Matthew A. Plow, PhD1, Marcia Finlayson, PhD, OT Reg (Ont), OTR2, Douglas Gunzler, PhD3 and Allen W. Heinemann, PhD4
From the 1Frances Payne Bolton School of Nursing, Case Western Reserve University, Cleveland Clinic Lerner Research Institute, Cleveland, USA, 2School of Rehabilitation Therapy, Queen’s University, Kingston, Ontario, Canada, 3School of Medicine, Case Western Reserve University, Cleveland and 4Feinberg School of Medicine, Department of Physical Medicine and Rehabilitation, Northwestern University and Rehabilitation Institute of Chicago, Chicago, USA
OBJECTIVE: To explore the associations between impairments, self-management self-efficacy, self-management behaviors, and environmental factors and their role in predicting participation in meaningful activities among people with multiple sclerosis.
DESIGN: Online cross-sectional survey.
SUBJECTS/PATIENTS: Randomly selected individuals (n = 335) from a large multiple sclerosis patient registry.
METHODS: Participation in activities that are meaningful to the individual was measured with Community Participation Indicators (CPI), the dependent variable. Independent variables included symptom severity, activities of daily living limitations, cognitive problems, stages of change for physical activity, nutritional behaviors, self-efficacy, and environmental barriers. A backwards selection regression analysis was used to compare the relative contributions of independent variables in predicting the CPI. A path analysis was conducted to explore the associations between independent variables and their direct and indirect effects on the CPI.
RESULTS: The final regression model included self-management self-efficacy (β = 0.12), environmental barriers (β = –0.16), cognitive problems (β = –0.22), and stages of change for physical activity (β = 0.12). Path analysis indicated that impairments and environmental barriers might negatively influence self-management self-efficacy. Self-management self-efficacy might have indirect effects on the CPI via engagement in self-management behaviors.
CONCLUSION: Future research should explore whether interventions that promote self-management self-efficacy can facilitate participation in meaningful activities.
Key words: multiple sclerosis; social participation; International Classification of Functioning, Disability and Health; self care; regression analysis.
J Rehabil Med 2015; 47: 538–545
Correspondence address: Matthew Plow, Frances Payne Bolton School of Nursing Case Western Reserve University, 10900 Euclid Avenue, Frances Payne Bolton School of Nursing, Cleveland, OH, USA. E-mail: map208@case.edu
Accepted Nov 19, 2014; Epub ahead of print May 5, 2015
INTRODUCTION
Multiple sclerosis (MS) is a disabling immune-mediated disease of the central nervous system. Progression and symptom manifestation are unpredictable and existing medical treatments are only partially effective in slowing impairments caused by de-myelination of nerves (1). Common MS symptoms, such as fatigue, mobility impairments, and cognitive problems, can negatively impact on many aspects of daily life and can present challenges to engaging in activities that help maintain independence and provide a sense of meaning and autonomy (2). MS symptoms can make it difficult to engage in self-management behaviors (e.g. physical activity and healthy eating) that are important in preventing comorbidities and functional decline. Individuals with moderate to severe symptoms of MS may routinely have to prioritize self-care activities and daily chores over leisure and social activities, which can have detrimental effects on quality of life (3). Indeed, an important goal in rehabilitation is promoting full participation in life roles or involvement in all meaningful activities and situations (4).
According to the International Classification of Functioning, Disability and Health (ICF), participation restrictions are an outcome of the disease process and the complex interactions between personal factors, environmental contexts, impairments, and activity limitations (5). Unfortunately, the ICF framework provides little guidance to researchers and clinicians on which factors are most important to address in order to encourage full participation in life roles. Furthermore, research has been hindered by participation measures that are not adequately validated, narrowly focused, and/or do not account for differences in individual preferences about engaging in activities across different life roles (6, 7). Thus, many questions remain about the factors that influence participation. For example, are there modifiable psychological, behavioral, or environmental factors that a clinician can address to facilitate participation across different life roles that are meaningful to the patient? With the recent development of the Community Participation Indicators (CPI) by Heinemann and colleagues (8–10), it is now possible to explore such questions.
An important psychological factor in facilitating participation across different life roles might be self-management self-efficacy or confidence in managing symptoms to engage in activities as desired (11, 12). Self-efficacy refers to the belief that one can successfully cope with challenging conditions. If people judge themselves as capable of being able to manage symptoms and engage in activities as desired, there may be a greater likelihood that engagement in meaningful activities is repeated. Although research indicates that generalized self-efficacy is associated with health-related quality of life in MS (13), to date no studies have examined the association between self-management self-efficacy and participation across different life roles.
Self-management self-efficacy might also indirectly influence participation by facilitating engagement in self-management behaviors, such as routinely engaging in physical activity and healthy eating, communicating effectively with caregivers, and managing emotions. Routinely engaging in self-management behaviors might mitigate the negative impact of symptoms on daily activities in people with MS (14). For example, managing stress is associated with fewer exacerbations and routine physical activity is associated with improved health-related quality of life (15, 16). Increasing self-management self-efficacy might be a strategy for encouraging engagement in self-management behaviors, which in turn could help prevent participation restrictions.
Alternatively, environmental factors, such as the inaccessibility of transportation, healthcare services, and information, can create barriers to participating in life roles (17). Environmental barriers interacting with impairments and activity limitations might reduce self-efficacy, and may explain why people with the same level of impairments can function very differently (18). For example, 2 persons with the same moderate severity level of MS-related fatigue may or may not have difficulty participating in meaningful activities depending, for example, on whether their social support system enables them to delegate tasks and chores. Thus, it is important to account for environmental factors when exploring the factors associated with participation.
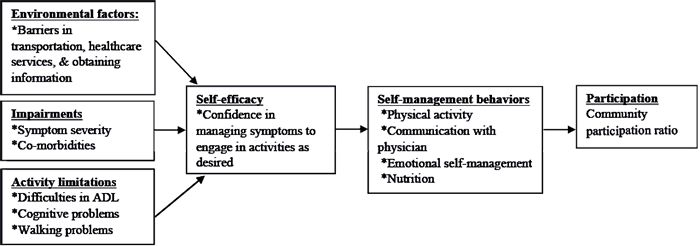
The aim of this study was to explore the associations between impairments, activity limitations, self-management self-efficacy, self-management behaviors, and environmental barriers and their role in predicting participation in activities that are meaningful to people with MS. Specifically, we examined bivariate correlations with the CPI, used multiple regression analysis to determine the relative importance of variables in predicting the CPI, and conducted a path analysis to explore the relationships between independent variables and their influence on the CPI (Fig. 1). Using path analysis, we explored 3 hypotheses: (i) that barriers created by the environment, impairments, and activity limitations negatively influence self-management self-efficacy; (ii) that self-management self-efficacy positively influences self-management behaviors; and (iii) that self-management behaviors positively influence the CPI.
Methods
Data were obtained from an online survey designed using SurveyMonkey. Individuals with MS (n = 1,000) were selected from the North American Research Committee on Multiple Sclerosis (NARCOMS) volunteer patient registry (http://narcoms.org/). A total of 1,000 randomly-selected recent responders to the NARCOMS registry were emailed a request to complete an online survey about their function and engagement in healthy behaviors. Participants were asked to complete the survey twice to obtain test-retest reliability data. A total of 335 individuals participated in the first survey (response rate 33.5%) and 165 individuals (response rate 49.2%) completed the second survey 8–12 weeks later. University of Illinois at Chicago review board approved this study.
Dependent measure
The dependent measure was the CPI, a new measure developed by Heinemann and colleagues with input from multiple stakeholders (8–10). It is validated through Rasch analysis in a sample of 1,163 individuals with a variety of disabling conditions. Analyses supported a measure with adequate spread and fit of items. For each item, respondents rated the frequency of engagement (either in days, hours, or times per week, depending on the activity type), whether it was important (yes/no), and to what extent they were doing it (too much, enough, or not enough). For the analysis, a ratio of the number of important activities engaged in often enough or too much (numerator) to the number of important activities (denominator) was calculated. A higher score (range between 0 and 1) indicates increased participation in activities across productive, social, and community roles that are meaningful to the individual. Frequency of activity was used for descriptive purposes only. Test-retest reliability over a 2.5-month period was good (∆ mean = < 0.01, σ = 0.16, p = 0.91; r = 0.84, p < 0.01).
Independent measures
Self-management self-efficacy. The 6-item Chronic Diseases Self-efficacy questionnaire (19) was used to assess confidence in preventing emotional distress and symptoms, such as fatigue and physical discomfort, from interfering with daily activities. A 10-point scale, ranging from not confident at all to completely confident, is used to rate questions. A higher score indicates increased confidence to self-manage stress and symptoms to engage in activities as desired. Internal test-retest reliability and internal consistency were good (∆ mean = 0.01, σ = 1.27, p = 0.91; r = 0.78, p < 0.01; α = 0.87).
Self-management behaviors. Included variables were stages of change for physical activity, communication with physicians, nutrition, and emotional management. Participants were categorized into stages of change for physical activity by a questionnaire developed by Marcus et al. (20, 21). The 5 stages of change (pre-contemplation, contemplation, preparation, action, and maintenance) reflect behavioral intentions and the temporal process from inactivity to routine engagement in physical activity. A higher score indicates increased readiness to engage in physical activity. Test-retest reliability was adequate for stages of change placement (∆ mean = 0.09, σ = 1.16, p = 0.31; r = 0.72, p < 0.01).
Healthy nutritional behaviors were measured using a previous survey among women with disabilities (22), which includes 5 questions about making good food choices, eating 5 servings of fruits and vegetables a day, limiting fat intake, reading labels, and eating regularly that are rated on a 3-point scale, ranging from never to frequently. A higher score indicates healthier nutritional behaviors. Test-retest reliability and internal consistency was adequate (∆ mean = 0.01, σ = 0.27, p = 0.48; r = 0.79, p < 0.01; α = 0.73).
The Communication with Physician questionnaire consisted of the following 3 questions on a 6-point scale, ranging from never to always (23): Do you prepare a list of questions for your doctor?; Do you ask questions about the things you want to know about and don’t understand?; Do you discuss any personal problems that may be related to your illness? A higher score indicates better communication with physicians. Test-retest reliability and internal consistency were adequate (∆ mean = 0.08, σ = 0.97, p = 0.30; r = 0.72, p < 0.01; α = 0.75).
Emotional management was measured with the Cognitive Symptom Management questionnaire (23), which asks 6 questions on a 6-point scale, ranging from never to always how often they use visualization and other distraction strategies to help manage their emotions. Questions include: “When you are feeling down in the dumps… (i) do you talk to yourself in a positive way, (ii) play mental games, (iii) practice progressive muscle relaxation?” A higher score indicates more frequent use of distraction strategies to manage emotions. Test-retest reliability and internal consistency were adequate (∆ mean = 0.04, σ = 0.70, p = 0.51; r = 0.71, p < 0.01; α = 0.77).
Environmental barriers. The Craig Hospital Inventory of Environmental Factors–Short Form (CHIEF-SF) was used to measure perceived barriers in the physical and social environment (24). Questions include: “In the past 12 months how often has… (i) the availability of transportation been a problem, (ii) the information you wanted or needed not been available in a format you can use or understand, and (iii) the availability of healthcare services and medical care been a problem for you.” Participants rate how often they experience the environmental barrier and whether it has been a big or small problem. A higher score indicates increased environmental barriers. Test-retest reliability for the CHIEF-SF was adequate (∆ mean = 0.10, σ = 0.69, p = 0.07; r = 0.79, p < 0.01).
Impairments. Indicators of impairments were a count of co-morbid conditions and symptom severity. The number of co-morbid conditions was a count in response to 15 common conditions, such as diabetes, arthritis, and heart problems. Test-retest reliability was good (∆ mean = 0.08, σ = 0.96, p = 0.32; r = 0.84, p < 0.01). Symptom severity was measured with the Symptoms of Multiple Sclerosis Scale (25), which measures the extent to which individuals experience fatigue, pain, visual impairments, paralysis, bladder difficulties, lack of concentration, inability to communicate, bowel difficulties, numbness, tremors, loss of balance, and spasticity on a 5-point scale, ranging from never to always. A higher score indicates increased symptom severity. Test-retest reliability was adequate (∆ mean = 0.28, σ = 3.22, p = 0.30; r = 0.94, p < 0.001; α = 0.83).
Activity limitations. Included variables were problems in walking and cognition, as well as limitations in activities of daily living. We use the 5-item Perceived Deficits Questionnaire (PDQ) to measure limitations in activities due to cognitive impairment (26). Participants are asked how often they have trouble getting things organized, forget the date, forget what was talked about after a phone conversation, and feel like their mind went totally blank on a 5-point scale, ranging from never to almost always. A higher score indicates increased cognitive problems. The PDQ showed adequate test-retest reliability and internal consistency (∆ mean = 0.05, σ = 2.12, p = 0.74; r = 0.91, p < 0.01; α = 0.91).
The Self-Reported Functional Measure assesses one’s perceived ability to perform daily activities (27). Participants were asked how much help they needed with such tasks as eating, moving around the house, dressing upper and lower body, grooming, transferring, and managing bladder and bowels. Participants rate these questions on a 5-point scale ranging from no extra time or help to total help or never do. A higher score indicates greater difficulty in accomplishing such tasks. Test-retest reliability and internal consistency were good (∆ mean = 0.03, σ = 0.91, p = 0.72; r = 0.70, p < 0.001; α = 0.97).
The MS Walking Scale was used to assess difficulty in walking (28). Participants used a scale of 1 (not at all) to 5 (extremely) to rate how much MS had caused problems with walking, running, and climbing stairs as well as perceptions about balance, smoothness and pace of walking and need for support while walking. A higher score indicates greater problems with walking. Test-retest reliability and internal consistency were good (∆ mean = 0.56, σ = 7.73, p = 0.36; r = 0.97, p < 0.001; α = 0.99).
Analysis
We conducted descriptive, distributional, bivariate correlations, multiple regression analysis, path analysis, and multiple imputations for missing data using SPSS version 21. Because online administration of the survey resulted in missing data from approximately 30% of participants, we tried to minimize selection bias and maximize power by using multiple imputations. Specifically, we used the fully conditional specification method available in SPSS; 100 imputed data sets were used and 60 data points were imputed for the CPI. Thus, we were able to use the full survey sample for analyses (n = 335). To examine potential biases, we compared results of the imputed dataset to the non-imputed dataset. A multiple linear regression analysis was used to examine the relative importance of variables in predicting the CPI. Variable selection was performed by using only significant bivariate correlates in a backwards elimination method. Using pooled estimates from multiple imputations, a p-value of 0.05 was selected for excluding independent variables.
Path analysis is used to answer questions about the relationships between independent variables and identify direct and indirect relationships with a dependent variable (29). Path models illustrate theoretical, hypothesized directional relationships. Path coefficients are calculated using a series of multiple regression analyses based on the hypothesized model. To evaluate our hypothesized model, only independent variables that had a significant bivariate correlation with the CPI were used in the analyses. Path coefficients were calculated by conducting the following 3 regression analyses: (i) self-management self-efficacy was regressed on impairments, activity limitations, and environmental barriers, (ii) self-management self-efficacy was regressed on self-management behaviors, and (iii) self-management behaviors were regressed on the CPI. Impairments, activity limitations, and environmental barriers were exogenous variables, whereas self-management self-efficacy and behaviors were endogenous variables. Based on recommendations to use normally distributed variables, minimize collinearity, and have at least 30 participants per independent variable (29, 30), we met statistical assumptions and the required number of participants to perform the analyses.
Results
Participants were mostly white (98.5%), upper middle-class (59.7% reporting an annual household income of over 50,000 USD), well educated (61.2% reporting more than 15 years of education) and women (79.7%). Mean age was 53.0 years (standard deviation (SD) 10.2) and years since diagnosis averaged 15.0 years (SD 8.3). Most participants reported having relapsing-remitting MS (63.0%), followed by secondary progressive (20.0%), primary progressive (8.1%), and progressive-relapsing (2.4%). The majority of participants used a mobility aid sometimes or always (59.7%). Results on the frequency of engagement in activities and the percent of participants who viewed activities as important and whether they were doing it enough is reported in Table I.
|
Table I. Descriptive statistics on participants’ activities |
||||
|
Activity |
Frequency % > none |
Important % |
Doing activity enough % |
Activity important & Doing activity enough % |
|
1. Get out and about |
96.1 |
91.9 |
65.0 |
61.0 |
|
2. Spend time with family |
86.8 |
91.6 |
65.3 |
60.4 |
|
3. Keep in touch with family by phone or internet |
94.5 |
93.2 |
72.2 |
67.0 |
|
4. Spend time with friends |
79.4 |
90.6 |
43.2 |
36.0 |
|
5. Keep in touch with friends by phone or internet |
93.9 |
91.2 |
67.5 |
61.0 |
|
6. Go to parties, out to dinner, or other social activities |
64.6 |
76.9 |
57.7 |
41.4 |
|
7. Spend time with a significant other or intimate partner |
79.4 |
88.1 |
60.6 |
54.0 |
|
8. Work for money |
52.6 |
68.0 |
62.1 |
35.8 |
|
9. Cook, clean, and look after your home |
93.2 |
84.4 |
57.8 |
50.7 |
|
10. Manage household bills and expenses |
87.7 |
87.6 |
85.2 |
74.3 |
|
11. Look after children or provide care for a loved one |
42.3 |
57.0 |
81.6 |
42.2 |
|
12. Go to classes or participate in learning activities |
40.0 |
64.6 |
62.8 |
32.6 |
|
13. Volunteer |
40.9 |
69.3 |
57.3 |
31.5 |
|
14. Participate in religious or spiritual activities |
46.3 |
58.2 |
84.6 |
31.7 |
|
15. Go to support groups or self-help meetings |
14.5 |
24.6 |
84.6 |
13.2 |
|
16. Engage in hobbies or leisure activities |
89.4 |
94.1 |
58.1 |
53.1 |
|
17. Go to movies, sporting events or entertainment events |
45.0 |
62.4 |
62.3 |
30.5 |
|
18. Participate in sports or active recreation |
64.0 |
79.9 |
49.7 |
35.6 |
|
19. Participate in community clubs or organizations |
25.1 |
39.3 |
77.7 |
23.4 |
|
20. Participate in civic or political activities |
17.2 |
28.7 |
83.6 |
18.5 |
Table II reports the means and standard deviations and Table III reports Pearson correlations between the CPI and the independent variables. Bivariate correlations indicated that the MS Walking Scale, number of co-morbid conditions, communication with physician, and limitations in activities of daily living were not associated significantly with the CPI. Self-management self-efficacy, environmental barriers, cognitive problems, emotional self-management behaviors, symptom severity, healthy nutritional behaviors, and stages of change for physical activity were associated significantly with the CPI.
|
Table II. Characteristics of research sample and variables considered for analysis |
||
|
|
Mean (SD) |
Possible range |
|
Dependent measure |
|
|
|
Community Participation Ratio |
0.61 (0.26) |
0–1 |
|
Impairments |
|
|
|
Symptoms of Multiple Sclerosis Scale |
19.33 (8.20) |
1–60 |
|
Number of co-morbidities |
1.19 (1.17) |
0–15 |
|
Activity limitations |
|
|
|
Self-Reported Functional Measure (ADL) |
6.42 (10.46) |
0–52 |
|
MS Walking Scale |
51.32 (36.15) |
0–100 |
|
Perceived Deficit Questionnaire |
2.95 (3.37) |
0–20 |
|
Self-management behaviors |
|
|
|
Stages of change for physical activity |
2.96 (1.54) |
1–5 |
|
Communication with physician |
9.17 (3.78) |
0–15 |
|
Emotional management |
6.82 (5.51) |
0–30 |
|
Nutritional behaviors |
7.46 (2.24) |
0–10 |
|
Environment |
|
|
|
CHIEF-SF |
0.95 (0.82) |
0–8 |
|
Self-efficacy |
|
|
|
Self-management symptoms |
41.13 (12.28) |
6–60 |
|
CHIEF-SF: Craig Hospital Inventory of Environmental Factors–Short Form; ADL: activities of daily living; SD: standard deviation. |
||
|
Table III. Correlation matrix (Pearson’s R) |
||||||||||||
|
|
Community Participation Ratio |
Symptoms of Multiple Sclerosis Scale |
Number of Co-morbidities |
Self-Reported Functional Measure (ADL) |
MS Walking Scale |
Perceived Deficit Questionnaire |
Stages of change for physical activity |
Communication with physician |
Emotional management |
Nutritional behaviors |
CHIEF-SF |
Self-management symptoms |
|
Community Participation Ratio |
1.00 |
|
|
|
|
|
|
|
|
|
|
|
|
Symptoms of Multiple Sclerosis Scale |
–0.243** |
1.00 |
|
|
|
|
|
|
|
|
|
|
|
Number of co-morbidities |
–0.10 |
0.236** |
1.00 |
|
|
|
|
|
|
|
|
|
|
Self-Reported Functional Measure (ADL) |
–0.03 |
0.270** |
0.02 |
1.00 |
|
|
|
|
|
|
|
|
|
MS Walking Scale |
–0.05 |
0.581** |
0.07 |
0.439** |
1.00 |
|
|
|
|
|
|
|
|
Perceived Deficit Questionnaire |
–0.354** |
0.526** |
0.280** |
0.02 |
112* |
1.00 |
|
|
|
|
|
|
|
Stages of change for physical activity |
0.225** |
–0.311** |
–0.196** |
–0.246** |
–0.389** |
–0.176** |
1.00 |
|
|
|
|
|
|
Communication with physician |
–0.01 |
0.133* |
0.04 |
0.06 |
0.07 |
0.02 |
0.05 |
1.00 |
|
|
|
|
|
Emotional management |
–0.176** |
0.315** |
0.143** |
–0.01 |
0.129* |
0.236** |
0.03 |
0.219** |
1.00 |
|
|
|
|
Nutritional behaviors |
0.159** |
–0.03 |
–0.132* |
–0.07 |
–0.04 |
–0.159** |
0.170** |
0.153** |
0.191** |
1.00 |
|
|
|
CHIEF-SF |
–0.308** |
0.393** |
0.222** |
0.136* |
0.277** |
0.375** |
–0.191** |
0.04 |
0.258** |
–0.07 |
1.00 |
|
|
Self-efficacy self-management symptoms |
0.306** |
–0.442** |
–0.268** |
–0.129* |
–0.198** |
–0.425** |
0.280** |
–0.130* |
–0.146** |
0.234** |
–0.340** |
1.00 |
|
*Correlation is significant at ≤ 0.05 level. **Correlation is significant at ≤ 0.01 level. CHIEF-SF: Craig Hospital Inventory of Environmental Factors–Short Form; ADL: activities of daily living. |
||||||||||||
Table IV reports the backwards selection regression model to identify the relative importance of variables. The final model included self-management self-efficacy, environmental barriers, cognitive problems, and stages of change for physical activity. Nutritional behaviors, symptom severity, and emotional self-management were tested for inclusion in the model, but did not explain enough variance in the CPI to make the final model. Increased environmental barriers and cognitive problems were associated significantly with decreased scores on the CPI, whereas greater self-management self-efficacy and higher stages of change placement for physical activity were associated significantly with increased scores on the CPI. Cognitive problems explained the most variance in the CPI, followed by environmental barriers and stages of change for physical activity, and self-efficacy self-management. The final model variables accounted for 19.4% of variance in the CPI. Due to the negative skewness (–0.234) of the CPI, we performed the same analyses with a log transformation and obtained similar results. Furthermore, as shown in Table IV, we obtained similar results using imputed and non-imputed data; i.e. regression coefficients were essentially unchanged, but the statistical precision may have been improved using the imputed dataset.
|
Table IV. Final backwards selection multiple regression model predicting community participation (considering all variables that had a significant bivariate correlation with Community Participation Indicators (CPI)) |
||||
|
Outcome variable |
R2 |
Predictor variables |
Standardized β |
p |
|
Participation (imputed dataset) |
0.19 |
Stages of Change for Physical Activity |
0.12 |
0.027 |
|
|
Environmental barriers |
–0.16 |
0.006 |
|
|
|
Self-efficacy self-management |
0.12 |
0.045 |
|
|
|
Cognitive problems |
–0.22 |
< 0.001 |
|
|
Participation (non-imputed dataset) |
0.20 |
Stages of Change for Physical Activity |
0.12 |
0.040 |
|
|
Environmental barriers |
–0.15 |
0.017 |
|
|
|
Self-efficacy self-management |
0.14 |
0.025 |
|
|
|
Cognitive problems |
–0.23 |
< 0.001 |
|
All path coefficients were statistically significant (Fig. 2). As hypothesized, increased environmental barriers (β = –0.15), cognitive problems (β = –0.23), and symptom severity (β = –0.26) negatively influenced self-management self-efficacy. Increased self-management self-efficacy negatively influenced the use of emotional self-management strategies (β = –0.20), but positively influenced stages of change placement for physical activity (β = 0.25) and engagement in healthy nutritional behaviors (β = 0.23). Higher stages of change placement for physical activity (β = 0.20), increased engagement in healthy nutritional behaviors (β = 0.17), and decreased use of emotional self-management strategies (β = –0.21) negatively influenced scores on the CPI.
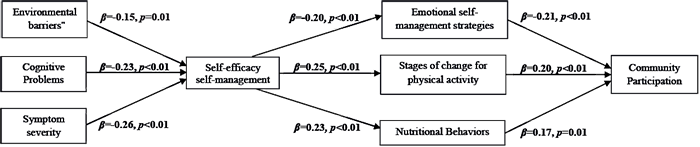
Fig. 2. Path model coefficients calculated via a series of multiple regression analyses (using imputed dataset).
Discussion
Although previous studies of MS have explored factors associated with participation (31–33), these studies have typically only evaluated bivariate correlations or used narrowly focused measures of participation, such as employment status or the Role Physical and Role Emotional subscales of the SF-36. This study advances MS research literature by exploring several factors that possibly directly and/or indirectly influence a participation measure that accounts for preferences to engage in activities that are meaningful to the individual. Our path analysis provides preliminary support that our data were consistent with the hypothesized model depicted in Fig. 1. We found that cognitive problems and environmental barriers had the largest negative direct effect on participation. We also found that self-management self-efficacy might have indirect effects on participation via engagement in self-management behaviors. Below we discuss the results of the path analysis and provide possible explanations on the relationships found between independent variables and participation.
Path analysis
Although models predicting health-related quality of life among people with MS have been published, to date, no path models predicting participation in meaningful activities across different life roles among people with MS have been published. Path analysis has advantages over traditional regression analysis because of the option to explore relationships between sets of independent variables and identify direct and indirect effects on the dependent variable (29). Path analysis is a more feasible alternative to structural equation modeling, which has recommendations to use sample sizes of more than 500 participants even for testing simple models with few parameters (29, 34). Our hypothesized model needed to have several parameters to help explore the complex dynamics that influence participation in meaningful activities. Thus, our analysis serves as a starting point for future longitudinal studies that examine additional variables in a larger sample size using structure equation modeling to create latent variables and calculate model fit statistics.
Self-efficacy
Our results are consistent with Lorig’s self-management framework (12). Lorig’s 6-week self-management program can significantly improve self-management self-efficacy and higher self-efficacy is a predictor of better health outcomes (35). However, there is a dearth of intervention studies in MS that have incorporated self-management self-efficacy and comprehensive participation measures. The potential utility and clinical relevance of targeting a single psychological factor that might improve participation across several different life roles merits further research. Future research should examine the different ways that self-management self-efficacy might play in mediating the relationships between impairments, activity limitations, and participation in life roles as well as explore the relative importance of different types of self-efficacy and more global psychological characteristics, such as locus of control and personality traits, in influencing participation in life roles.
Self-management behaviors
We found that increased readiness or higher stages of change for physical activity, increased engagement in healthy nutritional behaviors, and decreased use of emotional self-management strategies were associated significantly with greater participation. Physical activity and nutritional behaviors are activities involved in a variety of different life roles and might indicate better community integration and increased participation across different life roles. However, it was surprising that our results indicated that increased use of emotional self-management strategies were associated with lower self-management self-efficacy and decreased participation. Having to frequently use visualization or employ other distraction techniques may indicate a higher incidence of experiencing bothersome symptoms. This supposition is somewhat supported with the backwards selection model and finding that emotional self-management was not included in the final model when impairments were included.
Impairments and activity limitations
We found that increased limitations in activities due to cognitive impairment was associated significantly with lower levels of participation, whereas mobility problems and difficulties engaging in ADLs had a small and non-significant association with participation. Consistent with the research literature for people with MS, cognitive impairment can negatively impact many aspects of daily life and is a significant and consistent predictor of reductions in quality of life (36). However, the latter findings about mobility impairment and ADLs are inconsistent with the existing research literature in people with disabling conditions (32, 37). These inconsistent results may reflect differences in participation measures. Most participation questionnaires measure the frequency, limitation, or satisfaction with engaging in an activity or social role (7). Asking about satisfaction with a particular activity, as in the Participation Measure for Post-Acute Care (38), is different than asking whether the task is important and carried out often enough. It may be that dissatisfaction with an activity is more indicative of frustration with impairments, while whether a factor is important and being done enough is indicative of a multitude of factors. Jette et al. (37) reported that the association between activity limitations and participation restrictions varied across subscales. Clearly, there is a need to conduct research that compares different measures of participation and activity limitations.
Environmental factors
We found that increased environmental barriers were associated significantly with lower self-management self-efficacy and lower participation. Our findings are consistent with other studies that have found a moderate association between environmental factors and participation in life roles (17). Encouraging social support and teaching skills to utilize community resources might be strategies for reducing environmental barriers (12). Future research should explore whether the strength of the association between environmental barriers and participation is stronger when timing and types of activities correspond between measures. For example, the CHIEF-SF asks broad questions about an individual’s environment over the past year, while the CPI asks specific questions about particular behaviors over the past week or month. Asking about environmental barriers and facilitators in relation to each particular item in a participation measure may reveal a higher correlation between the 2 constructs.
Study limitations
We were only able to explain 19% of the variance in participation, which indicates a need to examine additional theoretical frameworks and variables. Ravesloot et al. suggests that a sense of comprehensibility, manageability, and meaningfulness might be important constructs in connecting behavior change theories with participation as defined by the ICF (39). Doble’s conceptualization of meaningful occupation suggests that a person’s subjective experiences while engaging in an activity are influenced by the extent to which he or she feels a sense of accomplishment, agency/control, companionship, affirmation, pleasure, renewal, and coherence (40). Including salient and situational psychosocial constructs beyond self-efficacy, such as those suggested by Ravesloot and Doble, might help explain additional variance in participation. Additional personal factors or indicators of socioeconomic status should also be explored. Perceived income adequacy, years of education, and perceived social status in the community might influence skills, confidence and ability to participate fully in life roles.
This study was also limited by its cross-sectional approach, sample self-selection, and the use of only self-report measures. Because this was a cross-sectional correlation study, the hypothesized directional relationships depicted in the path model cannot be confirmed. The generalizability of this study was limited to a white middle-class population with MS. Self-selection via online surveys may result in under-representation of persons from minority backgrounds and those with lower income or severe disability. Furthermore, there are unknown differences between recent responders of the NARCOMS survey and the general MS population. The use of self-report measures may have resulted in the misclassification of participants, a shortcoming that may have been amplified by our use of multiple imputation techniques that could have influenced correlation estimates in unknown ways. However, there were minimal differences when comparing missing data models to models that included all participants. Longitudinal designs that use structural equation modeling to include latent variables of objective and self-report measures of function, self-management behaviors, and additional psychosocial constructs would provide more compelling evidence for the hypothesized model in Fig. 1.
Ackowledgements
This work was supported through the National Multiple Sclerosis Society (NMSS) post-doctoral training grant and in part by the National Institute of Nursing Research of the National Institutes of Health (NIH) under award number K01NR012975 for supporting time in writing the manuscript and CTSA KL2TR000440 for supporting time in conducting the statistical analysis. The information presented in this article does not necessarily reflect the position, ideas, or opinions of the NMSS and NIH.
References

