Susanne Guidetti, PhD1, Charlotte Ytterberg, PhD1,2,7, Lisa Ekstam, PhD1,3, Ulla Johansson, PhD1,4 and Gunilla Eriksson, PhD1,5,6
From the 1Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, 2Department of Neurobiology, Care Sciences and Society, Division of Physiotherapy, Karolinska Institutet, 3Department of Occupational Therapy, Karolinska University Hospital, Stockholm, 4Centre for Clinical Research, Uppsala University/County Council of Gävleborg, 5Department of Speech Pathology, Physiotherapy and Occupational Therapy, University Hospital, 6Department of Public Health and Care Sciences, Research in Disability and Habilitation, Uppsala University, Uppsala and 7Department of Neurology, Karolinska University Hospital, Stockholm, Sweden
OBJECTIVE: To examine data collected using the Stroke Impact Scale 3.0 (SIS) at 3 and 12 months post-stroke, and to explore any clinically meaningful changes in everyday life in relation to age, gender and stroke severity.
DESIGN: Prospective longitudinal study.
METHODS: A total of 204 persons were assessed using the SIS at 3 and 12 months after onset of stroke. Changes in domain scores were calculated over time and in relation to age, gender and stroke severity.
RESULTS: The Strength, Hand Function and Participation domains had the highest perceived impact at 3 and 12 months, indicating problems in everyday life. Stroke recovery was perceived to be significantly higher at 12 than at 3 months irrespective of stroke severity, age or gender. The impact on the Strength and Emotion domains was significantly lower at 12 months than at 3 months. Most clinically meaningful changes, both positive and negative (± 15 points), were seen in the Participation domain and in Stroke recovery. Few changes were associated with age, gender or stroke severity.
CONCLUSION: Both positive and negative clinically meaningful changes related to impact of stroke were found between 3 and 12 months post-stroke. Therefore it is important to pay close attention to patients’ perceptions of their everyday life situation during rehabilitation and at discharge.
Key words: stroke; Stroke Impact Scale; rehabilitation; longitudinal study.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Susanne Guidetti, Division of Occupational Therapy, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Box 23 200, SE-141 83 Huddinge, Sweden. E-mail: susanne.guidetti@ki.se
Accepted May 6, 2014; Epub ahead of print Sep 3, 2014
INTRODUCTION
Stroke is a serious event that impacts significantly on many aspects of an individual’s life. Rehabilitation interventions are commonly delivered within the first 3 months after stroke onset. However, persons with stroke and their families perceive restrictions in functioning in everyday life for a considerable period of time after stroke (1, 2). The need for rehabilitation is not always fulfilled by 12 months (3–6). In a Swedish survey, almost half of the study population (n = 13,159) still reported problems in activities of daily living (ADL) 1 year after stroke, indicating a need for rehabilitation interventions that focus on decreasing the impact of stroke in everyday life (3). There is limited information on how persons perceive the impact of stroke at different time-points over the first year post-stroke. There is a need for better understanding of perceived change over time in order to deliver individualized rehabilitation interventions with appropriate timing (7).
The perceived impact of stroke can be measured with the Stroke Impact Scale 3.0 (SIS), a self-report instrument developed from the perspective of, and with input from, people with stroke and their caregivers as well as health professionals with stroke expertise (8). The SIS is designed to assess physical aspects and dimensions of health-related quality of life: emotion, communication, memory and thinking, and social role function (9), and covers perceptions by the individual with stroke on everyday functioning in 8 domains. It has proved valid, reliable and useful in describing changes after stroke (8, 10).
Several studies have used the SIS to explore the impact of stroke, but few studies have focused on the perceived impact of stroke at different time-points after stroke. One previous study, which used the SIS at 1, 3 and 6 months after stroke, found that people who had had minor strokes perceived less impact than those with moderate strokes in all domains except Emotion, and that the perceived impact of stroke was less at 3 and 6 months irrespective of whether they had experienced a minor or a moderate stroke (9).
Studies reporting the perceived impact of stroke at 1 time-point after stroke are more common. A study by Lai et al. (11) found that persons with stroke with a high level of recovery still perceived that the stroke impacted on the domains: Hand Function, Activities of Daily Living/Instrumental Activities of Daily Living (ADL/IADL), Strength, Mobility and Participation, 3 months after onset (11). Follow-up studies 1 year or more post-stroke showed that the domains: Hand Function, Strength (12, 13) and Participation (14) had the highest perceived (negative) impact on everyday life. Stroke recovery is seen as a function of the domain scores (9). In a Swedish sample, Hand Function and Emotion had the greatest impact on how stroke recovery was perceived at 1 year after onset for those of working age, while for the older group Participation, Communication and Hand Function had the largest impact on how stroke recovery was perceived (15). A strong positive correlation was found between ability to walk and high domain scores (indicating fewer problems in everyday life) in 4 of the 8 domains in the SIS: Strength, Mobility, ADL and Participation in a follow-up sample with a mean time of 5 years post-stroke (14).
In summary, most studies have explored the impact of stroke using the SIS on a single occasion. Hand Function, Strength and Participation are perceived as the most affected domains, even in the long-term. However, no studies have used established instruments to explore the change in impact from the individuals’ perspective over the first year after stroke. Information about which physical aspects and dimensions of health-related quality of life are impacted at different time-points is necessary in order to develop rehabilitation interventions. It is therefore necessary to follow people with stroke prospectively during the first year after onset. Information about the perceived impact of stroke may be useful in individualizing the rehabilitation provided.
The aims of this study were to examine data collected using the SIS at 3 and 12 months post-stroke, and to explore any clinically meaningful changes in everyday life in relation to age, gender and stroke severity.
METHODS
Data were collected in the context of a prospective observational study of the rehabilitation process after stroke: Life After Stroke phase I (LAS I). All subjects with a stroke diagnosis, verified by computed tomography, who were admitted to the stroke units at the Karolinska University Hospital, Stockholm, Sweden during a 1-year period, from 15 May 2006 to 14 May 2007 were eligible for the LAS I study. Participants were provided with written and oral information about the study and were included after giving their informed consent. In addition, they were asked to select a significant other (partner/relative/friend), who was then informed about the study and asked to participate. If use of the SIS proxy version was considered necessary, based on an evaluation of the level of cognitive and/or communicative impairments that limited the ability of patients to provide self-reports, their significant other was given written and oral information about the study and was invited to participate.
Information on the health of the persons with stroke was extracted from the medical records at inclusion into the study, i.e. 2–3 days after stroke onset. The remaining data collection was conducted via structured face-to-face interviews in the clinic or in the participants’ homes. The interviews were performed by specially trained research assistants (experienced occupational therapists and physiotherapists) at baseline and at 3 and 12 months after onset. The research assistants interviewed the participating significant others/proxies at the same time-points.
Instrument
Cognitive function at baseline was assessed with the Mini-Mental State Examination (MMSE) (16). ADL was assessed with the Barthel Index (BI) (17) and the BI scores at inclusion were used to determine stroke severity (18). BI scores of 100–50 signified a mild stroke; 49–15 a moderate stroke; and ≤ 14 a severe stroke.
The SIS 3.0 was used at 3 and 12 months to assess the perceived impact of stroke, comprising 59 items and representing 8 domains, including Strength, Memory and Thinking, Emotions, Communication, ADL/IADL, Mobility, Hand Function, and Participation (8, 10). As an example, the SIS Participation domain has 8 questions that ask the participant to rate how much of the time he or she has been limited in the past 4 weeks in: (i) work (paid, voluntary, or other), (ii) social activities, (iii) quiet recreation, (iv) active recreation, (v) role as a family member and/or friend, (vi) participation in spiritual or religious activities, (vii) ability to control life as you wish, and (viii) ability to help others (19). The responses to each question in the 8 domains are scored on a scale of 1 to 5. Aggregated scores are generated, and the higher the score (0–100) the less impact (fewer problems in everyday life) is perceived. The SIS also includes 1 item, presented in the form of a vertical visual analogue scale (VAS), that assesses overall stroke recovery, ranging from 0 = ”no recovery” to 100 = ”full recovery”. The 8 domains in the instrument have high reliability, with Cronbach alphas ranging from 0.83 to 0.90 and inter-class correlation coefficients (ICC) ranging from 0.70 to 0.92. An exception is the Emotion domain, which has ICC = 0.57 (9). The SIS has been extensively tested and there is validity evidence of high internal consistency in the 8 domains (8). Further concurrent (9) and construct validity has been established (20). A possible ceiling effect has been found for people with mild stroke in the Strength, (9) Emotion, Communication and Memory (8) domains.
To assess the perceived impact of stroke in individuals with severe stroke a proxy version was developed, since there is a risk that persons with major cognitive and communicative impairments after stroke will be excluded from evaluations. The SIS proxy version has proved able to provide valid information with small observed biases that were not clinically meaningful (21). Agreement between the persons with stroke and the proxies has been shown to be acceptable in most of the SIS domains (21).
Changes in the SIS domain scores of approximately 10–15 points appear to represent reasonable definitions of a clinically meaningful change (9). In the present study, we considered it to be a positive clinically meaningful change in scores when the difference in domain score was +15 points or more; no change when the difference was between –14 and +14; and a negative clinically meaningful change when the difference in score was –15 or lower (9).
Data analysis
Descriptive statistics were used to describe the study sample concerning stroke severity, age and gender.
Firstly, aggregated scores in each domain were generated (12) using the algorithm ( = [mean–1/5–1] × -100). If a participant responded to < 50% of the questions in a domain, the domain score was assigned as missing (9). In analyses of the whole sample, Wilcoxon’s matched pairs test was used to calculate changes in domain scores between 3 and 12 months. The same test was used to calculate changes in domain scores in relation to age groups (divided by median age), gender and stroke severity at stroke onset, based on the BI scores (18) (mild vs moderate/severe stroke) in the domains with statistically significant differences in domain scores over time.
Secondly, the participants were sorted into 3 groups according to the changes in their domain scores between 3 and 12 months, i.e. those with clinically meaningful positive change (+15 points or more); clinically meaningful negative change (–15 and lower); and no change (–14 to +14). These clinically meaningful positive or negative changes over the year were analysed in relation to gender and stroke severity by testing for differences between those with clinically meaningful positive changes and those with no change, and between those with negative changes and those with no change, using the χ2 test. The clinically meaningful positive or negative changes were also analysed in relation to age, using the Mann-Whitney U test.
RESULTS
The study sample is shown in Fig. 1. Of the 349 individuals who were included in the LAS I study, participants in the present study consisted of the 204 persons who responded to the SIS at 3 and 12 months post-stroke. Participant’s characteristics are shown in Table I. Their mean age was 70 years and 57% of the sample were men. Of the participants, 66% had a mild stroke; 21% a moderate stroke, and 13% a severe stroke. In the sample, 80% were born in Sweden, and 68% had no aphasia. All but 10 of the participants responded to the SIS by themselves. For 10 persons (9 women, 1 man) the impact of stroke was reported by a significant other using the SIS proxy version (4 partners, 1 sister, 2 daughters, 2 sons and 1 by the patient and the staff together).
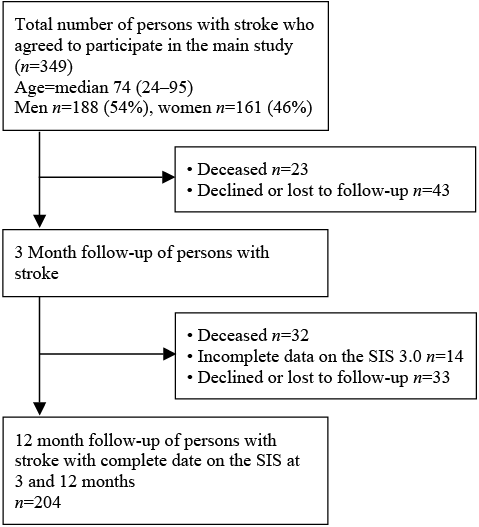
Fig. 1. The study sample. SIS: Stroke Impact Scale 3.0.
|
Table I. Participants’ characteristics (n = 204) |
||
|
Variables |
Valid, n |
|
|
Male/female, n (%) |
116 (57)/88 (43) |
204 |
|
Age years; mean (SD)/median (range) |
70 (14)/72 (24–93) |
204 |
|
Civil status, n (%) Married/cohabiting Single Other, e.g. lives with children, lives alone but has a partner |
116 (57) 74 (36) 12 (6) |
202 |
|
Born in Sweden, yes/no, n (%) |
164 (80)/34 (17) |
198 |
|
Education, n (%) Compulsory school, 7–16 Upper secondary school, 16–19 University |
84 (41) 46 (22.5) 51 (25) |
181 |
|
Stroke severity, n (%) Mild Moderate Severe |
135 (66) 42 (21) 27 (13) |
204 |
|
MMSE, mean (SD) |
29 (17) |
168 |
|
Aphasia, n (%) No aphasia Limited vocabulary/incoherent speech More than ”yes/no”, but no longer sentences Only ”Yes/No” or less |
135 (68) 39 (20) 15 (8) 9 (5) |
199 |
|
Type of stroke, n (%) Ischaemic Haemorrhagic |
170 (83) 34 (17) |
204 |
|
Localization of stroke, n (%) Left hemisphere Right hemisphere Unspecifieda |
86 (42) 85 (42) 30 (15) |
201 |
|
Barthel Index, mean/median (IQR) at inclusion |
67/85 (60) |
204 |
|
Barthel Index, mean/median (IQR) at 3 months |
87/100 (15) |
203 |
|
Barthel Index, mean/median (IQR) at 12 months |
90/100 (15) |
204 |
|
aFor example, cerebral infarction-unspecified, deep inter-cerebral haemorrhage, haemorrhage with multiple locations. MMSE: Mini-Mental State Examination; IQR: interquartile range; SD: standard deviation. |
||
Impact of stroke
The perceived impact of stroke in the total sample at 3 and 12 months, as reported in the SIS, is shown in Table II.
The domains Strength, Hand Function and Participation had the lowest mean scores at 12 months. When examining the impact of stroke, statistically significant positive changes in 2 domains had occurred between 3 and 12 months in the Strength domain (p < 0.05) and in the Emotion domain (p = 0.001). For the Strength domain, participants with mild stroke reported no change, but participants with moderate/severe stroke reported a positive change (p = 0.007), as did the younger age group (p = 0.02), but there was no statistically significant change in the domain score in the older age group, either in men or in women. Differences with regard to stroke severity, age and gender were analysed separately. Regarding the Emotion domain there were statistically significant positive changes for those with mild stroke (p = 0.012); statistically significant positive changes were also recorded for those with moderate/severe stroke (p = 0.035), in the younger (p = 0.028) and in the older age group (p = 0.016), for men (p = 0.007), but not for women.
Furthermore, the ratings on Stroke recovery (VAS 0–100) were significantly higher at 12 than at 3 months (p < 0.001) (shown in Table II) regardless of stroke severity, age or gender. There were however, no statistically significant changes over time in the total sample in the domains: Memory, Communication, ADL/IADL, Mobility, Hand Function and Participation.
|
Table II. Impact of stroke at 3 and 12 months in the Stroke Impact Scale 3.0 (SIS) domains and changes in impact between time-points (Wilcoxon’s matched pairs test) (n = 204) |
||||
|
SIS domains |
Valid, n 3/12 months |
Domain score |
Changes 3/12 months p-value |
|
|
3 months Mean (SD) |
12 months Mean (SD) |
|||
|
Strength |
201/203 |
69 (27) |
71 (26,9) |
0.045* |
|
Memory |
201/202 |
80.7 (20.9) |
81.1 (22.2) |
0.29 |
|
Emotions |
197/193 |
73.5 (17.7) |
77.6 (17.4) |
0.001* |
|
Communication |
202/203 |
85.1 (21.2) |
85 (21) |
0.96 |
|
ADL/IADL |
201/204 |
74.6 (26.7) |
75 (28.5) |
0.25 |
|
Mobility |
201/204 |
75.6 (28.1) |
75.6 (29.2) |
0.5 |
|
Hand function |
194/199 |
67.1 (35.5) |
68.9 (34.5) |
0.09 |
|
Participation |
201/201 |
67.7 (26.8) |
70.3 (27.5) |
0.09 |
|
Stroke recovery |
196/198 |
61.3 (25.7) |
68.4 (25.5) |
< 0.001* |
|
*p < 0.05. SD: standard deviation; ADL: activities of daily living; IADL: instrumental activities of daily living. |
||||
Clinically meaningful change in impact of stroke
The changes within the SIS domains between 3 and 12 months post-stroke and how these changes are distributed in the 3 groups, i.e. positive, negative or no clinically meaningful change, are shown in Table III. In the Strength and Participation domains > 20% of the participants had a clinically meaningful positive change, while, in the same domains, there were also high proportions of clinically meaningful negative change. A high proportion of clinically meaningful negative change was also reported in the Hand Function domain.
|
Table III. Changes in the Stroke Impact Scale 3.0 (SIS) domains between 3 and 12 months and distribution of participants in the 3 groups: positive, negative and no clinically meaningful change |
|||||
|
SIS-domains |
Valid, n |
Range in domain score changes between 3 and 12 months |
Positive change > +15 n (%) |
Negative change < –15 n (%) |
No change –14 to +14 n (%) |
|
Strength |
200 |
–100.0 to +62.5 |
47 (23) |
30 (14.7) |
123 (60.3) |
|
Memory |
200 |
–92.8 to +50.0 |
24 (11.8) |
20 (9.8) |
156 (76.5) |
|
Emotions |
189 |
–36.1 to +47.2 |
33 (16.2) |
16 (7.8) |
140 (68.6) |
|
Communication |
201 |
–100.0 to +42.9 |
17 (8.3) |
17 (8.3) |
167 (81.9) |
|
ADL/IADL |
201 |
–62.5 to +45.0 |
30 (14.7) |
19 (9.3) |
152 (74.5) |
|
Mobility |
201 |
–88.9 to +72.2 |
19 (9.3) |
18 (8.8) |
164 (80.4) |
|
Hand function |
193 |
–62.5 to +85.0 |
37 (18.1) |
29 (14.2) |
127 (62.3) |
|
Participation |
199 |
–65.6 to +60.4 |
56 (27.5) |
41 (20.1) |
102 (50) |
|
Stroke recovery |
192 |
–13.5 to +90.0 |
60 (29.4) |
21 (10.3) |
111 (54.4) |
|
ADL: activities of daily living; IADL: instrumental activities of daily living. |
|||||
The distribution of stroke severity, age and gender in the groups with positive, negative or no clinically meaningful change is shown in Table IV. Few statistically significant differences in clinically meaningful change were found regarding age and stroke severity when comparing the groups with clinically meaningful positive or negative changes with the group with no clinically meaningful change. These differences are presented in Table IV. The groups showing clinically meaningful negative changes in the Strength, Communication, ADL and Participation domains were significantly older. The groups with clinically meaningful positive changes in Strength, ADL, Mobility, Communication and Memory had a greater proportion of participants with moderate/severe stroke than the group with no change. The group with clinically meaningful negative change in Participation also had a greater proportion of participants with moderate/severe stroke than the group with no change. Regarding gender, no significant differences were found.
|
Table IV. Proportions of stroke severity, gender and median age in the 3 groups and statistically significant changes between the groups with positive and negative clinically meaningful change, compared with the group with no change (n = 204) |
|||||
|
Domain |
Positive change |
Positive change p-value |
Negative change |
Negative change; p-value |
No change |
|
Stroke severity: mild/moderate + severe |
|||||
|
Strength |
25/22 |
0.04* |
21/9 |
0.99 |
86/37 |
|
Memory |
12/12 |
0.04* |
11/9 |
0.14 |
111/45 |
|
Emotions |
22/11 |
0.89 |
13/3 |
0.39 |
95/45 |
|
Communication |
7/10 |
0.02* |
13/4 |
0.59 |
114/53 |
|
ADL/IADL |
13/17 |
0.003* |
11/8 |
0.21 |
109/43 |
|
Mobility |
5/14 |
< 0.001* |
10/8 |
0.15 |
118/46 |
|
Hand function |
21/16 |
0.09 |
19/10 |
0.51 |
91/36 |
|
Participation |
35/21 |
0.15 |
23/18 |
0.04* |
75/27 |
|
Stroke recovery |
36/24 |
0.08 |
14/7 |
0.56 |
81/30 |
|
Age, median, years |
|||||
|
Strength |
73 |
0.67 |
77 |
0.013* |
70 |
|
Memory |
72 |
0.80 |
73 |
0.91 |
72 |
|
Emotions |
69 |
0.74 |
71 |
0.80 |
72 |
|
Communication |
77 |
0.16 |
78 |
0.04* |
71 |
|
ADL/IADL |
68 |
0.51 |
78 |
0.05* |
72 |
|
Mobility |
67 |
0.73 |
77 |
0.20 |
72 |
|
Hand function |
67 |
0.11 |
79 |
0.07 |
71 |
|
Participation |
65.5 |
0.06 |
78 |
0.04* |
71 |
|
Stroke recovery |
72.5 |
0.13 |
76 |
0.10 |
70 |
|
Gender, male/female, % |
|||||
|
Strength |
60/40 |
0.61 |
60/40 |
0.64 |
55/46 |
|
Memory |
58/42 |
1.00 |
50/50 |
0.48 |
58/42 |
|
Emotions |
61/39 |
0.61 |
69/31 |
0.34 |
56/44 |
|
Communication |
59/42 |
0.95 |
53/47 |
0.68 |
58/42 |
|
ADL/IADL |
57/43 |
0.95 |
58/42 |
0.96 |
57/43 |
|
Mobility |
68/32 |
0.35 |
44/56 |
0.30 |
57/43 |
|
Hand function |
65/35 |
0.29 |
45/55 |
0.32 |
55/45 |
|
Participation |
66/34 |
0.17 |
54/46 |
0.89 |
55/45 |
|
Stroke recovery |
55/45 |
0.74 |
57/43 |
0.97 |
58/42 |
|
*p < 0.05. ADL: activities of daily living; IADL: instrumental activities of daily living. |
|||||
DISCUSSION
This is the first study to describe how persons with stroke rate their perceived impact of stroke and the change in impact between 3 and 12 months post-stroke according to the SIS. The most impacted domains (lowest domain scores) at 3 and 12 months were Strength, Hand Function and Participation. In the total sample, there were statistically significant positive changes, albeit rather small changes in absolute numbers, in the Strength and Emotion domains between 3 and 12 months, as well as in Stroke recovery. With regard to clinically meaningful changes in the 8 different domains, similar proportions of subjects (Table III) perceived lower (fewer problems) or higher impact (more problems) of stroke at 12 months compared with impact at 3 months. The highest frequency of clinically meaningful changes, both positive (problems had decreased from 3 to 12 months) and negative (problems had increased from 3 to 12 months), was found in the Participation domain.
Impact of stroke
There are few studies reporting the impact of stroke using the SIS at 1 year or more after stroke onset. Stroke recovery was rated significantly higher at 12 months than at 3 months in the total sample, irrespective of stroke severity, age or gender. Higher scores in Stroke recovery at 3 and 6 months, compared with scores 1 month after stroke onset, were also reported by Duncan et al. (9).
The most impacted domains (more perceived problems) at both 3 and 12 months were Strength, Hand Function and Participation, which is in accordance with results from other stroke samples using the SIS (11, 13, 15, 17, 22). The Strength domain, however, was also 1 of the 2 domains that had statistically significant positive changes in scores over the year in the total sample, and among participants with moderate/severe stroke. One possible reason for this positive change over time among people with moderate/severe stroke is that they had more scope for improvement over time. It is likely that the participants with mild stroke reported higher scores in the Strength domain at 3 months than the participants with moderate/severe stroke, which might make a positive change impossible at the second time-point on account of a ceiling effect in the instrument. These results are in agreement with those of Duncan et al. (9), who showed a positive change between 1 and 6 months after stroke, which was greater in those with moderate stroke compared with those with mild stroke. The study by Duncan et al. (9) provides support for a possible ceiling effect in the Strength domain for individuals with mild stroke, and a later study also found a ceiling effect for individuals with mild stroke in the domains of Emotion, Communication and Memory (8).
Clinically meaningful change in impact of stroke
As this is the first study to explore clinically meaningful change in impact in all domains over the first year after stroke it is not possible to make comparisons with other studies. In the various SIS domains, we found that between 8% and 27.5% of the sample perceived positive or negative clinically meaningful changes. The Participation domain had high proportions of both positive (27.5%) and negative clinically meaningful change (20%). Those who had a negative change in the Participation domain were significantly older and had a higher proportion of moderate/severe stroke than the group with no change. There were no differences regarding gender. The fact that almost half of the study sample had a clinically meaningful positive or negative change in the Participation domain over the first year implies that this domain is sensitive to the impact of stroke on individuals over time, both in positive and negative directions. Furthermore, it indicates that taking part in social, recreational and productive activities, as well as maintaining one’s social role and control over one’s life are perceived to be important and are essential ingredients in the planning of rehabilitation interventions. However, recent studies measuring the effects of rehabilitation intervention found contradictory results in the responsiveness of the Participation domain in the SIS (23–25).
Two-thirds of the participants in the study sample had sustained a mild stroke and it might be reasonable to believe that they, in general, perceived less impact of stroke than those who had a more severe stroke, even at 3 months after stroke. Almost all stroke recovery occurs in the first 3 months after stroke onset (9), but recovery takes longer for those with severe stroke (26). Nevertheless, the findings in this study indicate that the perceived impact of stroke also changes after 3 months, and the positive changes in the Strength, Memory, Communication, ADL and Mobility domains imply that clinically meaningful changes were seen mostly for participants with moderate/severe strokes. However, knowledge is limited regarding when and for how long after the first 3 months perceived change in impact of stroke occurs. A clinical implication that can be derived from this result is that clients with moderate/severe stroke might need follow-up and rehabilitation interventions with appropriate timing beyond the subacute phase.
Forty percent of the study sample changed their ratings on Stroke recovery by + or –15 points between 3 and 12 months. Stroke recovery, which is seen as a function of the domain scores, has been shown to be predicted by the physical aspects of disability and Emotion and Participation domain scores (9). Of those domain scores, the Participation score was the one in the present study that changed similarly to the Stroke recovery ratings concerning proportions of both positive and negative clinically meaningful change. Stroke recovery, together with the Hand Function domain score, has been proven to have medium responsiveness to changes during a 3-week rehabilitation intervention provided for people 17 months after stroke onset, and it is recommended that it be used to measure outcome of rehabilitation (23). The findings of the present study indicate that Stroke recovery together with the Participation domain might be the most responsive of the ratings in the SIS over the first year, since between 40% and almost 50% of the participants appeared to have clinically meaningful changes in these areas. This result supports the clinical use of the SIS Stroke recovery and the Participation domain to both grasp the perceptions of the individual impact of the stroke and to tailor future interventions. However, further research is needed to explore the responsiveness of the SIS in larger samples and over longer time periods.
Study limitations
There are issues that limit the generalizability of the findings of this study to the broader population of all individuals with stroke. As emphasized earlier, 66% of the sample consisted of people with mild stroke. It is reasonable to consider that people with very mild, as well as those with severe stroke may be underrepresented, as those with very mild stroke are discharged after a very short stay and those with severe stroke might have a condition too poor for it to be appropriate to ask them to participate in the study. Another issue is the limitations in the SIS assessment regarding ceiling effects in some of the domains. These effects are related to stroke severity (8, 9) and, as the study sample consisted of a majority of people with mild stroke, it is likely that these ceiling effects have influenced the result.
Clinical implications
The SIS is more sensitive than other outcome measures (23) when used to measure change after rehabilitation. In order to be patient-centred, an instrument has to reflect patient priorities (27), and the SIS does that more than other instruments (28), although Tistad et al. identified that the SIS did not capture some categories of experienced problems, such as fatigue and performing activities of daily living, e.g. using transport and driving, in a sample 3 months after stroke (28). Based on the results, the SIS domain Participation and Stroke recovery is suggested for use in the clinical context after the acute phase as a basis for rehabilitation planning and, later on, for evaluation of the rehabilitation provided.
In conclusion, both positive and negative clinically meaningful changes occur in people with stroke during the period between 3 and 12 months post-stroke. These changes, even if they are not perceived by the majority of this sample, predominantly affected by mild stroke, indicate the need to carry out follow-up and provide rehabilitation interventions, at least for people with moderate/severe stroke. Furthermore, this study indicates the need for individualized rehabilitation interventions, based on activities that the individual wants to resume and in social situations in which they will continue to participate.
ACKNOWLEDGEMENTS
This work was financed by grants from: Karolinska Institutet, Centre for Health Care Science, Karolinska University Hospital, ALF, the regional agreement on medical training and clinical research between Stockholm County Council and Karolinska Institutet, Solstickan Foundation, and The Swedish Association of Occupational Therapists in Stockholm, Sweden.
The authors would like to thank the patients and their caregivers who participated in this study.
REFERENCES

