Didier Pradon, PhD1, Nicolas Pinsault, PT, PhD2, Raphaël Zory, PhD1 and
François Routhier, PhD3
From the 1Groupement de Recherche Clinique et Technologique sur le Handicap (EA 4497), CIC-IT 805, CHU
Raymond Poincaré, Garches, 2Ecole de kinésithérapie du Centre Hospitalier Universitaire, Grenoble, France and
3Centre interdisciplinaire de recherche en réadaptation et intégration sociale (CIRRIS), Institut de réadaptation en
déficience physique de Québec (IRDPQ), Québec, Canada
OBJECTIVE: To determine the relationship between mobility performance measures and Wheelchair Skill Test (WST) scores and to establish the test-retest and inter-rater reliability of these measures.
METHODS: Forty patients with spinal cord injury participated in this study. Subjects performed the Wheelchair Skill Test and mobility performance tests: maximal velocity (Vmax), spontaneous velocity (Vspont) and a 10-m back and forth slalom (Stime). Eighteen patients with spinal cord injury participated in a second testing session to evaluate test-retest reliability and, among these patients, 8 participated in a third testing session to evaluate inter-rater reliability.
RESULTS: Spearman’s correlation coefficients calculated between WST and Vmax, Vspont and Stime were high and significant (p < 0.05). The intraclass correlation coefficients (ICC (2.1)) evaluating test-retest reliability for Vmax, Vspont and Stime were 0.94, 0.84 and 0.88, respectively. The ICC evaluating inter-rater reliability for Vmax, Vspont and Stime were 0.92, 0.92 and 0.95, respectively. Reliability results were confirmed by Bland-Altman plots.
CONCLUSION: Vmax and Stime could be used to evaluate wheelchair skills and to create a new scale, whereas Vspont is the least appropriate of these measurements to describe wheelchair skills.
Key words: spinal cord injury; evaluation; Wheelchair Skills Test; Spearman’s correlation.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Didier Pradon, EA 4497 GRTCH, CIC-IT 805, Laboratoire d’analyse de la marche – Hôpital Raymond Poincaré, 104 Bd Raymond Poincaré, FR-92380 Garches, France. E-mail: didier.pradon@rpc.aphp.fr
Submitted May 2, 2011; accepted October 21, 2011
Introduction
The Council of Europe estimated in 2002 that by 2005 more than 2.5 million people worldwide could be living with spinal cord injury (SCI) (1). Whereas it is difficult to establish an accurate picture of the epidemiology of spinal cord injuries (SCI), more recent studies are in line with the Council of Europe estimate, and show that the prevalence of SCI is increasing (2, 3). Most patients with SCI need rehabilitation and physiotherapy to help them maximize their potential and learn to live efficiently as wheelchair users. To enable this process, the objective evaluation of manual wheelchair skills is of great importance.
There are some excellent instruments to evaluate manual wheelchair skills described in the literature (4–6). The Wheelchair Skill Test (WST), which was initially proposed by Kirby et al. (6) in 2002 and subsequently revised systematically (7), has the advantage of evaluating manual wheelchair function at the level of activities of daily living, and demonstrates good metrological properties (8). In fact, establishing the reliability and validity of a given evaluation constitutes an important, but not sufficient, prerequisite for its use and for the interpretation of collected parameters. For example, practical considerations, such as applicability (9), which is the quality of a tool that enables its use with a given population or in a specific context, appear to be an important complement to metrological properties. In fact, the WST is traditionally mentioned as the standard for these objective evaluations, but it sometimes fails to reach the standards required for widespread use (10). Different wheelchair or mobility performance tests have been developed. For example, a 9-task wheelchair circuit (including a sprint, figure-of-8 shape, transfer, etc.) has been proposed and validated by Kilkens et al. (11). This kind of test presents very good reliability. However, the applicability of the test under clinical conditions is more difficult because it requires time and equipment. At the same time, many simple outcomes are collected during adapted physical activity or physiotherapy sessions that could expand on fill out the WST evaluation and make the wheelchair selection process easier for clinicians and their patients. Among these outcomes, we can take into account the mobility performance measures, corresponding to the wheelchair users’ ability to move easily and efficiently, which bring together wheeling performance (expressed through speeds) and handiness (expressed through the time taken to perform a slalom).
The aim of the present study was to determine the relationship between mobility performance measures and WST scores and to establish the test-retest and inter-rater reliability of these measures.
Methods
Subjects
Forty SCI patients participated in the first testing session (30 males and 10 females; mean age 36.9 years (standard deviation (SD) 11.2); mean height 172.8 cm (SD 9.9); mean weight 68.6 kg (SD 12.5)). Within these subjects, 18 could be classified as low paraplegics (level of SCI from T10–L3), 15 as high paraplegics (T1–T9) and 7 as tetraplegics (C6–C7). We used a heterogeneous sample in order that the sample was as close as possible to clinical realities and interrogations. All the SCI patients were, or had been, involved in a rehabilitation programme. The subjects had a mean of 79.8 months’ experience (range 1–360). There was no attempt to stratify the sample on the basis of age, sex or level of SCI. The study inclusion criteria were: 20 years of age or older; cooperative and pain-free; competent to give informed consent; and willing to participate. Prior to involvement in this study, each participant signed a letter indicating informed consent. The study was conducted according to the Declaration of Helsinki and approval for the project was obtained from the institutional ethics committee.
Experimental procedure
The 40 patients with SCI participated in the first testing session (S1). First, subjects performed the WST (3.2 version). The WST was administered as outlined in the WST test manual (7). WST provides capacity scores for each skill based on explicit criteria. Each participant was evaluated in the wheelchair that they were using on the day of the study and equipped in his or her usual manner when using the wheelchair. The total scores were calculated according to the WST 3.2 manual (7).
Next, subjects performed the 3 wheelchair mobility tests: (i) maximal velocity (Vmax; km/h); (ii) spontaneous velocity (Vspont; km/h); and (iii) slalom (Stime; s). For Vmax measurement, subjects were instructed to wheel the chair in a 20-m straight line at the fastest speed they could reach. Value of Vmax was obtained for the first 12 m only. Three trials were completed, and the fastest was accepted as the measure of Vmax. Vspont was obtained by asking subjects to wheel the chair in a 20-m straight line at their preferred speed. The value of Vspont was obtained for the first 12 m only. Three trials were completed and their mean was accepted as the measure of Vspont. To evaluate the handiness of the wheelchair, subjects performed a 10-m back and forth slalom (each block separated by 1 m) as fast as possible. The measure (slalom) was the total time (Stime; s) needed to complete the task considering that each missed (or felt) block added 10 s to the total slalom time.
Eighteen SCI patients agreed to participate in a second experiment (S2, 15 males and 3 females) and, among these patients, 8 participated in a third experiment (S3, 5 males and 3 females). S2 and S3 were similar to S1. For S2, the entire procedure evaluating wheelchair mobility performance was repeated by the same rater as for S1, on the 18 patients after a 1-week interval to evaluate test-retest reliability. For S3, two different raters administered the entire procedure, evaluating wheelchair mobility performance for 8 patients within the same day to evaluate inter-rater reliability. Values obtained for each experimenter were not communicated to the other.
Statistical analysis
All statistical calculations were carried out with R 2.0.1 software (R Core Development Team). Means, SD, range and standard errors were calculated for each parameter. A level of p < 0.05 was used to identify statistical significance. Considering that the data do not appear to follow a normal distribution, the relationship between WST scores and Vmax, Vspont and Stime was established using a Spearman’s rank correlation coefficient (Rs). The Rs values were interpreted according to Domholdt recommendations (12). Spearman’s rank correlation coefficients were calculated for: (i) total sample (n = 40); (ii) the 20 subjects with the worst WST score (G1, n = 20); and (iii) the 20 subjects with the best WST score excluding patient with the maximal score (G2, n = 20).
The test-retest and inter-rater reliability of Vmax, Vspont and Stime were assessed with the intraclass correlation coefficient (ICC (2,1)) (13) and according to Fleiss’ classification (14). The standard error of measurement (SEM) and the 95% confidence interval (CI) of ICC values were calculated for all dependent variables (15). The use of the 95% CI demonstrates how closely the measurements agree on different occasions, whereas the SEM indicates the precision of measurements. Finally, Bland-Altman graphs were formed to give a visual interpretation of the data as well as to determine potential bias (16).
Results
The total group of subjects obtained a mean WST score of 83.8% (SD 16.6%) (range 47.0–100.0%), a mean Vmax of 6.91 km/h (SD 2.10) (range 3.6–11.7), a mean Vspont of 4.74 km/h (SD 1.21) (range 2.6–7.5) and a mean Stime of 60.4 s (SD 29.6) (range 25.0–153.0). For the total sample and G1, Spearman’s rank correlation coefficients between WST score and mobility performance measurement (Vmax, Vspont and Stime) were all significant (Table I). According to Domholdt recommendations (12), the correlation between WST score and Vmax and Stime is high, whereas the correlation between WST and Vspont is moderate. Spearman’s rank correlation coefficients calculated on G2 (n = 20) are all very low and non-significant.
| Table I. Spearman’s rank correlation coefficient between Wheelchair Skill Test score and the maximal velocity (Vmax), the spontaneous velocity (Vspont) and the slalom time (Stime) for the total sample (n = 40), group 1 (n = 20) and group 2 (n = 20) |
| Variables | Total | Group 1 | Group 2 |
| Vmax | 0.72* | 0.80* | 0.31 |
| Vspont | 0.57* | 0.64* | 0.17 |
| Stime | –0.75* | –0.75* | –0.33 |
| *Indicate that Spearman’s rank correlation coefficient were significant at p < 0.05. |
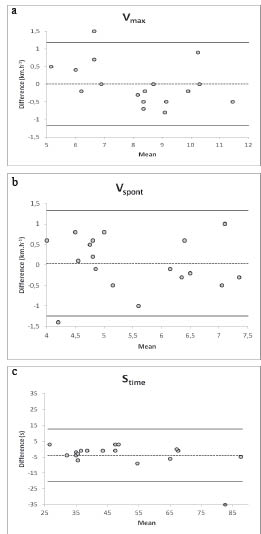
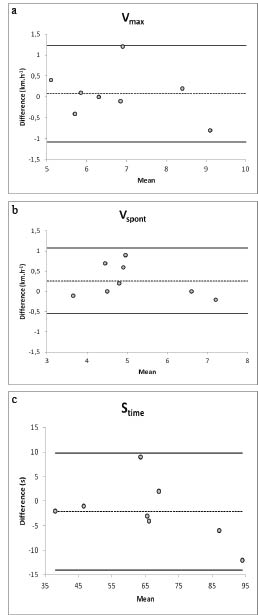
Concerning the test-retest reliability (n = 18), analysis of Vmax showed an ICC of 0.94 (95% CI 0.86–0.98, SEM 0.15). For Vspont, the ICC value was 0.84 (95% CI 0.68–0.91, SEM 0.26) and for Stime the ICC value was 0.88 (95% CI 0.72–0.98, SEM 2.92). Finally, for the inter-rater reliability (n = 8), the ICC value was 0.92 for Vmax (95% CI 0.60–0.98, SEM 0.17), 0.92 for Vspont (95% CI 0.15–0.99, SEM 0.11), and 0.95 for Stime (95% CI 0.82–0.98, SEM 1.35). In addition to those good to excellent ICCs, Bland-Altman plots showed no specific or major trends between testers or between testing time (Figs 1 and 2).
Fig. 1. Test-retest Bland-Altman plots: difference against mean for (a) maximal velocity Vmax; (b) spontaneous velocity Vspont; (c) slalom time Stime. Dotted line: mean. Solid line: limits of agreement according mean ± 2 standard deviations.
Fig. 2. Inter-rater Bland-Altman plots: difference against mean for (a) maximal velocity Vmax; (b) spontaneous velocity Vspont; (c) slalom time Stime. Dotted line: mean. Solid line: limits of agreement according mean ± 2 standard deviations.
Discussion
The aim of the present experiment was to determine the relationship between wheelchair mobility tests and WST scores and the test-retest reliability and inter-rater reliability of these measures. The key findings of this study were that: (i) the relationship between mobility performance test and WST score are high when considering patients with the lowest score at the WST (G1) or the total sample; and (ii) the test-retest reliability of the 3 mobility performance tests (Vmax, Vspont and Stime) is excellent.
The WST scores of the 40 SCI patients were first compared with wheelchair mobility performance measures such as Vmax, Vspont and Stime. Firstly, our results showed that Vmax and Stime were “highly” correlated with WST scores, whereas Vspont was only “moderately” correlated with WST scores. In other words, the results suggest that Vspont is the least appropriate of the measures in this study to describe wheelchair skills. This result is not surprising considering that the instruction “to wheel at preferred speed” is highly subjective for the subjects and very difficult for the clinician to interpret. The high level of correlation found between WST and Vmax and Stime also underlines the good general validity of the WST. However, the very low Spearman’s rank correlation coefficient observed between WST scores and the mobility performance tests for G2 (the best scores on WST, n = 20) highlighted an important limit of the WST. Indeed, this result shows that the WST has difficulty in differentiating patients with a high level of performance. Although the WST has the advantage of being applicable to all kinds of wheelchair users, when we consider the application of this test for specific users, such as patients with SCI, there are some difficulties in discriminating patients. In fact, sportsmen with SCI generally obtained maximum or very high scores on the WST, whereas clinically they might exhibit very different skill and mobility performances.
Secondly, our results showed that all parameters demonstrated excellent test-retest and inter-rater reliability. For Vmax, these results confirm those of a recent study that highlighted high test-retest and inter-rater reliability on a similar test (13). Nevertheless, the reliability is necessary, but not sufficient, for an evaluation to be used. In fact, Mortensen et al. (10) underlined the importance of the applicability. On this particular point, the evaluation of wheelchair mobility performance measures takes less than 5 min. These measures could be a good counterpart to the WST, which is much more time-consuming and perhaps less discriminative. Taken together, these results suggest that Vmax and Stime could be used in clinical practice and integrated in a new scale that is reliable, easy to use and not time-consuming.
It is important to note that this study focused only on SCI patients, whereas many other persons use manual wheelchairs. However, focusing on this group enabled us to evaluate a wide range of wheelchair skills. Moreover, because of personal constraints, only a few patients participated in experiments evaluating the reliability of the measures, thus widening the 95% CI of the ICC and limiting the impact of our results. Future research will study more subjects in order to develop a new scale that is easy to use, is not time-consuming and is based on performance measures.
Acknowledgement
The authors would like to thank the all of the subjects for their time and for enduring the rigors of the protocol and data acquisition process.
References