 2 patients died within the first 2 weeks post-stroke and another patient suffered from a recurrent stroke at week 13 resulting in a poor prognosis for survival. All 3 patients continued to have a flaccid paralysis of the upper extremity from clinical presentation. Thus, 40 patients, 20 women and 20 men, completed the study. The median age was 68 years (interquartile range 59–77 years). The neuroradiological characteristics of these 40 patients are shown in Table I. Sixteen (40%) patients had had previous stroke, whereas 24 (60%) patients had had a first-ever stroke. Twenty-nine patients had extensive lesions that were located in the territory of the MCA involving cortical (n=2), subcortical (n = 1), or both cortical and subcortical areas (n=26). Eleven patients had a focal, subcortically located lesion. In 4 of these patients the lesion was restricted to the basal ganglia.
| Table I. Neuroradiological characteristics of the 40 patients | ||
| Characteristics | n | |
| Stroke history | First ever | 24 |
| Previous | 16 | |
| Lesion side | Left | 22 |
| Right | 18 | |
| Infarct size | Small (<2 cm) | 1 |
| Moderate (2–5 cm) | 16 | |
| Extensive (>5 cm) | 23 | |
| Infarct localization | Cortical | 2 |
| Subcortical | 12 | |
| Cortical/subcortical | 26 | |
| Extent of stroke lesion | Focal | 11 |
| Extensive | 29 | |
TMS of the motor cortex was performed in all patients, however, 4 patients refused the second MEP assessment. Two of these patients developed hypertonia, one patient within the first week post-stroke. In the other patient, hypertonia was observed from the 6th week post-stroke. Thus, the complete MEP data-set was available for only 36 patients. The quantitative aspects of the TMS recordings are summarized in Table II for the subgroups of patients in which a positive MEP was obtained at t1 and t2. At both times, the MEP amplitudes in the BB and the ADM were significantly lower on the paretic than on the non-paretic side.
| Table II. Transcranial magnetic stimulation characteristics for both the biceps brachii (BB) and abductor digiti minimi (ADM) muscle in patients obtaining a positive motor-evoked potential at week 1 and week 3 post-stroke | ||||||
| Paretic side Mean (SD) | Non-paretic side Mean (SD) | Paired sample t-test p-value | Patients (n) | |||
| BB | Amplitude | Week 1 | 1.47 (1.27) | 5.46 (5.26) | 0.05 | 9 |
| (mV) | Week 3 | 1.59 (1.74) | 6.11 (3.28) | 0.00 | 15 | |
| ADM | Amplitude | Week 1 | 2.22 (1.97) | 6.68 (2.52) | 0.00 | 6 |
| (mV) | Week 3 | 2.28 (2.41) | 7.51 (1.63) | 0.00 | 10 | |
| Silent period | Week 1 | – | – | – | 0 | |
| (msec) | Week 3 | 336.75 (106.90) | 202.50 (29.46) | 0.11 | 4 | |
Potential risk factors for post-stroke hypertonia
From a clinical point of view, we were most interested in predicting persistent hypertonia. Therefore, we considered hypertonia at the 26th week post-stroke as the primary outcome. Both at t1 and at t2 no differences in MEP amplitude on the paretic side could be found between patients with and without hypertonia (Table III). At t1 no SP could be elicited at the paretic side in any of our patients, whereas at t2 only in 4 patients a SP could be determined: 2 patients with and 2 without hypertonia. No difference in SP duration between these small patient groups was found.
| Table III. Transcranial magnetic stimulation characteristics in both the biceps brachii (BB) and abductor digiti minimi (ADM) muscle at week 1 and at week 3 post-stroke in relation to hypertonia | |||||||
| Patients with hypertonia | Patients without hypertonia | Independent sample | |||||
| n | n | t-test p-value | |||||
| BB | Amplitude (mV) Mean (SD) | Week 1 | 1.20 (1.31) | 7 | 2.40 (0.71) | 2 | 0.266 |
| Week 3 | 1.11 (1.44) | 10 | 2.56 (2.04) | 5 | 0.132 | ||
| ADM | Amplitude (mV) Mean (SD) | Week 1 | 2.15 (2.10) | 4 | 2.35 (2.48) | 2 | 0.921 |
| Week 3 | 2.28 (2.91) | 6 | 2.27 (1.50) | 4 | 0.993 | ||
| Silent period length (msec) | Week 1 | – | 0 | – | 0 | – | |
| Week 3 | 327.00† 487.00† | 2 | 237.00† 296.00† | 2 | * | ||
| *Not calculated; †: individual data (data per patient) at week 3. | |||||||
In univariate analyses, all associations between hypertonia at week 26 and the selected potential risk factors were low and statistically not significant (Table IV). Table IV shows the positive and negative predictive values with their 95% confidence intervals for all factors. The positive predictive values varied from 0.52 to 0.68 and the negative values from 0.36 to 0.61. Changing the definition of persistent hypertonia into AS ≥2 at the 12th week or at the 6th week post-stroke yielded similar results. Even if clinically relevant hypertonia was defined as AS ≥1, or if hypertonia at any time post-stroke was used as the primary outcome, no association with the selected potential risk factors could be demonstrated.
Discussion
This study aimed to investigate to what extent selected neuroradiological and neurophysiological characteristics can be considered as risk factors for developing upper extremity hypertonia in patients with severe ischaemic supratentorial stroke. With regard to the neuroradiological assessments, the observed lack of association between the extent of the vascular lesion and hypertonia is consistent with the study of Patano et al. (12), who also found no correlation between lesion volume and muscle tone. Having had a previous stroke or the side of the lesion was also not significantly associated with hypertonia (Table IV). In general, the lack of association between stroke location and hypertonia in our study may have been influenced by the fact that the majority of our patients suffered from extensive lesions on CT involving both the cortical and subcortical areas. In the literature, there also remains much debate on the influence of stroke location on the occurrence of hypertonia (12–15), which may well be related to the fact that the applied methods to localize and measure the lesions lack sufficient sensitivity.
| Table IV. Associations between potential risk factors and hypertonia (HT) at 26 weeks post-stroke | |||
| With HT (n) | Without HT (n) | PPV and NPV (95% CI) | |
| Lesion side | |||
| Left | 15 | 7 | PPV 0.68 (0.49–0.88) |
| Right | 7 | 11 | NPV 0.61 (0.39–0.84) |
| Previous stroke | |||
| Present | 14 | 10 | PPV 0.58 (0.38–0.78) |
| Absent | 8 | 8 | NPV 0.50 (0.25–0.75) |
| Extensive stroke | |||
| Present | 15 | 14 | PPV 0.52 (0.34–0.71) |
| Absent | 7 | 4 | NPV 0.36 (0.03–0.69) |
| ADM – MEP | |||
| at week 3 | |||
| Absent | 18 | 12 | PPV 0.60 (0.43–0.78) |
| Present | 4 | 6 | NPV 0.60 (0.30–0.90) |
| ADM – MEP: abductor digiti minimi – motor evoked potential; PPV: positive predictive values; NPV: negative predictive values; CI: confidence interval. | |||
The selected neurophysiological measures obtained by TMS did not show a significant association with the occurrence of hypertonia either. Although it has been shown that muscle weakness is a clinical risk factor for post-stroke hypertonia, the absence of an ADM-MEP at the 3rd week post-stroke was not associated with hypertonia. This negative result can be explained by the fact that hypertonia may not directly result from damage to the corticospinal pathways, but from concomitant damage to the para-pyramidal pathways (26). At the cerebral level, there may be a loss of the cortical drive to several inhibitory centres in the brainstem, e.g. the origin of the lateral reticulospinal tract, resulting in disinhibition of bulbar and spinal reflexes (26–28). This loss of cortical drive may be due to lesions within areas projecting to the primary motor cortex (such as the primary somatosensory area, supplementary motor area, the pre-motor area, basal ganglia, thalamus and cerebellum. These brain areas provide important modulatory inputs to the primary motor cortex and lesions within these areas might, therefore, lead to a subsequent change in the balance between excitatory and inhibitory influences on the intra-cortical motor neurones that project to inhibitory centres at the level of the brainstem. Although these para-pyramidal pathways cannot be directly assessed, they might be indirectly assessed by TMS. Nevertheless, the results of this study do not support this clinical reasoning.
In chronic stroke patients, Uozumi et al. (19) and Cruz-Martinez et al. (20) found a possible association between TMS-induced inhibitory phenomena (SP) and hypertonia. The authors hypothesized that in the course of the development of hypertonia, cortical inhibition decreases and, subsequently, the SP shortens. In patients with subacute (≤2 weeks) stroke with a focal ischaemic lesion in the territory of the middle cerebral artery, Catano et al. (21) observed a decrease in SP duration with increasing muscle contraction. This contraction-induced reduction of the SP was associated with hypertonia. Although this (relative) inefficacy of the inhibitory mechanisms might be a risk factor for hypertonia, the phenomenon of contraction-induced reduction of the SP could not be assessed in our study. The voluntary contraction of the hand muscles in the majority of our patients was so severely impaired that often no SP could be recorded. Even patients in whom a SP could be elicited lacked the ability to elicit different degrees of voluntary contraction. As a result, in only 4 out of 40 patients (10%) a SP could be determined at 3 weeks post-stroke. The mean duration of the SP in 2 patients with hypertonia did not differ from the mean SP duration in 2 other patients without hypertonia. However, due to these small numbers of patients, the finding that the SP was not related to hypertonia in this acute-phase study must be interpreted with care.
It is important to note that this study was restricted to a homogeneous group of patients with acute stroke with initial paralysis of the upper extremity and a BI of 0. Predicting hypertonia using neuroradiological and neurophysiological characteristics as potential risk factors in such a severe subgroup restricts generalization of the outcomes to less severely affected patients. Moreover, this severe subgroup is probably not the most appropriate group to study the value of TMS- induced inhibitory phenomena. These patients lack the ability to move their affected limb voluntarily and selectively, which is necessary to generate a MEP and a subsequent SP.
Another possible limitation of this study may still be a lack of power due to the limited number of patients. We included only patients with initial paralysis to optimize the risk of post-stroke hypertonia (approximately 62%). This subgroup comprises however, only 19–30% of the stroke population at large (29). As a result, the inclusion rate was relatively low in just one academic hospital. Still, 40 patients should be a sufficient number to distinguish a “moderate” from an “absent” association between hypertonia and any clinical determinant (setting a at 0.05 and 1-b at 0.80). Larger studies of high-risk patients are needed to identify “weaker”, but significant, associations.
In conclusion, as yet, the association of neuroradiological stroke characteristics as well as TMS-induced excitatory and inhibitory phenomena with hypertonia seems to be weak, even in patients with severe stroke with upper extremity paralysis. In addition, TMS characteristics, such as the contraction-induced inhibition of the SP, are not applicable in these patients during the acute and subacute phases post-stroke.
References
1. Katz RT, Rovai GP, Brait C, Rymer WZ. Objective quantification of spastic hypertonia: correlation with clinical findings. Arch Phys Med Rehabil 1992; 73: 339–347.
2. Katz RT, Rymer WZ. Spastic hypertonia. Mechanisms and measurement. Arch Phys Med Rehabil 1989; 70: 144–155.
3. Mayer NH, Esquenazi A, Childers MK. Common patterns of clinical motor dysfunction. Muscle Nerve 1997; Suppl 6: S21–35.
4. Sommerfeld DK, Eek EU, Svensson AK, Holmqvist LW, von Arbin MH. Spasticity after stroke. Its occurrence and association with motor impairments and activity limitations. Stroke 2004; 35: 134–139.
5. Lin FM, Sabbahi M. Correlation of spasticity with hyperactive stretch reflexes and motor dysfunction in hemiplegia. Arch Phys Med Rehabil 1999; 80: 526–530.
6. Brashear A, Gordon MF, Elovic E, Kassicieh D, Marciniak C, Do M, et al. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after stroke. N Engl J Med 2002; 347: 395–400.
7. Francis HP, Wade DT, Turner-Stokes L, Kingswell RS, Coxon EA. Does reducing spasticity translate into functional benefit? An exploratory meta-analysis. J Neurol Neurosurg Psychiatry 2004; 75: 1547–1551.
8. Miscio G, Del Conte C, Pianca D, Colombo R, Panizza M, Schieppati M, et al. Botulinum toxin in post-stroke patients: stiffness modifications and clinical implications. J Neurol 2004; 251: 189–196.
9. Gordon MF, Brashear A, Elovic E, Kassiciech D, Marciniak C, Liu J, et al. Repeated dosing of botulinum toxin type A for upper limb spasticity following stroke. Neurology 2004; 63: 1971–1973.
10. Leathly MJ, Gregson JM, Moore AP, Smith TL, Sharma AK, Watkins CL. Predicting spasticity after stroke in those surviving to 12 months. Clin Rehabil 2004; 18: 438–443.
11. van Kuijk AA, Hendricks HT, Pasman JW, Kremer HPH, Geurts ACH. Are clinical characteristics associated with upper-extremity hypertonia in severe ischemic supratentorial stroke? J Rehabil Med 2006; xx: xx–xx [complete ref required]
12. Patano P, Formisano R, Ricci M, Di Piero V, Sabatini U, Barbanti P, et al. Prolonged muscular flaccidity after stroke. Morphological and functional brain alterations. Brain 1995; 118: 1329–1338.
13. Kunesch E, Binkofski F, Steinmetz H, Freund HJ. The pattern of motor deficits in relation to the site of stroke lesions. Eur Neurol 1995; 35: 20–26.
14. Fries W, Danek A, Scheidtmann K, Hamburger C. Motor recovery following capsular stroke. Role of descending pathways from multiple motor areas. Brain 1993; 116: 369–382.
15. Sherman SJ, Koshland GF, Laguna JF. Hyper-reflexia without spasticity after unilateral infarct of the medullary pyramid. J Neurol Sci 2000; 175: 145–155.
16. Wolf SL, Butler AJ, Alberts JL, Kim MW. Contemporary linkages between EMG, kinetics and stroke rehabilitation. J Electromyogr Kinesiol 2005; 15: 229–239.
17. Hendricks HT, van Limbeek J, Plat FM, Zwarts MJ. Systematic review for the prediction of motor and functional outcome after stroke using motor evoked potentials. Arch Phys Med Rehabil 2002; 83: 1303–1308.
18. Hendricks HT, Pasman JW, van Limbeek J, Zwarts MJ. Motor-evoked potentials in predicting recovery from upper extremity paralysis after acute stroke. Cerebrovasc Dis 2003; 16: 265–271.
19. Uozumi T, Ito Y, Tsuji S, Murai Y. Inhibitory period following motor evoked potentials evoked by magnetic cortical stimulation. Electroencephalogr Clin Neurophysiol 1992; 85: 273–279.
20. Cruz-Martinez A, Munoz J, Palacios F. The muscle inhibitory period by transcranial magnetic stimulation. Study in stroke patients. Electromyogr Clin Neurophysiol 1998; 38: 189–192.
21. Catano A, Houa M, Noel P. Magnetic transcranial stimulation. Clinical interest of the silent period in acute and chronic stages of stroke. Electroencephalogr Clin Neurophysiol 1997; 105: 290–296.
22. WHO task force on stroke and other cerebrovascular disorders. Stroke – 1989. Recommendations on stroke prevention, diagnosis, and therapy. Stroke 1989; 20: 1407–1431.
23. Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand J Rehab Med 1975; 7: 13–31.
24. Hess CW, Mills KR, Murray NMF. Responses in small hand muscles from magnetic stimulation of the human brain. J Physiol 1987; 388: 397–419.
25. Ashworth B. Preliminary trial of carisprodal in multiple sclerosis. Practioner 1964; 192: 540–542.
26. Sheean G, editor. Spasticity rehabilitation. Edinburgh: Churchill Communication Europe; 1998.
27. Brown P. Pathophysiology of spasticity. J Neurol Neurosurg Psych 1994; 57: 773–777.
28. Van Kuijk AA, Pasman JW, Geurts ACH, Hendricks HT. How salient is the silent period? The role of the silent period in the prognosis of upper-extremity motor recovery after severe stroke. J Clin Neurophysiol 2005; 22: 10–24.
29. Jørgensen HS, Reith J, Nakayama H, Kammersgaard LP, Raaschou HO, Olsen TS. What determines good recovery in patients with the most severe strokes? The Copenhagen Stroke Study. Stroke 1999; 30: 2008–2012.

