Marie R. Mouawad, BMedSc (Hons), Catherine G. Doust, BMedSc (Hons), Madeleine D. Max, BMedSc (Hons) and Penelope A. McNulty, PhD
From Neuroscience Research Australia and University of New South Wales, Sydney, Australia
Marie R. Mouawad, BMedSc (Hons), Catherine G. Doust, BMedSc (Hons), Madeleine D. Max, BMedSc (Hons) and Penelope A. McNulty, PhD
From Neuroscience Research Australia and University of New South Wales, Sydney, Australia
BACKGROUND: Virtual-reality is increasingly used to improve rehabilitation outcomes. The Nintendo Wii offers an inexpensive alternative to more complex systems.
OBJECTIVE: To investigate the efficacy of Wii-based therapy for post-stroke rehabilitation.
METHODS: Seven patients (5 men, 2 women, aged 42–83 years; 1–38 months post-stroke, mean 15.3 months) and 5 healthy controls (3 men, 2 women, aged 41–71 years) undertook 1 h of therapy on 10 consecutive weekdays. Patients progressively increased home practice to 3 h per day.
RESULTS: Functional ability improved for every patient. The mean performance time significantly decreased per Wolf Motor Function Test task, from 3.2 to 2.8 s, and Fugl-Meyer Assessment scores increased from 42.3 to 47.3. Upper extremity range-of-motion increased by 20.1º and 14.33º for passive and active movements, respectively. Mean Motor Activity Log (Quality of Movement scale) scores increased from 63.2 to 87.5, reflecting a transfer of functional recovery to everyday activities. Balance and dexterity did not improve significantly. No significant change was seen in any of these measures for healthy controls, despite improved skill levels for Wii games.
CONCLUSION: An intensive 2-week protocol resulted in significant and clinically relevant improvements in functional motor ability post-stroke. These gains translated to improvement in activities of daily living.
Key words: stroke rehabilitation; upper limb; motor control; functional ability; hemiplegia; virtual reality.
J Rehabil Med 2011; 43: 527–533
Correspondence address: Penelope McNulty, Neuroscience Research Australia, Barker Street, Randwick NSW 2031 Australia. E-mail: p.mcnulty@neura.edu.au
Submitted June 3, 2010; accepted March 17, 2011
INTRODUCTION
Stroke is the fifth largest cause of disability in the world (1) and the second largest in Australia (2). Because there is no cure, the only means of promoting functional recovery is through rehabilitation, but there is no standard protocol for post-stroke treatment. While constraint-induced movement therapy is the best-codified and internationally most successful treatment for upper limb dysfunction after stroke (3–5), concerns remain about patient safety and satisfaction (6, 7). Dissatisfaction with traditional methods of rehabilitation has led to a growing use of virtual reality therapy, both immersive systems that involve the whole body in the synthetic world by means of devices such as head-mounted displays (8), and non-immersive systems that engage only a single limb or sensory modality (9). Non-immersive systems create less sense of “presence” than immersive systems, but they are cheaper, easier to use and may cause less “cyber-sickness” (10, 11).
Virtual reality, whether immersive or non-immersive, has the potential to create stimulating and fun environments and develop a range of skills and task-based techniques to sustain participant interest and motivation (11, 12). This not only results in better movement outcomes for rehabilitation purposes, but helps to minimize the problems with compliance encountered with more traditional therapy strategies (6, 13). However, the equipment used in most virtual reality studies to date is complex, expensive and requires specialist facilities and staff (8, 14). It is therefore debatable whether this type of therapy is feasible for rehabilitation in the wider community.
The Nintendo Wii offers a simple and affordable mode of virtual reality therapy that is being used increasingly in stroke and rehabilitation units worldwide, but to date few studies of its efficacy have been published. A recent study in this journal suggested that the Nintendo Wii is a feasible adjunct to traditional therapy in moderately disabled subacute stroke patients (15). The present study extends this work into the chronic period post-stroke, demonstrating a greater range of functional improvements, including both active and passive upper limb joint range-of-motion, and a transfer of therapy gains into activities of daily living.
METHODS
Subjects
Seven consecutively screened stroke patients were recruited into the study (Table I), mean age 65.3 years (standard deviation (SD) 14.6) and mean 15.3 months (SD 12.6) post-stroke. Patients were recruited through the rehabilitation units of the Prince of Wales and St Vincent’s Hospitals, Sydney. Inclusion criteria were: (i) hemiparetic with upper limb dysfunction following a single unilateral stroke in the territory of the middle cerebral artery; (ii) ≥10º voluntary flexion movement on the more-affected side in the thumb, elbow and shoulder; (iii) ability to communicate; (iv) a carer available for the study duration; and (v) cognitively competent (≥ 24 Mini-Mental State Examination (16)), the cognitive competency of the patient with expressive aphasia was verified by physicians. Exclusion criteria were: (i) engaged in any other rehabilitation programme for study duration; (ii) unstable blood pressure; and (iii) peripheral neuropathies affecting sensorimotor function. The inclusion and exclusion criteria were deliberately minimal to assess whether Wii-based movement therapy has the potential to provide rehabilitation for those patients not normally targeted in such therapies. To ensure that functional improvements were not primarily due to skill acquisition or learning the Wii games, 5 healthy control subjects, 2 female and 3 male, mean age 58.8 years (SD 13.5) (range 41–71 years), completed Wii training and all functional assessments except joint range-of-motion. All subjects provided written, informed consent. The study was conducted in accordance with the Declaration of Helsinki and approved by the Human Research Ethics Committee, University of New South Wales.
|
Table I. Patient characteristics |
||||||||||
|
Patient number |
Age (years) |
Sex |
Time post-stroke (months) |
Stroke type |
Aff side |
Dom hand |
WMFTb pre time (s) |
WMFTb post time (s) |
FMAc pre (score) |
FMAc post (score) |
|
1 |
73 |
M |
38 |
I |
R |
R |
354.9 |
305.8 |
42 |
44 |
|
2 |
74 |
M |
11 |
I |
L |
R |
441.9 |
425.4 |
46 |
49 |
|
3 |
42 |
F |
1 |
I |
R |
R |
28.1 |
18.7 |
57 |
59 |
|
4a |
63 |
M |
26 |
I |
R |
R |
1342.0 |
1350.5 |
15 |
24 |
|
5 |
72 |
M |
6 |
I |
L |
R |
715.6 |
448.8 |
40 |
41 |
|
6 |
83 |
F |
11 |
I |
R |
R |
44.1 |
25.0 |
51 |
60 |
|
7 |
50 |
M |
14 |
H |
R |
R |
194.8 |
69.9 |
45 |
54 |
|
Mean |
445.9 |
389.7 |
42.3 |
47.8 |
||||||
|
SEM |
174.8 |
192.8 |
5.5 |
5.1 |
||||||
|
aDenotes the patient with expressive aphasia; aff side: more-affected side; dom hand: dominant hand pre-stroke; bWMFT sum of 15 timed tasks, maximum possible time 1800 s; cFMA upper limb portion motor subscale, maximum score 66. M: male; F: female; WMFT: Wolf Motor Function Test; FMA: Fugl-Meyer Assessment; SEM: standard error of the mean; R: right; L: left; I: ischaemic; H: haemorrhagic. |
||||||||||
Functional assessments
Primary outcome measure. Functional ability of the more-affected side of stroke patients and the dominant hand of controls was assessed prior to therapy and again immediately afterwards using the Wolf Motor Function Test (WMFT) as the primary outcome measure (17). The 2 strength tasks and 15 timed tasks of the WMFT were scored separately. Tasks replicate every-day activities, such as turning a key in a lock and picking up a pencil.
Secondary outcome measures. Patients were also tested using the upper extremity portions of the motor subscale of the Fugl-Meyer Assessment (FMA) (18), in which a maximum score of 66 signifies healthy functional use of the arm. Gross manual dexterity was tested using the Box & Block Test (19), in which subjects move as many 2.5 cm blocks as quickly as possible using only the thumb and index fingers during a timed 60 s trial. Passive and active range-of-motion were measured on the more-affected side for shoulder flexion and lateral abduction, and elbow flexion (20). Spasticity was assessed at the shoulder, elbow and wrist using the modified Ashworth scale (21) and balance with the Berg Balance scale (22).
Assessments and training were conducted using standardized protocols by the first 3 authors, working in pairs. All assessments, except for the FMA and balance, are quantitative and provide little opportunity for bias. Both training and the pre- and post-therapy testing were conducted by the same pair, but not every subject was tested by the same combination of authors.
Self-rated assessments. The patient group also completed 3 self-rated assessments. The Quality of Movement scale of the Motor Activity Log (MAL-QOM), has been shown to reflect how well the more-affected extremity is used in everyday tasks, and the 30-item log was completed daily (23, 24). Scores for each task range from 0, where the more-affected hand is not used at all, to a score of 5, in which the more-affected hand is used in the same manner as before the stroke. After the final therapy session satisfaction and perceived functional improvement with Wii-based movement therapy were rated out of 10 using a visual analogue scale.
Wii protocol
The protocol used for Wii-based movement therapy was modelled on that of the EXCITE trial of constraint-induced movement therapy (25). Patients played Wii games over 14 days, with 1 h of formal supervised training in the laboratory on 10 consecutive weekdays augmented by home practice that progressively increased from 30 to 180 min per day using a second Wii system installed in patients’ homes on day 2. Home practice was monitored via daily schedules, motor activity diaries and carer feedback. Healthy control subjects used the Wii remote with their dominant hand, completing only the formal 60 min session each day. The only participants to have had prior, but limited, exposure to the Nintendo Wii Sports were the 42-year-old female stroke patient and an age- and sex-matched healthy control subject.
For patients, the first formal hour of therapy was used as an assessment of the suitability of different games and/or movements and what modifications were required. Therapy consisted of playing the Wii Sports games of tennis, golf, boxing, bowling and baseball. Patients and healthy control subjects used the system to play games according to the rules or to engage in game-specific training drills. The latter include practicing golf putting or driving, and baseball pitching or hitting home-runs. Patients used the Wii remote in their more-affected hand to control play. When necessary they were allowed to stabilize the handset using the less-affected hand and such assistance was progressively reduced and removed by day 14. Games were introduced and varied in accordance with each patient’s ability and to prevent potential overuse discomfort. Each formal session concluded with the in-built test of “Wii Fitness”, in which game skills are assessed for tennis, bowling and baseball. The game software calculates a “Wii age” to represent a combination of improved skill and performance levels. The maximum age is 80 years, regardless of ability.
The amount of practice was determined as time-on-task, not the number of games played. Included in this time was the time taken to activate the system using the remote control (nominating right or left hand, selecting the game, etc.). Whereas healthy subjects take < 1 min to accomplish these tasks, patients can take > 10 minutes. A similar time difference occurred when using the remote to change from one game or activity to another. The number of trials to successfully complete a game or training drill was less for healthy controls, further increasing the time difference for any particular activity between patients and healthy controls. Thus, if the time taken to complete the required activities is not considered, on average, patients and healthy control subjects played an equivalent number of Wii games and activities over the two-week period.
Data analysis
The WMFT was analysed in 4 categories: performance time, performance time excluding tasks that could not be performed in the allocated 120 s, weight lifted and grip strength. Patient demographics are described as mean and SD. Normally distributed data were analysed using paired t-tests for pre- and post-therapy values and are presented as mean ± standard error of the mean (SEM). Non-normally distributed data were analysed using the Wilcoxon signed-rank test and presented as median and interquartile range (IQR). Differences were considered significant when p < 0.05.
RESULTS
All 7 patients successfully completed the allocated hours of formal therapy and home practice, while the healthy control subjects participated in formal training sessions only. Balance and active range-of-motion results represent data for 5 patients only, as these tests were added after the trial began. Due to an unrelated medical condition, one subject was unable to complete post-therapy assessments for the balance test and timed walk. Two-month follow-up assessments were conducted for 3 patients; statistical analyses were not undertaken for these data due to the small numbers involved. No significant differences were found for any test between pre- and post-training scores for healthy control subjects except for “Wii age”. Therefore, the results that follow are given only for patients, except for “Wii age”.
Functional ability
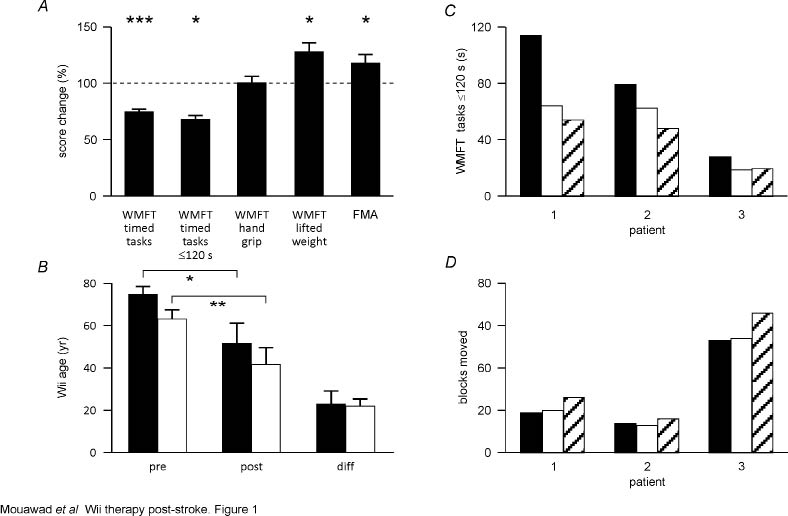
Wolf Motor Function Test and Fugl-Meyer Assessment. The mean time decreased from 3.2 s (1.5–21.9 s) to 2.8 s (0.8–14.3 s) per WMFT task (p < 0.001), as did the log of performance time, 0.5 (0.2–1.3) to 0.4 (–0.1–1.2) (p < 0.001). The mean ± SEM summed time for tasks that could be completed in ≤ 120 s decreased significantly, by 27.0% from 65.6 ± 14.9 s to 47.9 ± 11.2 (p = 0.027) (Fig. 1A); the log of these times also decreased from 1.7 ± 0.1 to 1.6 ± 0.1 (p =0.006). The weight-lifting task improved from 8.6 ± 2.6 lb to 11.4 ± 2.9 lb (p = 0.018), while handgrip strength did not change. This compared with FMA upper extremity scores, which increased from 42.3 ± 5.0 to 47.3 ± 4.7 (p = 0.013) (Fig. 1A).
Fig. 1. Functional improvements with Wii-based movement therapy (n = 7). (A) Changes in Wolf Motor Function Test (WMFT) and Fugl-Meyer Assessment (FMA) scores post-therapy normalized to pre-therapy values (horizontal line). The reduction in performance scores represents a significant improvement in timed tasks. First column: all timed tasks; second: tasks completed in <121 s. The weight lifted improved significantly, but handgrip strength did not. (B) Wii age significantly improved post-therapy for both patients (filled bars) (n = 5) and healthy controls (empty bars) (n = 5), but the amount of change that occurred was not different between groups. (C and D) Patients 1–3 (Table I) at pre-therapy (filled bars), immediately post-therapy (empty bars), and follow-up 2 months post-therapy (hatched bars) for (C) WMFT tasks completed in ≤ 120 s and (D) Box and Block Test. *p < 0.05; **p < 0.01; ***p < 0.001.
Motor Activity Log Quality of Movement. Use of the more-affected hand in everyday life improved significantly, with MAL-QOM scores increasing from a mean of 2.1 ± 0.7 to 2.9 ± 0.6 post-therapy (p = 0.008) (Fig. 2A). Summed scores for all 30 items increased from 63.2 ± 20.6 to 87.5 ± 17.2 (p = 0.009). The mean number of everyday tasks that could not be performed pre- and post-therapy was significantly reduced, from 9.1 to 4.0 (p = 0.022). The number of tasks that were scored > 3 (independent use of the hand) increased by a mean of 9.1% post-therapy.
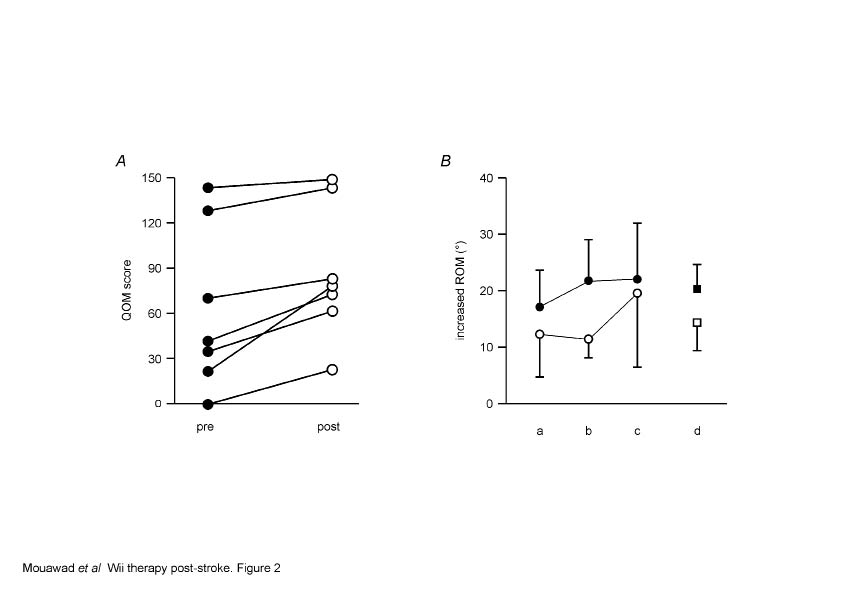
Fig. 2. Wii-based movement therapy improvements in other domains. (A) Quality of Movement scale of the Motor Activity Log (MAL-QOM) scores improved for all patients regardless of pre-therapy functional ability (n = 7). (B) Improved range-of-motion for a. shoulder flexion, b. shoulder lateral abduction, c. elbow flexion, and d. mean of all joints, for both passive (filled symbols, n = 7) and active (open symbols, n = 6) measurements. ***p < 0.001.
Shoulder and elbow range-of-motion increased (p < 0.001). The mean ± SEM improvement in passive range-of-motion (n = 7) was 20.1 ± 4.4º and active range-of-motion (n = 5) was 14.3 ± 4.8º (Fig. 2B). Although there were significant differences between the more-affected side and the less-affected side (p < 0.01) for gross manual dexterity, like balance they did not change post-therapy. The mean number of blocks moved pre-therapy was 25.5 ± 6.1, post-therapy 27.3 ± 6.3. Mean Berg Balance Scores were 49.2 ± 3.4 pre-therapy and 53.2 ± 2.1 post-therapy. Improvements in spasticity were noted in the more-affected upper limb, with scores decreasing from 2.0 ± 2.8 to 1.7 ± 2.6, but this change did not reach statistical significance.
Wii performance and satisfaction
“Wii age” was calculated at the end of every session for 5 stroke patients and 5 healthy controls (2 patients were unable to complete all necessary games). There were significant differences in Wii age from the first to the last session for both patients (p = 0.022) and healthy controls (p = 0.005) (Fig. 1D). However, there was no difference in the magnitude of the change for either group, the mean ± SEM difference being 22.6 ± 6.2 years for patients and 21.6 ± 3.8 years for healthy control subjects. While healthy control subjects played only 1 h a day, patient playing hours increased from 1 h a day to a maximum of 4 h a day. Over 14 days the mean scheduled playing time is 2.2 h per day, Wii-based movement therapy patients completed 2.4 ± 0.2 h per day. When asked to rate their satisfaction with Wii-based movement therapy, most patients were highly satisfied, with a mean score of 9.4 ± 0.4 on the visual analogue scale (Fig. 3). Similarly, all but 1 perceived they had improved functional ability assessed on the same scale, with a mean score of 7.0 ± 0.8 (Fig. 3).
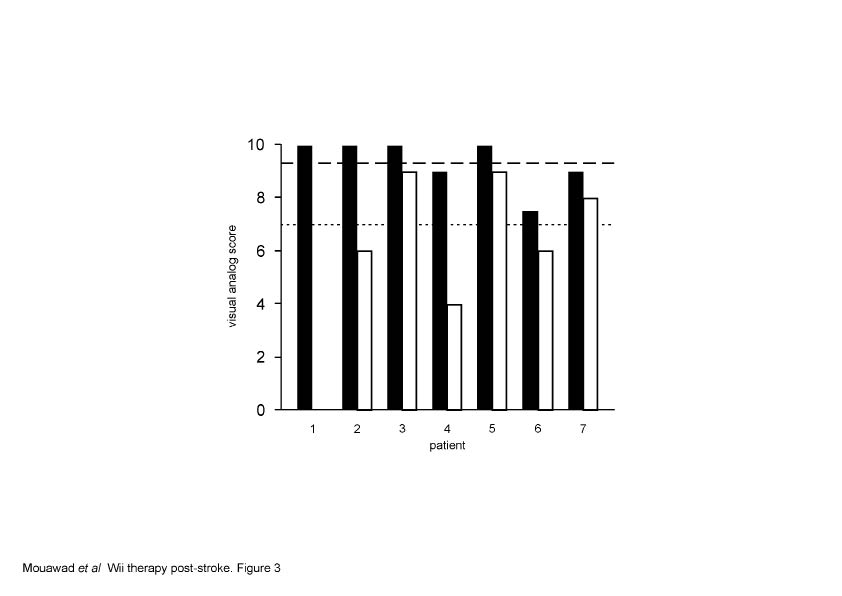
Fig 3. Patient satisfaction and improvement. Wii-based movement therapy satisfaction was rated on a 10-point visual analogue scale by each patient (Table I), mean = 9 (dashed line). Patient’s perception of their own improvement was rated on the same scale, with a mean of 7.4 (dotted line).
Two-month follow-up
Three patients were reassessed two months after Wii-based movement therapy. No attempt was made to control or account for activity during this time, whether therapeutic or otherwise. The post-therapy WMFT performance time for these patients was improved to a mean of 32.7% in comparison with pre-therapy scores. This improvement was not only retained but increased to 40.8% at follow-up (Fig. 1C). The number of blocks moved with the more-affected hand during the Box and Block Test by these patients pre-therapy (mean 28.7 blocks) was not changed after therapy (mean 29.0), but improved to a mean of 36.0 blocks at follow-up, an increase of 25.2%. These changes suggest a continued therapeutic effect of Wii-based movement therapy.
DISCUSSION
An intense two-week programme of Wii-based movement therapy improved functional upper-limb movement post-stroke in this small group of patients. This was despite both the heterogeneity of the population and the formal rehabilitation previously undertaken by all patients. Although the sample size of this study limits the generalizability of the results to the wider stroke population, significant improvements in the WMFT and MAL-QOM suggest that the gains from Wii-based movement therapy transferred to activities of daily living, and that the improved WMFT scores were clinically significant. These gains were accompanied by increased joint range-of-motion, both passive and active. While the number of patients in this trial was small, the diversity of their functional disability (Table I) reflects the heterogeneity of stroke survivors. In spite of this diversity, all patients gained improved functional use of the more-affected hand and arm during both testing (Fig. 1) and in activities of daily living (Fig. 2A).
A healthy control group of stroke patients receiving standard care alone was not included in this trial as previous studies have shown stroke patients receiving standard care for similar periods of time show no significant improvement in functional tests. Such studies include both a large, multi-site trial with 104 patient controls over a 2-week period (3) and a smaller single-site trial of 5 patient controls over 4 weeks (26). The small group of healthy control subjects was included to investigate whether the changes observed for the patient cohort could be due to skill acquisition or a learning effect, or if the functional testing items mimicked tasks practiced during Wii-based movement therapy (see below). On qualitative measures all healthy controls had maximal scores both pre-and post-training for the FMA and Berg Balance Test. The question of a ceiling effect for functional testing of the healthy control subjects is largely reduced by the use of timed tasks for the WMFT and Box and Block Test, and the test of grip force. Three healthy control subjects improved on the WMFT timed tasks, but two were slower; results for the Box and Block Test followed the same pattern (but not for the same individuals); and grip force was 1–2 kg lower in post-training testing for all healthy controls. Healthy controls were gender matched to one of the patients, and age-matched ± 2 years. Thus patients 2 and 6 (Table I) were not matched.
The recovery of functional ability was not simply a consequence of learning to play Wii games, which was assessed as a lowered “Wii age”. We do not know how “Wii age” is calculated. It appears to reflect a combination of factors including the distance a ball is hit, the number of trials required for successful completion of a task, and the number of successful tasks. The change in “Wii age” was the same for both healthy control subjects and patients, but functional testing scores improved only for the patients. Thus the absolute difference in Wii age between patients and healthy control subjects presumably reflects the difference in motor ability. This result suggests that the overall skill acquisition or learning effect for both groups was comparable, regardless of the additional Wii practice time undertaken by stroke patients; and that the improvements in functional testing for stroke patients were in addition to learning and improving Wii skills. These results provide encouraging evidence to suggest that improvements in Wii skills were generalized to the functional tasks tested by the WMFT and FMA that were not practiced during the two weeks of therapy, although this point requires further investigation.
The success of Wii-based movement therapy has been demonstrated previously in patients in the early sub-acute period (< 3 months) after stroke (15). One patient in the current study fell within this period, 1 was in the late sub-acute period (3–9 months) and 5 were in the chronic (> 9 months) period post-stroke. In the present study, the FMA scores pre- and post-therapy were comparable to those of Joo et al. (15), but the mean level of spasticity was approximately double that in the present study. The intensity of training used by by Joo et al. (15) was less than in the present study, with 6 30-minute sessions over a two-week period as an adjunct to occupational therapy. This combined therapy makes discrimination of the effects of Wii therapy more difficult. Patients in the present study were not undertaking any other rehabilitation, and so the improvements, particularly in those patients > 9 months post-stroke when natural recovery will be minimal (3, 26), are more likely to reflect the benefits of Wii-based movement therapy per se.
The potential for overuse injuries with Wii use has been identified in healthy people with intense and continuous exposure to Wii at first use (27) and patients immobilized through illness (28), and suggested as a potential risk for stroke patients (15). The progressive exposure to Wii use and the importance of changing games and drills every 10–20 min to prevent potential overuse injuries was stressed throughout this trial and monitored via patients’ daily diary. The accuracy of the diary was confirmed with each patient’s carer. Patients were encouraged to take rest breaks as necessary, and training hours were calculated from playing time not including breaks. We did not encounter any overuse injuries or other adverse side-effects of Wii-based movement therapy in this training paradigm. All participants completed their designated hours of training and practice.
Methodological considerations
The Wii and Wii Sports were used without modification even though the system and its games are not designed for stroke patients. Stroke patients found the control of handset buttons difficult and frustrating, however this obligatory hand use improved gross motor dexterity. These improvements were not significant at post-therapy testing, but were increased two months later (Fig. 1B). The timing and feedback from Wii Games also caused frustration. We therefore developed scoring and feedback that better reflected the progress of our participants. For example, in tennis we differentiated between balls that were hit and balls that were returned in court. Increased hitting always preceded an increase in balls remaining in play, an indicator of improved motor control. Similarly, the automated feedback such as “missed” is based on the rules of each game and is often regarded as a negative aspect of the Wii system. With therapist intervention patients learnt to interpret such feedback as a motivational challenge.
The diversity of stroke outcomes requires therapy to be tailored to each patient’s deficits. The use of the Wii system allowed for the introduction and difficulty of games and drills to be varied according to individual ability and progress. Stroke patients did not simply play Wii Sports, rather the device was used as a rehabilitation tool with targeted and specific movement goals aimed at reinforcing appropriate and co-ordinated motor patterns. Care was taken to ensure bad habits were not practiced. As reported previously (15) weak handgrip was overcome with bandaging and patients could undertake therapy seated. When assistance was required for insufficient balance, strength or dexterity a staged approach was used. Such aids were progressively reduced until games were played with minimal assistance. For example, the extent of bandaging was reduced day by day as handgrip strength increased. Improved balance stability was apparent, although the difference on testing did not reach significance. However Berg Balance Scale scores for two patients increased by 6 (from 47) and 10 points (from 35) and it has been suggested that improvements of this magnitude, while not statistically significant, may represent a “true change” in functional balance (29). Scores for the timed WMFT tasks, FMA, both active and passive range-of-motion, and the weight-lifting task in the WMFT were significantly improved, but maximum handgrip strength did not increase (Fig. 1A). This result suggests that grip strength was not addressed by Wii use and adjuvant therapy may be necessary.
Advantages of the system
A fundamental question in virtual reality therapy is whether gains from the virtual environment transfer to activities of daily living (15). Most virtual reality studies assess improvements using clinical measures of functional ability or range-of- motion, such as the WMFT and FMA, both of which significantly improved with Wii-based movement therapy (p = 0.006 and p = 0.013, respectively) in a manner and magnitude similar to other trials (15, 26, 30). The MAL-QOM was used as a measure of the transfer of rehabilitation gains to real-world activities of daily living (24). MAL-QOM scores increased by 38% (p = 0.008) and patients reported use of the more-affected hand and arm in more activities than they previously thought possible. This represents a reversal of the phenomenon known as “learned non-use” (23) whereby patients find tasks quicker, less frustrating and more successful using the less-affected hand and arm.
Feedback is fundamental to motor skill learning and performance efficiency (31). Higher motivation is associated with better rehabilitation outcomes (32), which may in turn minimize problems with compliance (6). Patients in this study unlike previously (15), found the Wii games reassuringly familiar. Such familiarity facilitated interest and motor learning, promoting motivation through the in-built commentary, prizes, visual and verbal cues. The nature of Wii Sports tapped into patients’ innate competitive nature, further facilitating compliance and motivation even for those who denied being competitive. Daily feedback of game-by-game progress was used to redefine therapy goals and appears to have promoted exercise adherence, although this was not measured directly. The range of different skills and task-based techniques learnt each day meant that the “hard work” of therapy was no longer perceived as a chore. This is evident in the satisfaction score for the present study and previous virtual-reality therapy trials (Fig. 3) (11, 12, 15, 33, 34). Three subjects initially suggested satisfaction scores > 10, but were restricted to the range of the visual analogue scale.
This study extended the use of Wii-based movement therapy into the chronic period post-stroke. Use of the more-affected upper extremity was increased both in therapy and in the real world for both subacute and chronic patients. Further improvements were seen at follow-up, albeit in only 3 subjects, suggesting that there may be a sustained therapeutic benefit following Wii-based movement therapy. The system is inexpensive, easy to use and appears to be effective. All patients were able to use the system at home, without the constant supervision of a therapist and bought their own system after completing the therapy, and report continued improvements in motor function. Further research is needed to identify the optimal design, intensity and duration of Wii-based movement therapy and to assess its efficacy in contrast to conventional strategies. The use of Wii-based movement therapy in telerehabilitation is yet to be explored, but the simplicity and affordability of the system emphasizes the potential to provide therapy access via broadband internet connections for patients isolated in rural centres.
AcknowledgementS
This work was supported by the NSW Office of Science and Medical Research (Spinal Injury and other Neurological Diseases Research Program).
REFERENCES

