Bastien Guillebastre, PhD1, Paul Calmels, MD2 and Patrice Rougier, PhD1
From the 1Department of Physical Exercise, University of Savoie, Le Bourget-du-Lac and 2Department of physical medicine and rehabilitation, University hospital of Saint Etienne, Saint-Etienne, France
OBJECTIVE: The aim of this study was to examine the relationships between lower limb muscular deficiencies and postural and gait capacities.
DESIGN: Observational study.
SUBJECTS: A total of 26 patients with Charcot-Marie-Tooth disease and 19 health-matched healthy subjects.
METHODS: Barefoot gait and postural control were analysed using a walking mat and a force platform, respectively. Muscular strength of the plantar and dorsal ankle flexors were assessed using the Medical Research Council scale.
RESULTS: Gait parameters correlated with both dorsal- and plantar-flexors strength, whereas postural parameters correlated only with plantar-flexors strength. More particularly, patients with a weak deficit of the plantar-flexor muscles were characterized by normal postural control except along the antero-posterior axis. For gait control, the overall pattern defined from the gait cycle division was preserved, whereas other spatio-temporal parameters were impaired, and more so in patients with a high level of deficit of the plantar-flexor muscles.
CONCLUSION: These data highlight behaviour differences in standardized tasks, such as standing still upright or gait. Improved knowledge of postural and gait capacities may constitute a basis to emphasize the corrections that should be enabled by rehabilitation exercises or orthotic devices.
Key words: Charcot-Marie-Tooth disease; muscle deficit; gait; postural control.
J Rehabil Med 2013; 45: 314–317
Guarantor’s address: Patrice Rougier, Département STAPS, Domaine Scientifique de Savoie-Technolac, 73 376 Le Bourget-du-Lac cedex, France. E-mail: Patrice.Rougier@univ-savoie.fr
Accepted Sep 26, 2012; Epub ahead of print Feb 14, 2013
Introduction
Charcot-Marie-Tooth (CMT) disease is a hereditary slowly progressive degenerative disease that affects the peripheral nervous system. The clinical manifestations of CMT involve distal muscle weakness and sensory disturbance (1). Wide variability in motor impairment is a general characteristic of CMT disease. Clinical scales are widely used to assess muscular capacities in order to categorize patients, but no clear information can be obtained about functional consequences in daily life in general, and on standardized sensory-motor tasks, such as postural control and gait, in particular.
Several studies have assessed deficiencies in gait and postural control in patients with CMT. During standing posture, patients with CMT swayed significantly more than controls (2, 3), with no correlation between sway area and muscle strength (2). During gait, patients with CMT frequently display bilateral foot-drop, associated with inadequate plantar flexion (4), inducing a lower self-selected walking velocity (15% lower than healthy subjects taken as reference) (5), longer stride duration, lower swing velocity, shorter step length, and greater step width (6). Don et al. (6) first distinguished patients with CMT according to the deficient muscles (plantar- and/or dorsal-flexors) and found differences in basic spatio-temporal parameters.
It remains unclear, however, whether there are correlations between the level of muscular strength deficiency of the lower limbs and some functional abilities. Analysis of two different motor tasks, such as postural control and gait, which solicit neither the same muscular groups nor the same levels of muscular activation, should enable us to highlight the functional consequences of each deficient muscular group. The purpose of the present investigation was to determine which insights can be gained from data about the muscular strength of the lower limbs, assessed through clinical tests. On the one hand, considering standing posture as mainly controlled by plantar-flexor muscles (7), patients with CMT with a preserved strength of these muscles should be characterized by normal postural control. On the other hand, during gait that solicits both the plantar- and dorsal-flexors (8), it is hypothesized that the rolling of the foot should be affected (due to weakness of the dorsal-flexor muscles), whereas step length ought to be affected to a greater extent in patients with a high deficit of the plantar-flexor muscles.
Methods
Subjects
Patients with CMT were recruited during consultation in a physical medicine and rehabilitation outpatient unit and included after giving their informed consent. A total of 11 women and 15 men without equinus foot participated in the study (9) (Table I). All were able to stand quietly unaided for more than 1 min and to walk alone barefoot. Their force capabilities were tested for dorsal- and plantar-flexor muscles according to the Medical Research Council (MRC) 0–5 scale (Table II), by the same clinician during the clinical examination before the motor task assessment. While dorsal-flexors are the first muscles impaired in the progression of CMT disease, plantar-flexors are affected to a variable degree. Classifying patients according to their muscular deficit might help better identify their functional abilities. Patients were therefore classified into two groups according to whether they were able to move the ankle joint against resistance (Gr 1: plantar-flexor MRC score ≥ 4 and Gr 2: plantar-flexor MRC score < 4). Thus, only patients in Gr 1 were able to produce a movement against gravity, which is a prerequisite for achieving motor tasks. Interestingly, we observed that, in both groups, approximately half of the patients presented a deep and superficial sensory deficit (Table I). Nineteen matched healthy subjects free of neurological and orthopaedic disorders also participated in the study. This study was approved by the local ethics committee (11 March 2009).
|
Table I. Clinical characteristics of Charcot-Marie-Tooth (CMT) patients and healthy subjects. Paired and unpaired t-tests were computed to analyse the differences between groups and muscular groups, respectively |
|||||
|
Healthy subjects |
Patients with CMT |
Gr 1 |
Gr 2 |
p-value |
|
|
Sex, F/M, n |
10/9 |
11/15 |
5/6 |
6/9 |
|
|
Age, years, mean (SD) |
49.4 (10.7) |
50.7 (16.0) |
43.7 (20.3) |
55.3 (11.0) |
0.23 |
|
Height, cm, mean (SD) |
167.6 (8.3) |
167.2 (10.8) |
168.9 (13.5) |
166.0 (8.8) |
0.62 |
|
Weight, kg, mean (SD) |
67.7 (13.6) |
64.8 (12.5) |
63.7 (12.4) |
66.0 (12.6) |
0.53 |
|
MRC ankle score |
|||||
|
Dorsal-flexors |
– |
1.3 (1.4) |
2.3 (1.3) |
0.4 (0.8) |
< 0.001 |
|
Plantar-flexors |
– |
2.4 (1.8) |
4.2 (0.3) |
1.1 (1.2) |
< 0.001 |
|
< 0.001a |
< 0.001b |
||||
|
Sensory deficit, % |
|||||
|
Deep |
– |
44 |
45 |
43 |
|
|
Superficial |
– |
52 |
54 |
50 |
|
|
aComparison between groups. bComparison between dorsal- and plantar-flexors. MRC: Medical Research Council; M: male; F: female; Gr 1: plantar-flexor MRC score ≥ 4; Gr 2: plantar-flexor MRC score < 4; SD: standard deviation. |
|||||
|
Table II. Correlations coefficients (r) between gait and postural parameters, and Medical Research Council (MRC) scores of dorsal- and plantar-flexors |
||
|
MRC score |
||
|
Dorsal-flexors |
Plantar-flexors |
|
|
Postural parameters |
||
|
CP-area, mm² |
–0.28 |
–0.46* |
|
CP-AP, % |
–0.31 |
0.08 |
|
BWllf, % |
0.18 |
–0.51* |
|
ML variance, mm² |
–0.38 |
–0.50* |
|
AP variance, mm² |
–0.11 |
–0.30 |
|
Gait parameters |
|
|
|
Velocity, cm/s |
0.49* |
0.50* |
|
Cadence, Hz |
0.37 |
0.36 |
|
Step length, cm |
0.39 |
0.39 |
|
Single sup, % |
0.19 |
0.03 |
|
Double sup, % |
–0.19 |
–0.04 |
|
Heel off-on, % |
–0.07 |
0.24 |
|
*p < 0.05. ML: medio-lateral; AP: antero-posterior; CP-AP: antero-posterior axis; BWllf: percentage of total body weight distributed over the less loaded foot; sup: support. |
||
Posturography
Postural capacities were assessed using a double force platform (PF02, Equi+®, Le Bourget-du-Lac, France). Subjects were asked to stand quietly barefoot in a standardized position with their feet placed on marks (heels separated by 9 cm, toes out at 30º), arms hanging freely along the body, eyes open. Data were collected through 3 trials of 32 s (sample frequency 64 Hz) separated by seated periods of 2 min (9–11). In addition to the centre-of-pressure area (CP area) (12), postural orientation was assessed through mean position, relatively to the feet length, of the CP displacements along the antero-posterior axis (CP-AP, %), and the percentage of total body weight distributed over the less loaded foot (BWllf, %). Finally, the variances (mm²) were aimed at characterizing the CP movements along the medio-lateral and antero-posterior axes (ML and AP variance, respectively). The higher the variance, the more difficult is the postural control along the axes considered. Clinically, these parameters allow identification of the main characteristics that can be improved during rehabilitation.
Gait analysis
Gait was assessed with an electronic mat (GAITRite®, CIR Systems, Clifton, PA, USA). The GAITRite® is an 8.3 × 0.89-m electronic walkway. Subjects were required to walk barefoot over a 12-m distance at a self-selected velocity (two trials separated by a seated period of 2 min). To limit variability due to acceleration and deceleration, subjects covered a distance longer than the mat, which was in the middle of the walkway.
The GAITRite® application software was used to assess gait through velocity, cadence, step length, gait cycle division (with percentage of single and double support time), and support initial contact, i.e. the percentage of time during which the rear third of the foot was on the ground (heel off-on).
Even though a different number of trials was achieved for each motor task, these tasks were performed without fatigue and with good reliability and reproducibility. Each patient was assessed through the mean of the 2 or 3 trials (for gait and postural control, respectively).
Statistical analysis
For all clinical, gait and postural parameters, normality, which was tested using Kolmogorov-Smirnov tests, led us to achieve a parametric one-way analysis of variance (ANOVA) followed, when necessary, by Newman-Keuls multiple comparison tests. Student t-tests were performed to compare clinical data, and correlations were analysed using Pearson’s coefficients. A significance level of p < 0.05 was set for all tests.
Results
Clinical data
MRC scores for the dorsal- and plantar-flexor muscles were significantly lower in patients in Gr 2 than those in Gr 1 (t = 4.699, p < 0.05 and t = 8.507, p < 0.05, respectively) (Table I). Moreover, dorsal-flexors were significantly more deficient than plantar-flexors only in Gr 1 (t = 4.659, p < 0.05) (Table I).
Relationships between muscular deficit and postural control
Significant correlations were found between plantar-flexors’ muscular deficit and most of postural parameters (p < 0.05) (Table III). Compared with healthy subjects, Gr 2 patients were characterized by a larger CP-area (q = 5.467, p < 0.05) (Fig. 1a). Interestingly, while AP variance was increased for all patients with CMT compared with healthy subjects (healthy subjects vs Gr 1: q = 2.861, p < 0.05; healthy subjects vs Gr 2: q = 3.692, p < 0.05), variance along the ML axis was disturbed only in Gr 2 patients with respect to Gr 1 patients (q = 3.737, p < 0.05) and healthy subjects (q = 5.984, p < 0.05) (Fig. 1a).
|
Table III. Medical Research Council scale explanation |
||
|
Score |
Meaning |
CMT patients |
|
5 |
Muscle contracts normally against full resistance. |
Gr 1 |
|
4 |
Muscle strength is reduced but muscle contraction can still move joint against resistance. |
|
|
3 |
Muscle strength is further reduced such that the joint can be moved only against gravity with the examiner’s resistance completely removed. |
Gr 2 |
|
2 |
Muscle can move only if the resistance of gravity is removed. |
|
|
1 |
Only a trace or flicker of movement is seen or felt in the muscle or fasciculations are observed in the muscle. |
|
|
0 |
No movement is observed. |
|
|
CMT: Charcot-Marie-Tooth. |
||
Relationships between muscular deficit and gait
Comfortable velocity correlated with both dorsal- and plantar-flexors (r = 0.49 and r = 0.50 p < 0.05, respectively) (Table III). Compared with healthy subjects, gait cycle division was preserved in patients with CMT, whatever the group (Fig. 1b). All the remaining spatio-temporal gait parameters displayed large differences between healthy subjects and Gr 2 patients (Fig. 1b). In comparison with healthy subjects, Gr 1 patients had a preserved cadence (q = 1.989, p > 0.05). Finally, gait velocity (q = 4.791, p < 0.05), cadence (q = 3.664, p < 0.05) and step length (q = 3.251, p < 0.05) were better in Gr 1 with respect to Gr 2 patients (Fig. 1b).
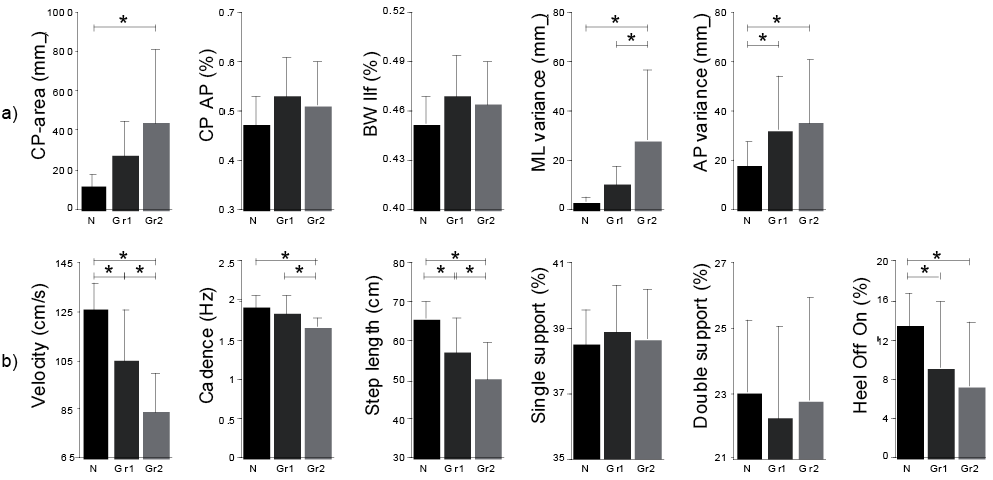
Fig. 1. Comparison of postural and gait values in 3 groups (N: normal subjects; patients with Charcot-Marie-Tooth with a weak (Gr 1) or high (Gr 2) level of deficit of the plantar-flexors). Statistically significant differences are underlined as *p < 0.05.
Discussion
This study describes the relationships between muscular deficiency of the lower limbs and the functional abilities of patients with CMT with various ankle muscular weaknesses. The results of this study are in agreement with the literature and broaden our knowledge of this topic (2, 5, 6). Analysis of gait and postural control in patients with variable muscular deficiencies allows us to identify the functional consequences of these impairments.
As hypothesized, the main parameters used to globally describe postural control and gait (body sway area and comfortable velocity) correlate with the muscular deficits. In addition, the assessment of subgroups through our two standardized laboratory tasks provides complementary information. The influence of the muscular deficit on these functional abilities depends on the required strength level to achieve these motor tasks. Indeed, postural control, which does not require much strength, is not affected when a weak deficit is present. In contrast, the muscular force deficiency affects gait, which requires a higher strength level.
Interestingly, additional insights are provided by the correlation analysis. The muscular strength of plantar-flexors is significantly linearly correlated with postural control, but only along the ML axis, while the activity of these muscles is mainly known to achieve AP postural control (13). However, classifying patients according to their level of muscular deficit shows that patients with CMT all have disturbed AP control, while only patients with severe muscular deficit have difficulty controlling their posture along the ML axis. Considering that the subjects’ feet are in an exorotation position, one can suggest that plantar-flexors muscles are also involved (as a complement to hip muscles) (13) in the lateral postural control (14). Dissociating data along the ML and AP axes thus allows the identification of different postural strategies in patients with CMT. In accordance with a previous study, gait cycle division remained normal in patients with CMT, whereas all other gait parameters are impaired (6), inducing a lower comfortable gait velocity (5). In spite of a significant difference in strength levels in dorsal-flexor muscles, no consequence was found during the foot strike between the two groups of patients. Therefore, the strength difference in dorsal ankle muscles appears to be too small to significantly influence this gait pattern phase. Finally, a limitation of this study is that the protocole inversor and eversor muscles were not assessed.
In conclusion, classifying patients into subgroups avoids the problem of items’ precision of the clinical scale, which can disrupt the interest of the correlation analysis, and thus highlight other postural control and gait strategies. As shown by the present data, clinical tests appear partially appropriate to inform about functional consequences, and thus justify their use in parallel with standardized laboratory tasks. Indeed, the assessment of basic movements that mobilize only one joint (as in the MRC scale) is poorly representative of complex tasks requiring muscular coordination. In this study the elucidation of the relationships between muscular deficits and certain functional abilities constitutes the main finding. Our data highlight that various muscular deficits in CMT disease contribute to functional differences during various motor tasks assessed through standardized analyses. Eventually, this finding should be useful, for example, in choosing optimal bracing to provide appropriate assistance. Indeed, when prescribed, the choice of the model of ankle-foot orthoses is often enough confusing. However, it is clear that the specific mechanical characteristics of orthoses must compensate appropriately for muscular deficit by restoring motor function without restraining the preserved abilities.
References

