Christoph Gutenbrunner, MD PhD1, Jerome Bickenbach, LLB, PhD2,3, Carlotte Kiekens, MD4, Thorsten Meyer, PhD5, Dimitrios Skempes, PT, MPH2,3, Boya Nugraha, MS, PhD1, Matthias Bethge, MS, PhD6 and Gerold Stucki, MD PhD2,3
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Germany, 2Swiss Paraplegic Research, Nottwil, 3Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, Switzerland, 4Physical and Rehabilitation Medicine, University Hospitals Leuven, Leuven, Belgium, 5Integrative Rehabilitation Research Unit, Institute for Epidemiology, Social Medicine and Health Systems Research, Hannover Medical School and 6Institute of Social Medicine and Epidemiology, University of Lübeck, Lübeck, Germany
OBJECTIVE: Rehabilitation is one of 4 main health strategies. The World Report on Disability identifies deficits in rehabilitation care for people with disabilities as an important barrier to full inclusion in society or to achieve optimal functioning. In order to overcome such deficits, to close gaps in national and/or regional rehabilitation systems, and to develop appropriate rehabilitation services, it is crucial to define uniform criteria and a widely accepted language to describe and classify rehabilitation services. The aim of this paper was therefore to develop a list of dimensions and categories to describe the organization of health-related rehabilitation services.
METHODS: The classification is based on a series of expert workshops including members of the International and European Society of Physical Medicine and Rehabilitation.
RESULTS: The proposed classification has 2 levels (dimensions and categories). The upper level distinguishes 3 dimensions: the service provider (with 9 categories), the funding of the service (with 3 categories), and the service delivery (8 subcategories). A further specification of the categories in a 3-level classification (including value sets) is needed.
CONCLUSION: This paper is an intermediate step towards development of a classification system with distinct categories and dimensions.
Key words: health-related rehabilitation; service organization; classification system; dimensions; categories.
J Rehabil Med 2015; 47: 809–815
Correspondence address: Christoph Gutenbrunner, Department of Rehabilitation Medicine, Coordination Centre for Rehabilitation Research, Hannover Medical School, Carl-Neuberg-Str. 1, DE-30625 Hannover, Germany. E-mail: gutenbrunner.christoph@mh-hannover.de
Accepted Jun 10, 2015; Epub ahead of print Sep 7, 2015
INTRODUCTION
Rehabilitation can be understood as one of 4 main health strategies (1–3). It aims at enabling persons experiencing disability to achieve optimal functioning (4). Thus, it is one of the most important tools for overcoming disability in persons with health conditions, such as congenital deformities, chronic diseases or trauma (5). In this context, disability may be defined as the result of an interaction between the person with a health condition and his or her environment (5, 6). Thus rehabilitation must aim both at empowering persons experiencing disability to enhance their level of activity and participation, and at removing barriers from the environment (4). Physical and Rehabilitation Medicine integrates medical interventions to improve body functions and activities and actions to overcome environmental barriers, e.g. providing assistive technology or advising employers to create a supportive work environment (7).
The World Report on Disability (WRD) (5) identifies deficits in rehabilitation care for people with disabilities as an important barrier to full inclusion into society. On the other hand, the report demonstrates that good rehabilitation services can help significantly to enable participation. Consequently the WRD states “the priority is to ensure access to appropriate, timely, affordable, and high-quality rehabilitation interventions, (…) for all those who need them” (5). For stakeholders the report claims that:
And, very concretely, the WRD states that “plans should be based on analysis of the current situation, consider the main aspects of rehabilitation provision – leadership, financing, information, service delivery, products and technologies, and the rehabilitation workforce” (5). This assumes that there are tools to analyse the provision of rehabilitation services and to identify gaps in relation to the needs of persons with disabilities. Other related points are the improvement in funding and the enhancement of the rehabilitation workforce (8).
In order to overcome deficits and to close gaps in national and/or regional rehabilitation systems, as well as to build up appropriate rehabilitation services, it is crucial to define uniform criteria and widely accepted language to describe and classify rehabilitation services. For international comparisons such a classification must be accepted internationally. It must be feasible and applicable in different world regions and cultures. Such a classification for rehabilitation service organization has not yet been developed.
There are, however, several classifications within the health system that have been published at national and international levels that make some reference to the description of health-related rehabilitation services. The most relevant are:
Certainly, classifications for diseases and the functioning of patients are of also major relevance, especially:
Many aspects of the classifications listed above are useful in many different ways, e.g. to describe rehabilitation services. However, due to the specific goals and methods of these classifications, there is a need to adapt their items and to combine them in a new system that covers all aspects of rehabilitation service organization.
Recently, Meyer et al. (12) published a conceptual description of health-related rehabilitation services, describing them as “personal and non-personal intangible products provided to persons with a health condition experiencing or likely to experience disability or to their informal care-givers within an organisational setting (…) addressing individual functioning needs (…) delivered by rehabilitation professionals, other health professionals, or appropriately trained community-based workers.” This description implies that rehabilitation services are, on the one hand, characterized by their goals, but, on the other hand, can be described by their organizational setting, including technical and human resources.
The aim of this paper is to develop a list of dimensions and categories to describe the organization of health-related rehabilitation services. The classification starts from the above-mentioned definition of a rehabilitation service, as given by Meyer et al. (12). It will take into account existing descriptions of health-related rehabilitation services at national and regional levels (13, 14) and criteria being used to compare specific types of health-related rehabilitation services (15, 16).
This paper is intended as an initial proposal for further discussion and consensus by experts from all International Society of Physical and Rehabilitation Medicine (ISPRM) areas and subareas (17).
Methods and classification principles
The dimensions and categories described here were developed in working groups of the “Strengthening Medical Rehabilitation Subcommittee” within the “WHO Liaison Committee” of ISPRM and Public Health Committee within ESPRM. These working groups have specific expertise in Physical and Rehabilitation Medicine, and Rehabilitation, and Public Health Research. The process was continued in a total of 6 2-day workshops with intermediate literature search and reflections in between the meetings.
In the first meeting the following principles were agreed:
In the literature, the term “rehabilitation service” is not used uniformly (12). Sometimes it is used for the offer of a set of interventions applied to a target group and seen as the treatment process. Other authors, e.g. Meyer et al. (12), have used it as an organizational term related to the setting or organization that provides rehabilitation measures. In this paper we use the term in the latter sense. This also refers to the conceptual description of rehabilitation as a health strategy (4). Furthermore, it is in line with the World Health Organization (WHO)’s definition of rehabilitation as “a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments”.
The dimensions and categories aim to describe rehabilitation services, as defined by Meyer et al. (12), at the meso level. However, some overlap with the macro level (health policy and health system) and the micro level (programmes, interventions, patients) may occur (Fig. 1).
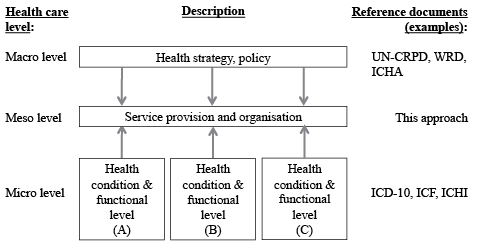
Fig. 1. Healthcare levels and reference documents. UN-CRPD: UN-Convention for the Rights of People with Disabilities; WRD: World Report on Disability; ICHA: International Classification of Health Accounts; ICD-10: International Classification of Diseases 2010; ICF: International Classification of Functioning, Disability and Health; ICHI: International Classification of Health Interventions.
The proposed classification is not a measurement tool in itself. The dimensions at the present stage are still at a conceptual level. Thus, another step is needed to define value sets and measurement tools, and their application.
Classification dimensions
At this point the classification consists of 2 levels:
A third level with value sets may be added at a later stage of development.
The dimensions consist of 3 main characteristics of service organization. Level 1 distinguishes between 3 dimensions:
1. Service provider: the categories to describe the provider include the framework of the institution (location, organization, etc.) the resources (human and technical resources) and some aspects of service organization, such as profit-orientation and quality-assurance programmes. These categories respond to questions concerning where, by whom, and in which context the service is delivered.
2. Funding of the service: the categories of funding describe the main sources of income and refunding of services. They include the basic principles of payment, such as diagnosis-related groups, per-day payment or other forms of service refund. The underlying question here is what are the principles of founding a service.
3. Service delivery: the categories for service delivery contain the main strategy applied to the users, aspects of intensity and duration of intervention and the way the service is organized (e.g. team structure). It focuses on the question what, for what, and how the services are delivered to the user.
These 3 dimensions are categorized in the level 2 classification. It contains the following categories, with some examples in parentheses:
1. Provider
1.1 Location (centralized vs. decentralized service, situated in rural area vs. urban area, accessibility (transport systems and others) and other dimensions of location).
1.2 Organization (independent organization, affiliation, or other dimensions of organization).
1.3 Context (single practise, community-based service, institutional care, such as nursing home or hospital-based service, home-based or other dimensions of context).
1.4 Facility (building, hotel service and other aspects of facility).
1.5 Human resources (health professionals, administrative staff, technical staff, and other personnel).
1.6 Technical resources and equipment (diagnostic devices, therapeutic devices and treatment modalities, data procession and communication, and other technical resources).
1.7 Quality assurance (total quality assurance system, single quality assurance measures and other methods of quality assurance).
1.8 Profit-orientation (profit-oriented, non-profit organization as charity organization and others, and other aspects of profit-orientation).
1.9 Other categories of provider.
2. Funding
2.1 Source of money (health insurances, pension insurances, accident insurance or other insurances, social welfare system, private payment, e.g. out-of-pocket payment, founds, or other sources of money).
2.2 Criteria of cost refund (Diagnosis related group-system, day-based payment, or other systems).
2.3 Other criteria of funding.
3. Service delivery
3.1 Strategy (prevention (preventive strategy), therapy (curative strategy), rehabilitation (rehabilitation strategy), maintenance (supportive strategy), or other health strategies).
3.2 Target groups (e.g. patients with defined health conditions, persons with specific deficits in body functions, activities and participation, case mix index and other target groups).
3.3 Service goals (restitutio ad integrum, improvement of health status, improvement of self-care, return to normal life, return-to-work, or other service goals).
3.4 Aspects of time (phase of disease (acute phase, post-acute phase, long-term phase), time-frame of intervention (short-term intervention, long-term intervention, intermittent interventions), number and duration of treatment time per day, and other aspects of time).
3.5 Intensity (high, medium or low intensity or other dimensions of intensity).
3.6 Team structure (involved professions, team organization (e.g. multidisciplinary team, interdisciplinary team), or other dimensions of team structure).
3.7 Mode of production (hospitalization, inpatient service, day clinic, outpatient service or other modes of production).
3.8 Other categories of service delivery.
If education and training are part of service provision (e.g. in university hospital), students and trainers could be classified as target groups (point 3.2) and education and training as service goals (point 3.3). Consequently, trainers should be included in human resources (point 1.5). The same principle applies to scientific programme and research (see Table I).
|
Table I. Application of the dimensions and categories of the 2-level classification to the selected rehabilitation services |
|||||
|
Number |
Dimension and category |
Rehabilitation service A |
Rehabilitation service B |
Rehabilitation service C |
Rehabilitation service D |
|
Type |
University department |
Inpatient and outpatient rehabilitation service |
Inpatient and outpatient rehabilitation service |
Community-based rehabilitation service |
|
|
Name, place |
Department for Rehabilitation Medicine, Hannover Medical School, Hannover, Germany |
Department for Rehabilitation Medicine, Fatmawati, Jakarta, Indonesia |
Saint Joseph’s Children and Adult Home, Mambu, Bafut, NWR, Cameroon |
Functional rehabilitation programme for achieving independence and autonomy in the community, Medellin, Colombia |
|
|
1. |
Provider |
||||
|
1.1. |
Location |
City |
City |
Village |
Poor neighbourhoods in a city |
|
1.2. |
Organization |
Public |
Public/government hospital |
Private |
Non-governmental |
|
1.3. |
Context |
University hospital |
General hospital |
Rehabilitation centre |
City neighbourhoods |
|
1.4. |
Facility |
Rehabilitation department |
Rehabilitation department for outpatient and inpatient ward, orthotic and prosthetic workshop and wheelchair workshop |
Rehabilitation department with vocational training, orthopaedic workshop, Infirmary, shoe-making works, embroidery workshop, cane workshop, bakery and the resource room for the visually impaired |
Community centres and homes |
|
1.5. |
Human resources |
Multiprofessional team: physicians, physiotherapists, occupational therapists, dysphagia therapists, sport therapist, researchers |
Multiprofessional team: PRM specialists, physiotherapists, occupational therapists, speech therapist, prosthetics and orthotics, social workers, nurse, psychologists |
Physical therapists, orthopaedic technicians, prosthetic technicians, special education teachers, technical workers |
Interdisciplinary team: physiotherapists, psychologists, social workers, special trainer, sign language interpreter, sign language teacher (hearing impaired) |
|
1.6. |
Technical resources |
Physical medicine devices, medical training, gymnasium, pool, laboratory diagnostics, functional assessment |
Physical medicine devices, training gymnasium, pool, workshop for prosthetics and orthotics and wheel chairs |
Gymnasium, mechanical electrical and gait devices. Workshop for the production of wheelchairs and tricycles, cane devices, beads and bangles, shoes. |
Not required |
|
1.7. |
Quality assurance |
Single quality assurance measures |
Single quality assurance measures |
No feedback with the patient. |
Single quality assurance measures and feedback with the community |
|
1.8. |
Profit-orientation |
Non-profit |
Non-profit |
Non-profit |
Non-profit |
|
1.9. |
Other categories |
Teaching hospital |
Affiliation teaching hospital for PRM residence (education to become PRM specialist), practical ground for physiotherapists, occupational therapists, psychologist |
Rehabilitation services and practical ground for physiotherapists, occupational therapists and special education teachers for internship |
Education and training services for people with disabilities |
|
2. |
Funding |
||||
|
2.1. |
Source of money |
Public, health insurance |
Public, mostly government insurance |
Patients, well-wishers and non-governmental organizations |
Special public resources of the Medellin township called “participatory budgeting” whose destination is defined by the boards of the involved communities |
|
2.2. |
Criteria of cost refund |
Budget, internal settlement with other department, health insurance |
Budget and government health insurance |
No refund from the government |
Budget |
|
Table I. Condt. |
|||||
|
2.3. |
Other categories |
Research grants |
Donations |
Donations |
Social fund resources (institutional fund for payment of services not included in the programme) |
|
3. |
Service delivery |
||||
|
3.1. |
Strategy |
Rehabilitation, therapy, maintenance |
Rehabilitation, maintenance and prevention |
Rehabilitation and vocational training |
Group work for instruction in achieving independence and autonomy in activities of daily living, teaching sign language and Braille, field work with disabled people in different areas of the city |
|
3.2. |
Target groups |
Patients with a wide range of acute and chronic health conditions (predominantly musculoskeletal, neurological incontinence and postoperative) as well as all inpatients of the university hospital |
Patients with a wide range of acute and chronic conditions (musculoskeletal, neurological, spinal cord injury, bladder dysfunction, pediatric, geriatric), preventive rehabilitation (club of exercise activity for diabetic, heart and lung, stroke, osteoporosis and geriatric patients) |
Patients referred from higher levels of complexity to lower levels. Patients who do not have access to more comprehensive rehabilitation services |
Patients referred from higher levels of complexity to lower levels. Patients who do not have access to more comprehensive rehabilitation services |
|
3.3. |
Service goals |
Improvement in health condition and functioning of inpatients, rehabilitation of outpatients; research, training |
Preventing disability and improvement functioning of inpatient and rehabilitation of outpatient to achieve independency and quality of life |
Prevent, improve and restore function with mobility training in order to restore dignity, and improve living standards of those with physical and visual impairment in our society. |
Improved levels of independence and autonomy in activities of daily living and participation in different areas of the city |
|
3.4. |
Aspects of time |
Acute; post-acute; long-term. Inpatients: length of stay in acute ward (days to weeks); Outpatients: 2 weeks to 6 months |
Inpatients: weeks to months for spinal cord injury patients; and days to weeks for patients who need intensive rehabilitation (e.g. stroke patients) Outpatients: 2 weeks to 6 months |
Post-acute; long-term; and long life time for specific cases (e.g. cerebral palsy, post-polio, and spinal cord injury) |
Each programme has a duration of 6 months |
|
3.5. |
Intensity |
Inpatients: high intensity; outpatients: low intensity |
Inpatients: high intensity; outpatients: low intensity |
Inpatients: high intensity; outpatients: low intensity |
Low-intensity intervention by health professionals. Plans are provided for training at home |
|
3.6. |
Team structure |
Multiprofessional |
Multiprofessional |
Multiprofessional |
Multiprofessional |
|
3.7. |
Mode of production |
Inpatient and outpatient |
Inpatient and outpatient |
Inpatient and outpatient |
Only outpatient services in the community |
|
3.8. |
Other categories |
Scientific research |
Collaboration with prosthetics and orthotics school |
Collaborative benefits with other institutions |
Training programmes for people with disabilities and community leaders |
|
PRM: Physical and Rehabilitation Medicine. |
|||||
As mentioned above, a further specification of the categories in a 3-level classification is needed. Such value sets should be suitable for describing the categories; however, they are not intended to provide parameters or value sets to measure the categories.
DISCUSSION
This paper offers a proposal for the dimensions and categories required to describe and compare service organization in health-related rehabilitation services at the regional, national and international level. The classification includes 3 dimensions, comprising a total of 20 categories. These categories should be described by values sets that have not been defined previously. Such value sets could further specify the categories in the following way:
The proposed classification on 2 levels is comprehensive and has the potential to be used as a basis for the development of a distinct classification system.
According to the WHO (18) key components of a health system are governance and information, in addition to financing, human resources, products, technologies, and service delivery. These components have some overlap with the proposed classification; however, they also show some overlap between the macro and meso levels of healthcare (see 12).
As with other classification systems, there are some implicit problems with our proposal: first, the dimensions have been developed in only a small group of experts. Secondly, overlap or interaction of dimensions could not been totally excluded. Thus, the categories may not be strictly mutual exclusive, although the degree of overlap or interaction was judged acceptable by the working group. The leading principle was the applicability of the concept. Thirdly, the development of the classification in a group of European experts may limit its application in other world regions and different cultural and society contexts. This has been, at least partly, compensated, as experts from South America, Sub-Saharan Africa, South East Asia and Europe tested its feasibility by applying it to characterize existing rehabilitation services (see below).
Papers on the taxonomy or classification of specialized rehabilitation services have been published previously. For example, Hoenig et al. (19) published a taxonomy of relevant variables derived from a Delphi process among rehabilitation experts. They identified the following main categories:
Interestingly, financing is not part of their list of characteristics, probably due to the fact that the survey was carried out in a region with a uniform payment structure. However, economic pressure underlines the need for a transparent description of financial sources and costs required to meet patients’ needs and to achieve the intended outcomes (13).
From a regional perspective Graham et al. (14) identified a set of parameters to describe rehabilitation services using a mixed methods approach. They aimed at an international comparison between standards in Australia and New Zealand with those in the UK and USA. They identified the following issues that were best covered in the investigated standards:
Comparing these items with our proposal, number 1 is partly included in the dimension of the provider, number 2 coincides with our number 1.6 (technical equipment), number 3 is similar to our number 1.5 (human resources) and covers aspects of number 3.6 (team structure). Number 4 is related to some aspects of our third dimension (service delivery). Numbers 5 and 6 are related to interventions that are not part of the service classification but fit into the ICHI classification (9).
The list of dimensions and categories of rehabilitation services is comprehensive and covers a wide variety of aspects. However, it contains aspects from the micro-level of service delivery, such as rehabilitation programmes and diagnoses. Thus, it cannot be directly compared with our approach, although it can be used to redefine our categories.
Referring to the cited references, Table I shows an example of the dimensions and categories for 4 existing rehabilitation services without going to the level of value sets. Even this level of specification can provide a distinct picture of the services described and identifies differences in service organization. Table I also shows that, at this level of specification, the choice of criteria used to describe the rehabilitation service is variable. Thus, for scientific studies and for practical use, the development of value sets will be necessary.
Another example of the use of dimensions and components of rehabilitation services for the comparison of rehabilitation services is the assessment of human resources of the rehabilitation workforce (14). It shows that this parameter is feasible for international comparisons; however, it also shows that there may be gaps in the provision of value-sets (e.g. the ISCO code is lacking a clear definition of rehabilitation physicians). Another example is the comparison of rehabilitation services with the purpose of comparing health outcomes. Hoenig and colleagues used their taxonomy for stroke rehabilitation services, as described above, and showed that their classification system can be used to identify service factors associated with rehabilitation outcomes (15). In more detail, they identified specific organizational factors that were independently associated with differences in stroke patient outcomes, after controlling for patient characteristics, e.g. a greater availability of nursing personnel was associated with a slightly shorter length of stay.
The next step towards a broader consensus of this draft classification is a worldwide discussion with other experts in rehabilitation and health classifications; comments to the authors are therefore welcomed. After taking these comments into consideration, the working group will produce a revised version that then will be discussed and approved within the ISPRM. In parallel, some preliminary testing should be done, such as:
In addition, value sets should be defined and measurement systems or scales developed. A project should be performed to link the dimensions of this classification to other classifications and definitions in matrices (e.g. health strategies and PRM services). Finally it is hoped that the classification will be used to compare rehabilitation services worldwide and to identify gaps in rehabilitation systems, as called for by the World Report on Disability (5).
ACKNOWLEDGEMENTS
The authors would like to thank Dr Ngaibe Victorine from Saint Joseph’s Children and Adult Home, Mambu, Bafut, NWR, Cameroon; Peni Kusumastuti, MD, SpRM, from the Department for Rehabilitation Medicine, Fatmawati, Jakarta, Indonesia; and Professor Luz Helena Lugo, MD, from Grupo de Rehabilitacion en Salud, Universidad de Antioquia, who provided information for Table I.
The author declare no conflicts of interest.
REFERENCES

