Robert W. Motl, PhD and Edward McAuley, PhD
From the Department of Kinesiology and Community Health, University of Illinois at Urbana-Champaign, Urbana, IL, USA
Robert W. Motl, PhD and Edward McAuley, PhD
From the Department of Kinesiology and Community Health, University of Illinois at Urbana-Champaign, Urbana, IL, USA
OBJECTIVE: This study examined change in physical activity as a behavioral correlate of short-term disability progression in persons with multiple sclerosis over a 6-month period.
DESIGN: Panel design.
SUBJECTS: The sample included 292 persons with multiple sclerosis.
METHODS: Participants wore an accelerometer for 7 days as a measure of physical activity and then provided demographics and clinical information and completed the Patient Determined Disease Steps scale as a measure of disability. After a 6-month period, participants provided information about the occurrence of a relapse in the previous 6 months and again wore an accelerometer for 7 days and completed the Patient Determined Disease Steps scale.
RESULTS: Panel analysis indicated associations between baseline physical activity and disability (path coefficient = −0.41, p < 0.001) and 6-month change in physical activity and disability progression (path coefficient = −0.09, p = 0.025).
CONCLUSION: Such findings provide preliminary support for a reduction in physical activity as a behavioral correlate, but not necessarily cause, of short-term disability progression in persons with multiple sclerosis.
Key words: mobility; neurological disease; rehabilitation.
J Rehabil Med 2011; 43: 305–310
Correspondence address: Robert W. Motl, Department of Kinesiology and Community Health, University of Illinois, 350 Freer Hall, Urbana, IL 61801, USA. E-mail: robmotl@uiuc.edu
Submitted May 11, 2010; accepted December 21, 2010
Multiple sclerosis (MS) is the most prevalent non-traumatic disabling neurologic disease among young adults worldwide (1). MS typically begins with intermittent bursts of focal inflammation in the central nervous system (CNS) (2) and results in the demyelination and transection of axons in the brain, optic nerves and spinal cord (3). The resulting demyelination and transection of axons leads to conduction delay and conduction block of electrical potentials along axonal pathways in the CNS (4). This interference with neuronal conduction is associated with the accumulation of impairment and disability over time in people with MS.
Natural history studies have provided evidence for the rate and predictors of disability progression in persons with MS (5, 6). For example, nearly 50% of individuals will require the use of an aid for walking (i.e. reach an Expanded Disability Status Scale (EDSS) score of 6.0) within 15–25 years after the onset of MS (5–8). Approximately 50% of individuals will have even more severe functional limitations and irreversible disability (i.e. reach an EDSS score of 7.0) within 30 years after the onset of MS (6). Common predictors of disability progression include sex, age at MS onset, clinical MS course, and occurrence of a relapse (7–10).
Researchers have just begun considering physical activity as a behavioral correlate of disability progression in persons with MS (11) using cross-sectional research designs and small sample sizes (12–14). For example, there was a moderate, negative correlation between accelerometer counts and EDSS scores (r = –0.37) in a sample of 30 individuals with MS (13). Another study reported a strong, negative correlation between accelerometer counts and EDSS scores (r = −0.64) among 27 persons with MS (12). One final study reported a strong, negative correlation between accelerometer and EDSS scores (r = –0.60) in a sample of 80 persons with MS (14). Importantly, the functional dynamics of the association between changes in variables can only be inferred from cross-sectional analyses involving a single point in time. There is a requisite need for additional evidence from longitudinal designs that supports the association between changes in physical activity and disability progression over time. This is a logical precursor before developing and testing interventions using a randomized controlled trial design for increasing physical activity as a behavioral approach for reducing disability progression in persons with MS. This can be accomplished using a panel design. Panel designs involve the collection of observations or data at more than one point in time using the same persons, and this design allows for studying the dynamics of relationship changes over time.
Building upon previous research, the present study involved a longitudinal research design and an examination of physical activity as a behavioral correlate of the short-term progression of disability over a 6-month period in a large sample of individuals with MS. We hypothesized that change in physical activity would be negatively associated with change in disability over time while controlling for sex, clinical MS course, age of MS onset, and occurrence of a relapse as confounding variables.
MethodS
Participants
This panel study was part of an investigation of mediators of the association between physical activity and quality of life over time in persons with MS, and we have previously described the recruitment, inclusion criteria, and baseline characteristics of the sample (15). Briefly, there were 292 individuals with MS who provided baseline data and 276 of those individuals provided follow-up data 6-months later (95% of total sample). The 5% attrition at follow-up involved a change in residential addresses.
Measures
Demographic and clinical variables. Demographic (i.e. sex, marital status, age, employment, race, education, income) and clinical (clinical MS course, age of MS onset) information were collected using a questionnaire designed specifically for this project. The clinical diagnostic information was confirmed using a form-letter that was completed by each participant’s neurologist.
Physical activity. Physical activity was measured by ActiGraph single-axis accelerometers (model 7164, Manufacturing Technology Incorporated, Fort Walton Beach, FL, USA). This accelerometer contains a single, vertical axis piezoelectric bender element that generates an electrical signal proportional to the force acting on it. The acceleration/deceleration signal is digitized by an analog-to-digital converter and numerically integrated over a pre-programmed epoch interval. At the end of each interval, the integrated value of movement counts is stored in random access memory and the integrator is reset. The monitor is programmed for start time and data collection interval, and data are retrieved for analysis via a personal computer interface and software provided with the unit. The downloaded data from the accelerometers are then entered into Microsoft Excel for data processing. In this study, the epoch was 1 min, and the accelerometers were worn during the waking hours, except while showering, bathing, and swimming, for a 7-day period. Waking hours was defined as the moment upon getting out of bed in the morning through the moment of getting into bed in the evening. The accelerometers were not worn during the night while the participants slept. The participants were informed that the accelerometers measured physical activity, and recorded the time that the accelerometer was worn on a log, and this was verified by inspection of the min-by-min accelerometer data. Regarding data processing, we summed the minute-by-minute counts over each of the 7 days and then averaged the total daily movement counts over the 7 days. This yielded accelerometer data in total movement counts per day with higher scores representing more physical activity. We have used the same accelerometer and procedures in our previous research on validity of physical activity measures in persons with MS. Accelerometer activity counts over a 7-day period have been associated with scores from interview (r = 0.75), self-report (r = 0.52), and objective (r = 0.93) measures of physical activity in MS (13, 16).
Disability. Disability was measured using the Patient Determined Disease Steps (PDDS) scale (17). The PDDS is a self-report questionnaire that contains a single item for measuring self-reported disability using an 8-level ordinal scale. The verbal description for 0 was Normal, described as “I may have some mild symptoms, mostly sensory due to MS but they do not limit my activity. If I do have an attack, I return to normal when the attack has passed”. The verbal description for 4 was Early Cane, described as “I use a cane or a single crutch or some other form of support (such as touching a wall or leaning on someone’s arm) for walking all the time or part of the time, especially when walking outside. I think I can walk 25 feet in 20 seconds without a cane or crutch. I always need some assistance (cane or crutch) if I want to walk as far as 3 blocks”. The verbal description for 8 was Bedridden, described as “Unable to sit in a wheelchair for more than 1 hour”. This scale was developed as an inexpensive surrogate for the EDSS and scores from the PDDS are linearly and strongly related with physician-administered EDSS scores (r = 0.93) (17) thereby providing evidence for the validity of this scale as a measure of disability. Additional validity evidence is based on the correlation between PDDS scores and oxygen cost of treadmill and over-ground walking (range of r = 0.53 and 0.65) and Multiple Sclerosis Walking Scale-12 scores (r’s = 0.81 and 0.91) in previous research involving persons with MS (18).
Procedure
The procedure was approved by an Institutional Review Board and all participants signed an informed consent document. The study materials included a battery of questionnaires and an accelerometer, and the materials were sent to all participants through the US postal service, along with a pre-stamped and pre-addressed envelope for return postal service. The participants were instructed to wear the accelerometer during waking hours, except while bathing, showering, or swimming, for 7 days and then completed the battery of questionnaires on the eighth day. The same assessment procedures were completed at baseline and 6-months later at follow-up. Immediately before the follow-up assessment, participants provided information over the telephone about the occurrence of a relapse during the preceding 6-month period that was confirmed and treated with intravenous steroids by a neurologist. Participants received $40 remuneration, which was prorated for each assessment period.
Data analysis
We initially performed descriptive (means, medians, standard deviations, and/or ranges), distributional (skewness and kurtosis) and inferential (i.e. paired samples t-tests) analyses in SPSS, version 18.0 for Windows. The data were then analyzed using panel analysis with manifest variables and covariance structure modeling with the Full-Information Maximum Likelihood (FIML) estimation in AMOS 16.0. Panel analysis is a useful analytic procedure for testing hypothetical relationships involving change in manifest variables over time (19). Covariance structure modeling is a family of techniques that allow for testing the fit of hypothetical models that describe relationships among manifest or latent variables. The FIML estimator was selected because there were missing data and this estimator is an optimal method for the treatment of missing data in covariance modeling that has yielded accurate fit indices with simulated missing data (20). There were 4% and 9% of missing accelerometer data for baseline and follow-up, respectively. There were 5% missing PDDS data for follow-up, but 0% for baseline.
The first panel model that we tested is provided in Fig. 1. This model included: (i) stability path coefficients between baseline and follow-up for physical activity and disability; (ii) path coefficients between physical activity and disability at both baseline and follow-up; and (iii) cross-lagged path coefficients between physical activity at baseline and disability at follow-up and vice versa. Importantly, path coefficients are standardized linear regression weights that indicate the magnitude of a relationship between two manifest variables and, by extension, the amount of expected change in one variable that is associated with a standardized unit change in another variable. The stability coefficient for baseline and follow-up physical activity or disability, when imperfect (i.e. less than a maximum of 1.0), can be interpreted in terms of a change in the rank ordering of persons on those variables over time and this allows for the study of change in the follow-up variables (19). The path coefficient between physical activity and disability for follow-up, in particular, can be interpreted in terms of the association between change in physical activity and residual change in disability over time (18). The cross-lagged path coefficient between baseline physical activity and follow-up disability can be interpreted, for example, as the change in disability over time that is associated with initial levels of physical activity. The second panel model included that aforementioned parameterization plus: (i) path coefficients between sex, clinical MS course (relapsing-remitting vs progressive MS), and age of MS onset with physical activity and disability manifest variables for both baseline and follow-up; and (ii) associations between the occurrence of a relapse and disability for both baseline and follow-up. We did not include paths between physical activity and occurrence of a relapse based on a literature review demonstrating no evidence of an association (21). This model provided an indication of the cross-sectional and longitudinal associations between physical activity and disability controlling for sex, type of MS, age of MS onset, and occurrence of a relapse as confounding variables; this is important for indicating that any association between physical activity and disability is not merely a common manifestation of MS-disease activity. Model fit was assessed using the χ2, root mean-square error of approximation (RMSEA), and comparative fit index (CFI). We based an excellent model-data fit on a non-significant χ2 value and combinatory rules of RMSEA ≤ 0.06 and CFI ≥ 0.95 (22).
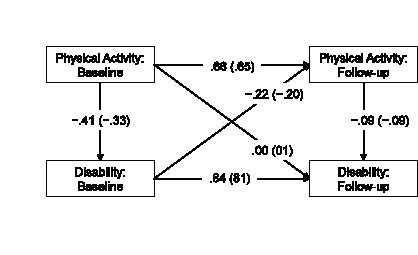
Fig. 1. Panel model of relationships among physical activity and short-term disability over time tested in individuals with multiple sclerosis. Note: All path coefficients in the figure are standardized estimates, and the values in parentheses are path coefficients controlling for sex, age of multiple sclerosis (MS) onset, MS type, and occurrence of a relapse. Physical activity was measured by an accelerometer and disability was measured by Patient-Determined Disease Steps scale. The follow-up variables reflect residual changes in physical activity and disability over time.
Results
Descriptive statistics
The sample consisted of 245 women and 47 men (~5:1 ratio of women to men), and 246 were diagnosed with relapsing-remitting MS and the remaining 46 were diagnosed with primary progressive or secondary progressive MS. The lower number of men vs women is generally consistent with the higher prevalence of MS in women (10). The mean age of MS onset was 37.7 years (standard deviation (SD) 10.1, range 14–60 years) and the mean duration, defined as time since definite diagnosis, of MS was 10.3 years (SD 7.9, range 1–35 years). Of the 292 participants, 28 individuals (i.e. 10% of the sample) reported occurrence of a relapse during the 6-month follow-up period.
Descriptive statistics for physical activity and disability over time are provided in Table I. Paired t-tests indicated that there was a statistically significant and small reduction in accelerometer counts over time, but there was no statistically significant change in PDDS scores over the 6-month period. We further examined the distribution of cases that improved, worsened, or remained stable based on a 1 or more point change on the PDDS scale over the 6-month time period. The adoption of a 1 or more point change in PDDS scores is consistent with the operational definition used in previous research for examining the effect of relapses on residual deficits in EDSS scores among persons with MS (9). We further note that the PDDS is a surrogate measure that is strongly associated with the EDSS. There were 169 persons who remained stable, 56 who progressed or worsened, and 49 who regressed or improved over time. The skewness and kurtosis estimates did not identify any major departures from a normal distribution for accelerometer or PDDS variables; this is an important assumption for the application of linear panel analysis.
| Table I. Descriptive statistics and changes over time for the measures in the panel analysis | ||||
| Variable | Baseline | 6-month follow-up | t | p |
| Accelerometer Mean (SD) Median (quartiles) | 220,006 (121,252) 200,768 (143,900–266,111) | 206,834 (104,781) 200,768 (134,250–261,662) | 3.56 | 0.001 |
| PDDS Mean (SD) Median (quartiles) | 2.3 (1.8) 3 (1–4) | 2.3 (1.7) 3 (1–4) | 0.34 | 0.72 |
| PDDS: Patient-Determined Disease Steps scale. | ||||
Model 1: Association between change in physical activity and disability over time
The first panel model was saturated and represented a perfect fit for the data (χ2 = 0, df = 0). The path coefficients from the panel model are provided in Fig. 1. The stability coefficients for physical activity (path coefficient = 0.66, p < 0.001) and disability (path coefficient = 0.84, p < 0.001) were imperfect (i.e. less than a maximum of 1.0) and indicated a change in the rank ordering of individuals over time (19). The path coefficients between physical activity and disability were statistically significant for baseline (path coefficient = −0.41, p < 0.001) and follow-up (path coefficient = −0.09, p = 0.025). The path coefficient for follow-up indicated that change in physical activity was associated with a residual change in disability over time. The path coefficient between baseline disability and follow-up physical activity was statistically significant (path coefficient = −0.22, p < 0.001), but the path coefficient between baseline physical activity and follow-up disability was not statistically significant (path coefficient = 0.00, p = 0.49). This indicated that those with higher disability had a greater reduction in physical activity over the 6-month period, but baseline physical activity did not predict a change in disability. We further tested this interpretation by removing the cross-lagged path between baseline physical activity and follow-up disability and the panel model still represented a excellent fit for the data (χ2 = 0.01, df = 1, p = 0.97, RMSEA=0.01, CFI = 1.00) and none of the remaining path coefficients changed in magnitude or direction. The scatter plot along with line of best fit and 95% confidence interval for the association between changes in physical activity and disability status is shown in Fig. 2.
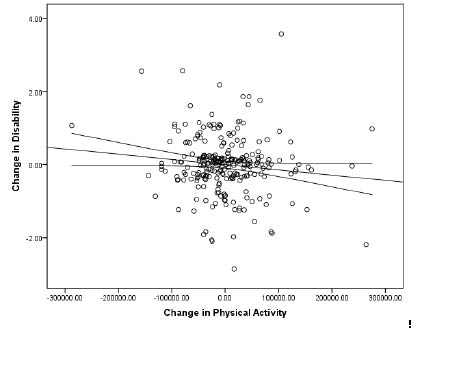
Fig. 2. Scatter plot along with line of best fit and 95% confidence interval for the association between changes in physical activity and disability.
Model 2: Association between change in physical activity and disability over time controlling for demographic and clinical variables as confounders
The second panel model controlled for confounding variables and represented an excellent fit for the data (χ2 = 4.78, df = 9, p = 0.85, RMSEA = 0.00, CFI=1.00). The path coefficients from the first panel model were generally unchanged in significance and magnitude when controlling for sex, age of MS onset, clinical MS course (relapsing vs progressive), and occurrence of a relapse as confounding variables and are provided in parentheses along with the original coefficients in Fig. 1. Regarding the demographic and clinical variables, age of MS onset was associated with baseline, but not follow-up, physical activity (path coefficient = −0.22, p < 0.001) and disability (path coefficient = 0.09, p = 0.05); clinical MS course was associated with baseline, but not follow-up, physical activity (path coefficient = −0.20, p < 0.001) and disability (path coefficient = 0.30, p < 0.001); and occurrence of a relapse was associated with baseline disability (path coefficient = 0.13, p = 0.025) and follow-up disability (path coefficient = 0.07, p = 0.01). Those with later age of MS onset and progressive MS had lower baseline physical activity and higher baseline disability levels, whereas those with higher baseline disability had a relapse during the follow-up period and those who had a relapse had an increase in disability over time. The importance of this analysis, in particular the inclusion of relapse occurrence as a confounding variable, is that it provides evidence that physical activity and disability are inter-related beyond the possibility of being common manifestations of MS-disease activity.
Discussion
Researchers have recently highlighted the possible role of physical activity as a behavioral correlate of disability progression in persons with MS (11), and previous cross-sectional research has demonstrated an inverse association between physical activity and disability in this population (12–14). Such observations provided the basis for this longitudinal examination of change in physical activity as a behavior correlate of short-term change in disability over time in a large sample of persons with MS. We reported that change in physical activity was associated with a residual change in disability over time, such that those who decreased physical activity reported an increase in disability level. This association was unaffected by controlling for other demographic and clinical predictors of disability progression, and was similar in magnitude, but still weak, when compared with that of the occurrence of a relapse. Such findings provide preliminary support for a reduction in physical activity as a meaningful behavioral correlate of short-term disability progression in persons with MS. The outcomes of this study do not establish evidence of causality, but rather might “set the stage” for randomized controlled clinical trials that examine physical activity as a behavioral modality for altering the trajectory of disability progression over time in individuals with MS, perhaps even among those who have reached a benchmark of cumulative disability. This latter group is particularly important as the trajectory of irreversible disability after reaching a benchmark EDSS score of 4.0 is not predicted by demographic and clinical variables (6), and most disease modifying agents have shown limited efficacy in slowing eventual disease progression in persons with MS (2, 6). Overall, we emphasize that our results do not establish causality, but do provide a preliminary scientific basis for randomized controlled clinical trials that examine physical activity as a behavioral modality for slowing the eventual progression of disability in individuals with MS.
The primary objective of our research involved an examination of change in physical activity behavior as a correlate of short-term disability progression, but 3 additional findings warrant discussion. One finding was that of a cross-lagged association between baseline disability and change in physical activity over time. The cross-lagged associated indicated that those with higher baseline disability had a greater reduction in physical activity over the 6-month period. This finding highlights the importance of developing and delivering interventions for maintaining and promoting physical activity among individuals with higher levels of disability. The second finding was that of no apparent association between baseline physical activity and change in disability over time. The zero-order association indicated that those with higher baseline physical activity did not have either a smaller or a larger increase in disability over the 6-month period. Such an observation would indicate that more physically active persons with MS are not prone to a subsequent increase or decrease in the rate of accumulative disability over time and this would neither argue against nor for the value of physical activity in MS. The third finding was that of an association between the occurrence of a relapse predicting follow-up disability (path coefficient = 0.07) such that those who had a relapse reported an increase in disability. The prediction of change in disability by the occurrence of a relapse is consistent with previous research (9). That research indicated that 42% and 28% of patients who had an exacerbation had residual deficits of ≥ 0.5 and 1.0 EDSS units, respectively, at an average of 64 days after the exacerbation (9). Although we did not assess degree and time course of disability after the occurrence of a relapse, we note that our results are consistent with the observation that exacerbations produce a measureable effect on disability. Such an observation is particularly important because it provides some meaning for our examination of physical activity as a correlate of short-term disability progression in that we observed similarly sized associations between both physical activity and occurrence of a relapse with disability progression.
This study did not examine mechanisms for physical activity as a behavioral correlate of disability progression because the design does not allow for causality, but we believe that some speculation on the possible mechanism might be warranted. Physical activity might be associated with a slower rate of disability progression through its beneficial effects on immune dysregulation, neurodegenerative processes (i.e. active pathology), and physiological function. Physical activity might influence concentrations of pro- and anti-inflammatory cytokines in a manner that alters the immune dysregulation associated with MS (23). Physical activity might further promote alterations in neurotrophic factors, such as IGF-I, BDNF, and NGF, that attenuate CNS vulnerability to neuronal degeneration in MS (24). Physical activity might alter physiological function in a manner that attenuates the progression of disability over time in MS (25). The potential beneficial effects of physical activity on immune dysregulation, neurodegenerative processes, and physiological function might provide a biological basis for a slower progression of disability in MS.
There are obvious limitations of our study. The first limitation is that of a relatively short, 6-month period of follow-up. We recognize that larger and more meaningful changes in disability would be observed over a longer period of observation and that the question addressed in this paper was the consequence of a secondary outcome of our primary study purpose, namely an examination of mediators of the association between physical activity and changes in quality of life. An additional limitation is that our design would not allow for an examination of causality among study variables over time. This can only be accomplished in the context of a randomized controlled trial that manipulates physical activity and examines the resulting effect on disability progression. Another limitation is that our sample had a relatively low level of disability based on the median baseline PDDS score of 3.0. This score is associated with gait disability and corresponds with an EDSS score of approximately 4.0 (onset of gait impairment). This is largely the result of one of our inclusion criteria involving independent ambulation (i.e. walking with minimal assistance) based on previous validity evidence for the accelerometer as a measure of physical activity. Accordingly, we limit our observations among a relatively intact group of individuals with MS and over a relatively brief period of time, and recognize that future research should be conducted that addresses both issues. The last limitation is that our sample, particularly based on the distribution of sex, might not be representative of the general population of persons with MS (10).
Collectively, our results provide a preliminary basis for physical activity as a behavioral correlate of disability progression over a 6-month period among persons with minimal disability, and we highlight the importance of continued investigation of the clinical value of physical activity in forestalling disability progression over time in persons with MS using a randomized controlled clinical trial. Such examinations will ultimately address the possible role of physical activity as a meaningful and important therapeutic agent in the prevention of disability progression in persons with MS (11).
Acknowledgement
Funded by the National Institute of Neurological Diseases and Stroke (NS054050).
References

