OBJECTIVE: To study future general and diagnoses-specific sickness absence and disability pension among young adults who were initially on long-term sick-leave due to back, neck, or shoulder diagnoses.
DESIGN: Eleven-year prospective cohort study.
SUBJECTS: All 213 adults in a Swedish municipality who, in 1985, were in the age range 25–34 years and had begun a spell of sick-leave lasting ≥ 28 days with low back, neck, or shoulder diagnoses.
METHODS: For the time-period 1985–96, data regarding the dates and diagnoses for all periods of sick-leave, and the dates of disability pension, emigration, and death were obtained. Numbers of days of sick-leave and disability pension were analysed separately for each of the 11 years in relation to the number of days at risk for such benefits.
RESULTS: The cohort members were on sick-leave or disability pension for 25% of all days at risk during the 11 years of follow-up. A large difference in the number of sick-leave days between the 22% of subjects who were later granted disability pension and the others was already apparent during the first 2 years. During the entire period, up to 21% of the sick-leave days for women and 24% for men entailed psychiatric diagnoses.
CONCLUSION: This cohort of young adults, initially off sick for 4 weeks due to back, neck, or shoulder diagnoses, also had a high level of sickness absence in the subsequent 11 years with other diagnoses.
Key words: sickness absence, sick-leave, disability pension, sick-leave diagnoses.
J Rehabil Med 2009; 41: 423–428
Correspondence address: Karin Festin, Division of Social Medicine and Public Health Science, Department of Medical and Health Sciences, Linköping University, SE-581 83 Linköping, Sweden. E-mail: karin.festin@liu.se
Submitted November 19, 2007; accepted January 22, 2009
INTRODUCTION
In many Western countries today, sickness absence is considered to be a public health problem with substantial consequences for society and workplaces, as well as for the affected individuals and their families (1–4). Nevertheless, few studies have concerned the long-term, e.g. several years, prognoses of future sickness absence in general and with specific diagnoses (2, 5). Such knowledge would be helpful for physicians when discussing the possible consequences of long-term sickness absence with patients (6, 7).
Many persons have prolonged or recurrent spells of sick-leave, especially when absence is due to musculoskeletal disorders (8–11). Studies often cover short periods (1–2 years) or are retrospective (12). Little is known about whether future absences are due to the same or other sick-leave diagnoses in a long-term perspective. Thus, knowledge of the prognoses of sickness absentees is limited. Are the persons generally sick-listed due to the same diagnoses or do diagnoses change? What is the risk of prolonged sickness absence if a person of a certain age has a particular diagnosis? What are the corresponding risks for future disability pension or further sickness absence with the same or other diagnoses?
The lack of studies concerning possible changes in sick-leave diagnoses over time is probably related to the fact that, for ethical reasons, the social insurance offices in most countries are not permitted to keep computerized records. Accordingly, diagnoses have to be retrieved manually from filed sickness certificates. Furthermore, analysis of sick-leave over time entails several statistical challenges that are associated with, among other things, recurrent events and uneven distribution of incidence and duration (13, 14).
Our aim was to analyse the pattern of sick-leave, both in general and in specific sick-leave diagnoses, over 11 years in a cohort of young adults initially long-term sickness absent due to low back, neck, or shoulder diagnoses.
MATERIALS AND METHODS
An 11-year prospective cohort study was conducted that included all individuals who met the following criteria in 1985 (15): (i) lived in the Swedish municipality of Linköping (population 117,000); (ii) aged 25–34 years; (iii) began a new spell of sick-leave of ≥ 28 days due to neck, shoulder, or low back problems classified as displacement of lumbar intervertebral disc (725), lumbago (7170), sciatica (7288), other deformities (738r), humeroscapular periarthritis (7171), myalgia (7179), cervicalgia (7280), cervicobrachialgia (7282), or tendovaginitis (731). According to the diagnostic codes of the Nordic Medicostatistical Committee, based on ICD-8 (16), the first 4 conditions mentioned above are referred to as low back diagnoses and the others as neck/shoulder diagnoses. Back problems related to pregnancy were excluded.
Subjects were identified from a large research database comprising all spells of sick-leave > 7 days in Östergötland County in 1985 (17, 18). Those diagnoses were selected because they represented (and still represent) the most common diagnoses underlying sickness absence (3, 13, 19). The reason for studying young adults was to research the possible negative consequences of long-term sick-leave (e.g. marginalization and disability pension) that might be more serious in that age group than in older people. Having spells of sick-leave lasting ≥ 28 days was chosen as an inclusion criterion, because after that period of time an employer would have been compelled to submit a plan for rehabilitation measures to a Social Insurance Office. The diagnoses and number of days in the spell of sick-leave used as an inclusion criterion were double-checked manually through the sickness certificates stored at the local Social Insurance Offices (13). The validity of these diagnoses had been tested previously and found acceptable (20, 21).
In 1985, 14,914 of the residents of the municipality of Linköping were in the age range 25–34 years. Of those individuals, 6.8% had begun a new spell of sick-leave ≥ 28 days, and 1.4% (n = 213) had at least one such spell due to neck, shoulder, or low back diagnoses and were therefore included in the study. Data on each of these 213 individuals (61% women) in the cohort were collected from the following 3 sources for the period 1 January 1985 to 1 September 1996: (i) from the National Social Insurance Office – information about sex, dates of emigration as well as dates, grades (full- or part-time), type (temporary or permanent) and diagnoses of disability pension; (ii) from the local Social Insurance Offices – information regarding all sick-leave periods (dates, diagnoses, full- or part-time) was retrieved manually from each sickness certificate filed by the local offices, also from the offices for those who had moved from the city of Linköping over the years (13); (iii) from the National Death Registry – dates of death up to 1 September 1996.
Data on disability pension was included since this type of benefit is closely related to sick-leave compensation and those 2 benefit systems are sometimes regarded as communicating vessels.
According to our definition, a period of sick-leave comprises the uninterrupted period of days stipulated on a sickness certificate. During such a period, the diagnoses and degree of absence (e.g. part- or full-time) are not changed. A spell of sick-leave is defined as one or more consecutive sick-leave periods.
Data analyses
Partial sick-leave or disability-pension days were converted into whole days. For example, 2 days with 50% leave were counted as one whole sick-leave day. The numbers of days on sick-leave and in receipt of disability pension were calculated separately and combined as a total, referred to as sickness compensation days.
For each person and year, days at risk of sickness compensation were determined as number of calendar days until censoring (due to death or emigration) or until the study ended on 1 September 1996. For 1985, the number of days a person was considered at risk covered all days from the first day in the spell of sick-leave used as inclusion criterion (i.e. the first spell with a back, neck, or shoulder diagnosis lasting ≥ 28 days) up to 31 December. Sickness compensation days were analysed in relation to the number of days at risk for sickness and disability benefits.
Days of disability pension were excluded from the analyses of changes in sick-leave diagnoses, and any individual who was granted full-time disability pension was censored as not being at risk of any subsequent sick-leave days. The diagnoses for the sick-leave periods were initially classified into the 18 groups of ICD-8 diagnoses applied in treatment of out-patients (Table I) (16). If more than one diagnosis was given on a sickness certificate, the first diagnosis was used in the analyses. A medical officer and a specialist in social medicine and general practice helped interpret the sick notes that were barely legible. Nearly 6% of the sick-leave periods (n = 471) lacked a diagnosis, but had information on dates and degree of absence, and in most cases also the name of the issuing physician and/or clinic. Most of those certificates covered only a few days between longer sick-leave periods, and were usually provided because the person had been hospitalized. Each such intervening period was assigned to a plausible diagnostic category by considering the diagnoses for the sick-leave periods that occurred immediately before and after the period in question and also the type of clinic at which the certifying physician worked. This task was performed separately and independently by a physician who was well acquainted with the different clinics and by a medical student. They agreed on the same classification for all but 61 of the 471 certificates, which were assigned to group 16, designated “symptoms, signs, and abnormal clinical and laboratory findings not elsewhere classified”. For government employees, sickness certificates for spells < 14 days were not sent to the Social Insurance Offices, thus we were unable to obtain information on the diagnoses for those 169 short sick-leave periods. Accordingly, those periods were also classified as belonging to group 16.
|
Table I. Number of sick-leave days in 1985–1996 related to various diagnostic groups shown for women (n = 129) and men (n = 84) initially sick-listed for four weeks in 1985 due to low back, neck, or shoulder diagnoses
|
|
Group of diagnosis
|
Women
|
%
|
Men
|
%
|
|
I Certain infectious and parasitic diseases
|
1,926
|
2
|
1,815
|
3
|
|
II Neoplasms
|
1,102
|
1
|
–
|
< 1
|
|
III Endocrine, nutritional, and metabolic diseases
|
428
|
< 1
|
451
|
1
|
|
IV Diseases of the blood and blood-forming organs
|
17
|
< 1
|
–
|
< 1
|
|
V Mental and behavioural disorders (total)
|
6,071
|
6
|
8,872
|
15
|
|
a) Depression
|
4,865
|
5
|
7,577
|
13
|
|
b) Abuse
|
949
|
1
|
1,084
|
2
|
|
c) Other
|
258
|
< 1
|
211
|
< 1
|
|
VI Inflammatory diseases of the central nervous system
|
2,502
|
3
|
453
|
1
|
|
VII Diseases of the circulatory system
|
391
|
< 1
|
454
|
1
|
|
VIII Diseases of the respiratory system
|
5,272
|
5
|
1,983
|
3
|
|
IX Diseases of digestive system
|
1,523
|
2
|
1,477
|
3
|
|
X Diseases of the genitourinary system
|
1,345
|
1
|
102
|
< 1
|
|
XI Pregnancy, childbirth, and the puerperium
|
3,095
|
3
|
–
|
–
|
|
XII Diseases of the skin and subcutaneous tissue
|
1,873
|
2
|
168
|
< 1
|
|
XIII Diseases of the musculoskeletal system and connective tissue (total)
|
67,130
|
68
|
34,777
|
60
|
|
a) Low back
|
30,097
|
31
|
22,630
|
39
|
|
b) Neck/Shoulders
|
14,623
|
15
|
2,759
|
5
|
|
c) Other
|
22,410
|
23
|
9,388
|
16
|
|
XIV Congenital malformations, deformations, and chromosomal abnormalities
|
39
|
< 1
|
–
|
< 1
|
|
XV Certain conditions originating in the perinatal period
|
0
|
–
|
0
|
–
|
|
XVI Symptoms, signs, and abnormal clinical and laboratory findings not elsewhere classified
|
2,367
|
2
|
2,683
|
5
|
|
XVII Injury, poisoning, and certain other consequences of external causes
|
2,738
|
3
|
4,505
|
8
|
|
XVIII Factors influencing health status and other contacts with health services
|
192
|
< 1
|
15
|
< 1
|
|
Total
|
98,008
|
100
|
57,756
|
100
|
In the second stage of the analysis, the sick-leave diagnoses were assigned to one of the following 5 groups: low back, neck or shoulder, all other musculoskeletal, psychiatric, and all other diagnoses. The analyses applied to the cohort in its entirety or stratified by sex or whether disability pension was granted during the follow-up period. Differences between groups (e.g. with respect to sex) were evaluated using the χ2 test, and, when appropriate, Fisher’s exact test. A p-value < 0.05 was regarded as statistically significant. SAS and SPSS statistical software were used for calculations.
The study was approved by the Swedish National Data Inspection Board and the local committee for research ethics.
Sickness insurance in Sweden 1982–96
In 1985–96, all residents over the age of 16 years who had an annual income from employment of > 6000 SEK (650 € in 2004) or were students or registered as unemployed had the right to claim economic compensation from sickness insurance when unable to work due to illness or injury. Degree of work capacity was determined in relation to the particular work demands of employees, or to jobs available on the labour market when considering those who were unemployed. Self-certification was accepted for the first 7 days, and thereafter a sickness certificate from a physician was required. There was no limit for the duration of a spell of sick-leave, e.g. it could last for more than one year.
Some changes in the sickness insurance scheme occurred over the study period: during the years 1985–87 and 1991–96, the first day of a sick-leave period was a waiting day when no benefits were paid. From 1 January 1992, compensation was paid by the employer for the first 14 days of sickness absence. Spells < 14 days, were therefore not registered at the Social Insurance Offices and not included in the study.
The sickness benefits amounted to 75–100% of lost income. Full- or part-time temporary (1–3 years) or permanent disability pension (called incapacity benefit in the UK and social security disability insurance in the USA) could be granted before the age of 65 years and covered at least 65% of lost income. There was also generous parental insurance covering absence from work for the care of newborn or sick children, but data on this type of absence were not included in the study.
RESULTS
During the 11-year follow-up of the cohort of young adults included in this study, 22% (n = 46) were granted disability pension (a majority after 1991), 7 emigrated, and 2 died (one of whom was in receipt of disability pension). More women than men were granted disability pension (26% and 14%, respectively), p = 0.041 (13).
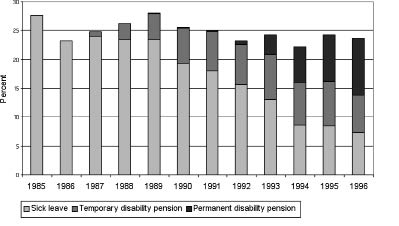
In all, the 213 cohort members had 155,763 sick-leave days that were included in 7875 sick-leave periods and in 4609 spells of sick-leave. Also, during the follow-up a decrease in number of sick-leave days concurred with an increase in number of days in receipt of disability pension (Fig. 1). Over the 11 years, the subjects were sickness absent or were receiving disability pension for approximately 25% of all days that were at risk for such compensation (Fig. 1). In 1996, most of the days with benefits (71%) represented disability pension.
Fig. 1. Days on sick-leave or disability pension (temporary or permanent) calculated as the percentage of days at risk for such compensation in a cohort of 213 persons followed over 11 years.
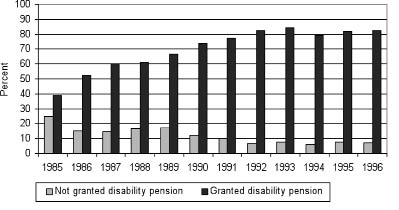
When the cohort was separated into 2 groups according to whether or not they had been granted disability pension during the follow-up period, a notable difference emerged between the 2 groups as early as 1985–86 regarding the number of days with sickness compensation; that is, at a point in time before any of the cohort members had been granted disability pension (Fig. 2). In 1996, those in the disability pension group were on sick-leave or receiving disability pension for 80% of all days at risk, whereas the corresponding rate was 12% for those in the non-disability-pension group (p < 0.001).
Fig. 2. Days on sick-leave and disability pension calculated as percentage of days at risk for such compensation in a cohort of 213 people followed over 11 years. The cohort is stratified by whether disability pension was (n = 46) or was not (n = 167) granted during the follow-up period.
Seventeen of the 18 ICD-based diagnostic categories were represented in the cohort; the only exception was the diagnostic group called “certain conditions originating in the perinatal period”, e.g. a diagnosis not relevant for the participants (Table I). Over the 11 years, musculoskeletal diagnoses were most common, constituting 68% and 60% of all sick-leave days for women and men, respectively. In the musculoskeletal group, neck/shoulder or other musculoskeletal diagnoses were more common among women, whereas men were more often on sick-leave due to low-back disorders. Psychiatric diagnoses were found to underlie 15% of the sick-leave days for men (mainly depression) but only 6% of the days for women.
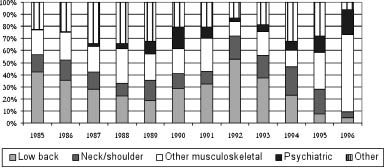
Considering women, closer analysis of sickness absence with musculoskeletal and psychiatric diagnoses showed that, in 1985, 57% of the total number of sick-leave days was due to the including diagnoses of low back or neck/shoulder disorders (Fig. 3). The proportions of the diagnostic groups changed over the years, with a decrease in low back and neck/shoulder diagnoses and an increase in other musculoskeletal diagnoses and psychiatric diagnoses. In 1996, 20% of the sick-leave days were due to psychiatric diagnoses.
Fig. 3. Sick-leave days in 5 diagnostic groups in 1985–96 among 129 women initially sick-listed due to back diagnoses. Results calculated as percent of all sick-leave days.
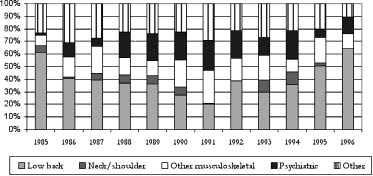
The pattern of the changes in diagnoses was similar for men (Fig. 4), in whom the including diagnoses represented 68% of the sick-leave days after inclusion in 1985. Furthermore, low-back diagnoses were more common among men, not only in 1985, but during the entire follow-up period.
Fig. 4. Sick-leave days in 5 diagnostic groups in 1985–96 among 84 men initially sick-listed due to back diagnoses. Results calculated as percentage of all sick-leave days.
DISCUSSION
This study was an attempt to describe the prognosis of sickness absence in terms of future general and diagnosis-specific sick-leave and/or disability pension in a cohort of young adults initially sick-listed due to back, neck, or shoulder diagnoses. As early as in the 2 first years of the 11-year follow-up, there was a notable difference in the number of sick-leave days between those who were and those who were not granted disability pension later during the study period. For the latter group, the number of sick-leave days decreased during the 11 years. Interestingly, the diagnostic panorama proved to be much wider than expected: 17 of the 18 ICD-8 diagnostic groups were represented on the cohort’s sickness certificates over the 11 years. Obtaining information on the prognosis of sickness absence should facilitate the selection of individuals for suitable interventions and rehabilitation measures, which should be particularly helpful when managing cases involving young adults.
Methodological considerations
The study has several strengths, such as a long follow-up, a very large number of periods of sick-leave (8000), very good quality of sick-leave and disability pension data, and no persons lost to follow-up. Due to the population-based approach, all residents with the type of sickness absence of interest were included in the study, and there was no bias with regard to type of workplace, occupation, or clinic, as is often the case in investigations examining sickness absence both in general and in relation to specific diagnoses (2, 13, 22–26). Linköping has been considered representative of many Swedish cities (13), but the results cannot be generalized to other age groups or sick-leave diagnoses. The fairly small size of the cohort was a limitation, although the group was large enough to achieve the goal of the study, considering the extensive number of included sick-leave data.
The type of analyses conducted in this study requires detailed information about diagnoses for each sick-leave period. Such detailed information is not usually available and, furthermore, in most other studies only the first diagnosis for the first period in a spell of sick-leave (13, 27) or the last diagnoses in the last sick-leave period (28) are obtainable. Data on incidence, occurrence, duration, and grade of sick-leave and disability pension were obtained from registers kept by the Social Insurance Offices, which can be regarded as highly accurate and valid sources. Data on diagnoses were retrieved manually from the sickness certificates by one of the researchers in the group. For subjects who moved to other regions during the study period, great effort was made to find all certificates at the insurance offices in the new home areas and to identify the diagnoses they contained. This task was very time-consuming, and this factor contributed to the uniqueness of our database. The validity of the diagnoses on sickness certificates has been discussed (2), but has been tested and found to be acceptable (20). The validity of more stigmatizing diagnoses, such as psychiatric illnesses, is probably greater compared with other diagnoses; in other words, people with psychiatric diagnoses are more likely actually to have such disorders (2, 29).
In the present study, even though 21% of the certificates listed more than one diagnosis, only the first diagnosis was used in the analyses. The first diagnosis is intended to represent the main reason for reduced work capacity, although it may be difficult to ascertain which is the most important in cases of comorbidity. It is plausible that physicians tend not to change the first diagnosis if other diagnoses are also found to be applicable when prolonging certification of a spell of sick-leave. This is a possible minor source of bias in our data, which might have led to underestimation of the variation in the diagnostic panorama. Moreover, diagnoses that are primarily associated with shorter spells of sick-leave may have been underestimated after 1992, since spells of sick-leave < 14 days were not included for employees after that time. However, this non-inclusion was the same for all members of the cohort, and hence it cannot explain the gender differences.
Results
Sickness certification is a common healthcare measure in the Western world today, but there is limited knowledge about when it is appropriate to apply this measure or regarding associated prognoses in terms of future sickness absence or disability pension (7, 30, 31). The purpose of sick-leave benefits is to provide economic and social security for anyone who is unable to work due to disease or injury. Notwithstanding, long-term sickness absence may have negative side-effects, such as passivity, disease, adverse lifestyles, isolation, and marginalization in the labour market (32–35).
The present results agree with the findings of earlier studies of the same cohort, where we inter alia concluded that the risk of receiving disability pension was more than 9 times greater for those who had had a spell of sick-leave > 90 days (regardless of diagnosis) than for those who had not had such a spell of sick-leave during the past 2 years in the follow-up period (36). For the majority of subjects (78%) the main reason for disability pension was musculoskeletal diagnoses, for 17% psychiatric diagnoses, and only 4% was due to other diagnoses.
During recent decades several countries have seen an increase in work absenteeism due to psychiatric disorders (4). Additional studies are required to determine whether the increase in such diagnoses in our cohort was due to this general change in the panorama of sick-leave and disability pension diagnoses, or whether this is a phenomenon often found among persons initially sick-listed with back, neck, or shoulder diagnoses. As there are very few diagnoses-specific studies following persons on sickness absence over time, it is too early to draw any conclusions. However, a recent study of persons long-term sickness absent (> 90 days) with psychiatric disorders showed that they had not had long sickness absences in previous years (37).
During the first 2 years of follow-up there was already a marked difference in the number of sick-leave days between those who were later granted disability pension and those who were not. This is remarkable, since a majority of the pensions were granted after 1991. To our knowledge, such an observation has not been reported previously. Such information might facilitate decisions regarding whether individuals are in need of rehabilitation measures or if they are likely to return to work anyway. This is a crucial matter in all judgements related to rehabilitation (38), i.e. the decision as to which individuals to direct further rehabilitation measures.
There are several plausible explanations for the present observation of a high rate of sickness absence due to psychiatric diagnoses. Perhaps some of the subjects already had psychiatric disorders at the time of inclusion but were reluctant to mention that fact to the physician. Moreover, the back disorders underlying the spell of sick-leave used as inclusion criteria might actually have been symptoms of depression or substance abuse. In addition, the long-term sickness absence per se might have led to isolation, anxiety, and/or depression (32–34) or abuse of alcohol and other substances resulting in a need for further sick-leave (39). It is noteworthy that such a large proportion of the sick-leave days was due to psychiatric diagnoses. This indicates that healthcare providers should consider discussing mental problems and factors such as alcohol consumption at an early stage in treatment, especially for male patients.
The actual ill-health content of the sickness absence related to back pain is often questioned. However, recent studies (35, 40) have shown highly elevated mortality rates among people in receipt of disability pension, even though the main diagnoses behind both such retirement and sickness absence, namely, musculoskeletal disorders, are seldom a cause of death. Our study also indicates a complex ill-health panorama among several persons with such absences.
In conclusion, this cohort of young adults initially sick-listed due to back, neck, or shoulder diagnoses also had, over this 11-year follow-up, a high level of sickness absence with other diagnoses. Even after the first year of the study period, there was a considerable difference in the level of sickness absence between those who were and those who were not later granted disability pension. This knowledge is valuable in a clinical context, since it can be used to aid decisions regarding the use of rehabilitation measures. More knowledge early in the process is warranted to be able to identify those who do not need rehabilitation measures. Over the 11-year period, the number of sick-leave days due to musculoskeletal diagnoses decreased in relation to psychiatric and other diagnoses, which suggests that healthcare providers should consider discussing mental problems and factors such as alcohol consumption early in their dealings with patients who are on sick-leave due to back problems.
REFERENCES