
From the 1Department of Rehabilitation Medicine, 2Department of Medicine, the University of Melbourne, 3Melbourne EpiCentre and 4Department of Respiratory and Sleep Medicine, Royal Melbourne Hospital, Melbourne, Australia
Objective: To investigate whether the use of cognitive behavioural therapy in pulmonary rehabilitation addresses the depression and anxiety burden and thereby improves rehabilitation outcomes.
Design: Prospective controlled clinical trial.
Patients: A total of 70 patients with chronic obstructive pulmonary disease who were referred to a community centre for pulmonary rehabilitation.
Methods: Patients were allocated to either the control group, consisting of pulmonary rehabilitation alone, or to the treatment group, receiving pulmonary rehabilitation and an additional 6 sessions of group-based cognitive behavioural therapy. Assessments consisting of questionnaires and walk tests were conducted pre- and post-pulmonary rehabilitation.
Results: A total of 28 patients were enrolled. The cognitive behavioural therapy group had significant improvements in exercise capacity following pulmonary rehabilitation (mean change 32.9 m, p = 0.043), which was maintained at 3 months post-pulmonary rehabilitation (mean change 23.4 m, p = 0.045). Patients in the cognitive behavioural therapy group showed significant short-term improvements in fatigue, stress and depression (mean change 2.4, p = 0.016, 3.9, p = 0.024 and 4.3, p = 0.047, respectively) and a 3-month post-pulmonary rehabilitation improvement in anxiety score (mean change 3.1, p = 0.01). No
significant changes were seen in the control group.
Conclusion: The addition of cognitive behavioural
therapy improved patients’ physical, psychological and quality of life results. Cognitive behavioural
therapy should be considered for inclusion in a
pulmonary rehabilitation programme to enhance outcomes.
Key words: pulmonary disease, chronic obstructive; pulmonary rehabilitation; cognitive therapy; psychotherapy.
Accepted Nov 4, 2016: Epub ahead of print Feb 2, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Edwin K. Luk, Department of Rehabilitation, Royal Melbourne Hospital, 3052 Melbourne, Australia. E-mail: Edwin.luk@mh.org.au
Chronic obstructive pulmonary disease (COPD) is a major cause of mortality, morbidity and health service use worldwide. COPD affects both the ability of patients to perform their activities of daily living and their quality of life. It is projected that COPD will be the seventh leading cause of loss of disability adjusted life years (DALYs) worldwide by 2030 (1).
COPD affects not only the lungs, but is a systemic disease causing other body system pathology, such as skeletal muscle dysfunction (2). Patients with COPD often experience limitations in physical and functional activity, but it is difficult to determine whether these changes relate to the disease itself or to reduced activity levels as a consequence of progressive lung disease (3).
Pulmonary rehabilitation (PR) involves patient assessment, exercise training, education, behaviour change, nutritional intervention and psychosocial support (4). Benefits of PR include improved exercise tolerance, improved quality of life and lowered perception of dyspnoea (5). Exercise programmes alone have clear benefits, while the benefits of education or psychosocial support without exercise training are less well documented (6). Comprehensive programmes incorporating all 3 interventions (exercise, education and psychosocial support) have the greatest benefits.
Comorbid psychological disorders are a significant burden for patients with COPD, in whom there is an increased prevalence of depression (36%) and anxiety (40%) (7). Patients with psychological co-morbidities are more likely to have reduced engagement and participation and subsequently reduced quality of life (6). The presence of anxiety or depression worsens the degree of dyspnoea and, consequently, patients are more likely to be sedentary at home (8).
Despite this, the treatment and rehabilitation of these patients focuses only on the physical characteristics of the disease. A systematic review of various psychological interventions showed some improvements in psychological outcomes when these were analysed together. However, when CBT was analysed as an intervention alone, there were significant improvements in psychological, but not physical, outcomes (9). Ultimately, the optimal type or intensity of psychological interventions remains unknown (9).
The objectives of this study were to: (i) conduct a clinical controlled trial (CCT) comparing the current PR regime with a programme adding cognitive behavioural therapy (CBT) to the existing schedule; and (ii) confirm that a directed psychological intervention consisting of CBT improves patient participation and clinical outcomes in PR.
This was a prospective CCT conducted at Royal Melbourne Hospital (RMH) and Merri Community Health Service (MCHS). Approximately 100 patients with stable COPD undertake outpatient PR each year at MCHS. Patients who were diagnosed with COPD and treated by the RMH respiratory service were referred to MCHS for ongoing pulmonary management and rehabilitation. The diagnosis and severity grading of COPD was based on the Global Initiative for COPD (GOLD) criteria, as assessed by the respiratory and rehabilitation physicians at RMH (10). This study was approved by the Human Research Ethics Committee at Melbourne Health (HREC Approval 2012.174).
All patients who were referred to the ambulatory PR programme during the 18-month trial were screened and consented for participation into the study. The multidisciplinary team, consisting of respiratory and rehabilitation specialists, physiotherapists and nurses, screened each patient according to the criteria. Patients were eligible for this study if they had stable COPD, ability to comprehend English and the consent to the study, and were able to attend regular PR sessions. Stable COPD was defined as no exacerbations within the previous 6 weeks and on optimal pharmacological therapy. Exclusion criteria included previous psychological treatment within the past 3 months and any significant psychiatric history, such as psychosis, bipolar disorder, schizophrenia, mental retardation, borderline personality disorder, chronic suicidal behaviour or major depressive disorder with previous episodes of hospitalization. The patient’s general practitioner was contacted if the psychiatric diagnosis was unclear.
Patients were allocated to either the treatment group, consisting of additional group based CBT and the usual PR, or the control group, consisting of PR alone. Allocation was not randomized. Once patients were referred and assessed to be eligible for PR, they were enrolled into the next PR group. Due to resources, the CBT programme was delivered to consecutive patients in 2 PR cohorts during the 18-month period. Patients who were recruited outside of these times did not receive CBT and were allocated to the control group.
Patients in both groups received the usual PR programme. This 8-week programme consisted of multidisciplinary management including medical, nursing and allied health using standardized therapy protocols. Each week included 2 sessions of 2-h duration, consisting of group physical therapy and general education sessions. The 45-min exercise session consisted of 15 min treadmill/walking, 15 min cycling and 15 min circuit exercises. Patients were educated and monitored to ensure they spent most of their time on the treadmill or bike at a high level of intensity as per current American Thoracic Society guidelines (4). Group education was provided on issues such as how the lungs work, nutrition, advanced care planning and medication management. Whilst patients were educated on the link between dyspnoea and COPD, no specific information was provided in relation to recognizing triggers of dyspnoea or the use specific breathing strategies. An a priori compliance with outpatient treatment was participant attendance in > 80% of treatment sessions.
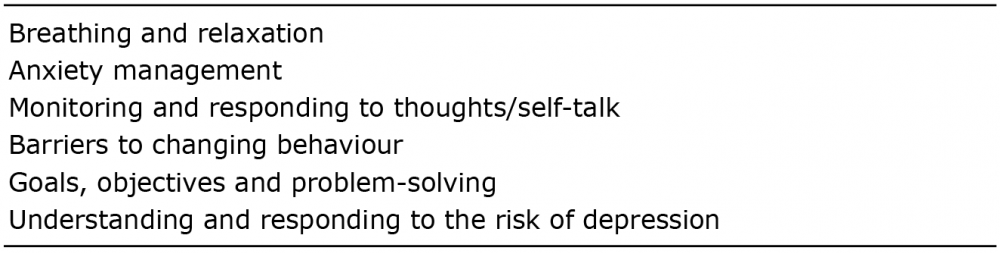
The CBT programme in the treatment group consisted of an additional 6 sessions of group-based CBT delivered by a psychologist. The psychologist did not take part in patient assessment. The content was designed in conjunction with the treating team to complement the pre-existing exercise and education programmes. The programme was not specifically directed at anxiety and depression, but incorporated common issues facing a PR participant. Table I lists the themes in the CBT group.
Patients progress was assessed in weekly meetings. Exercise schedules altered dependent on patient’s dyspnoea symptoms and vital signs during exercise. Adverse effects of rehabilitation were noted (e.g. falls, injury during treatment).
Table I. Themes in the cognitive behavioural therapy programme
All baseline participant interviews and clinical assessments were completed using a structured format. Demographic, functional, and quality of life (QOL) assessments were completed using standardized instruments. Assessors did not prompt patients, but provided assistance for those who had difficulty completing the questionnaires. COPD-related measures, such as socio-demographic, clinical and treatment data, were obtained from the medical record.
The primary outcome measure in this study was the Depression Anxiety Stress Scale (DASS) (short form). This is a 21-item self-reported questionnaire that measures the 3 related negative emotional states of depression, anxiety and tension/stress (11). Participants rated the extent to which they experienced each state over the past week on a 4-point Likert rating scale. When totalled, 3 domain scores are given. Scores greater than 9, 7 and 14 are suggestive of depression, anxiety and stress, respectively (11).
Secondary outcome measures included:
Data were keyed into Microsoft Excel (Microsoft, WA, USA) and exported into Stata12 (StataCorp, TX, USA) for data analysis and reporting. Descriptive analysis of study cohort was undertaken and results reported as n (%) for categorical data (e.g. sex) and median (interquartile range; IQR) for continuous data (Forced Expiratory Volume in one second (FEV1), forced vital capacity (FVC), body mass index (BMI), etc.).
The change in outcomes of interest between pre- and post-PR was calculated based on the score at end of PR minus the score at baseline. The 3-month post-PR change was calculated based on the score at the 3-month post-PR visit minus either the score at baseline or end of rehabilitation. Cohen’s d test was used to measure effect size. The differences were assessed for normality using Shapiro-Wilks test. Scores that were normally distributed, a 1-sample t-test was utilized to determine the significance of the change and its magnitude. Level of significance for the study was set at p < 0.05.
A total of 70 patients were screened for the study, 34 patients were consented (Fig. 1). Twenty-eight patients completed PR and completed all their assessments.
Fig. 1. Recruitment process. CBT: cognitive behavioural therapy; PR: pulmonary rehabilitation.
There were 14 patients in the CBT (treatment) group and 14 in the control group. Of the 6 non-completers, 5 were male; otherwise there were no statistical differences between the completers and non-completers.
Table II shows the baseline characteristics between the 2 groups. The mean age of study participants was 72.4 years (standard deviation (SD) 7.4), with 100% being smokers (past or present), mean FEV1 was 57.4% (SD 23.4) and 21% were on long-term oxygen therapy.
Table II. Baseline characteristics
Forty-three percent of participants lived alone and 7% of participants had only a primary education. There were no statistical differences between the 2 groups.
Table III describes participant’s outcome measures at baseline. There were no statistical differences between the 2 groups. DASS scores showed approximately half of the participants had probable depression and anxiety in both groups. These rates are higher when compared with the HADS scores or self-reporting.
Table III. Outcome measures at baseline
In the CBT group, statistical reductions were seen in depression and stress scores of the DASS (p < 0.05, p ≤ 0.02, respectively; Table IV). These improvements were not sustained at 3 months post-PR. In the anxiety sub-scale, a reduction was seen immediately post-PR, but was not statically significant. By 3 months post PR, a larger reduction was seen and was statistically significant (p < 0.01).
Table IV. Changes following pulmonary rehabilitation
In contrast, no significant improvements were seen in all 3 sub-scales in the control group.
Statistically significant improvements in the 6MWT were seen in the CBT group (p < 0.05). This was maintained at the 3-month post PR (p < 0.05). Improvements were also seen in the control group, but were not statistically significant.
In relation to the CRQ, only the fatigue domain had a statistically significant improvement in the CBT group (p ≤ 0.02). There was also a statistically significant improvement between the 2 groups (p = 0.03). Emotion and dyspnoea improved in both groups, though bigger changes were noted in the treatment group. However, these changes were not significant.
Both anxiety and depression scales in the HADS had reductions following PR in the CBT group, but were not statistically significant. In the control group, reductions were seen only in the depression scale. Again, none of the changes in the control group were statistically significant.
Reductions were seen in PAIS across both groups after completion of PR. None of the changes were statistically significant.
This is one of the few studies to examine strategies beyond physical measures for COPD. The results show that the addition of CBT to PR provides additional benefits. Greater improvements in the CBT group were seen in the 6MWT, HADS, DASS and CRQ (except Mastery). Only the 6MWT, fatigue, depression (DASS component) and stress measures were statistically significant (p < 0.05, p ≤ 0.02, p < 0.05, p ≤ 0.02, respectively).
The improvements in the 6MWT following PR were sustained at the 3-month post-PR time-point. At the 3-month post-PR, the improvement in the anxiety component of the DASS was statistically significant (p ≤ 0.02).
There was significant psychological comorbidity in patients in this study. Approximately half of study patients had depression or anxiety and 14% had stress on the DASS. This may have contributed to the lack of response to PR. This psychological burden was even higher than a previously conducted study in the same centre, which showed statistically significant improvements in the walk test and all 4 domains of the CRQ (18).
Two similar outcome measures (DASS and HADS) were used to measure anxiety and depression. Studies in the traumatic brain injury population reported both measures were valid as screening tools for anxiety and depression (19). In this study, the DASS showed higher prevalence rates than HADS. However, the DASS was more sensitive to changes following PR in the CBT group.
Despite the increasing recognition of psychological burden in patients with COPD, current Australian Lung Foundation Pulmonary Rehabilitation Guidelines do not recommend any routine screening or the use of psychological interventions (20). It is hoped that this study, along with other future studies, will offer additional evidence and suggest further modifications to the PR programme.
The use of CBT has been used more commonly for psychological disorders than in the general medical population. Reductions in stress and depression scores following CBT would be expected; however, this study showed CBT carries additional benefits to other impairments, such as exercise capacity. The CBT programme in this study was designed to address not only pre-morbid psychological burden, but also to enhance concurrent physical exercise and education programmes. Given that PR does not change lung function, the ultimate aim of PR would be not only to improve exercise capacity and QOL, but also improve self-efficacy and management of their disease (21).
Whilst there are trials evaluating the use of CBT in people with COPD, very few compare the additional benefits of CBT in PR. In a similar study, De Degoy et al. compared various PR components, such as exercise, education and CBT (22). This showed combined psychotherapy and exercise as well as psychotherapy alone were effective in improving exercise capacity, anxiety, depression and QOL. No statistical analyses were performed to show which group was more effective. Similarly, in this study it was shown that adding a CBT component provided additive benefits to a PR programme. Exercise alone in De Degoy et al. or PR alone in this study did not improve exercise capacity or QOL. In contrast, a systematic review on the role of physical exercise in COPD showed significant improvements in exercise and QOL (23). The improvements in the 6MWT and 6 of the 7 QOL domains exceeded the MID (23).
The PAIS was used as an outcome measure in this study to determine whether patients’ psychological adjustment changed following PR. With the greater recognition and treatment of psychological disturbance in COPD, it is hoped that patients would have increased psychological adjustment and associated self-coping. Whilst the PAIS scores reduced (indicating improved adjustment), the changes were not statically significant.
Respiratory studies frequently report on MID. MID attempts to define the smallest difference in score that patients would perceive as important (14). This is usually greater than statistical significance. In this study, the increases in 6MWT and the fatigue subscale of the CRQ, exceeded the MID (13, 14).
This study was a CCT, which could create bias. Participants were enrolled to either the CBT or control group based on when they started PR. A randomized controlled trial would provide a higher level of evidence though may be difficult to conduct with the small group sizes. Also, larger sample sizes would be ideal to provide statistically significant data.
PR, in particular exercise training has been shown to produce unequivocal improvements to QOL and exercise capacity (23). This study, in contrast has shown the PR programme at this centre does not produce similar results. An analysis involving a larger group of patients (n = 88) at this centre has shown statistically significant improvements in the walk test and CRQ (18). A larger sample size in this study may have been able to replicate these results. It would also allow further sub-analysis to determine whether certain factors, such as the presence of anxiety or depression, affects PR performance.
Another key difference is despite a similarity with severity of COPD compared with other studies, the mean CRQ scores were higher. Another study looking at PR in the same city and a similar cohort showed lower pre-PR CRQ scores (24).This means our patients at study entry had a higher QOL and thus further improvements in COPD-related QOL may have been limited. Further sub-analyses would be required to confirm this. Other factors that could have impacted on outcomes were beyond the scope of this study.
Data from participants were recorded up to 3 months after completion of PR. Information beyond 3 months were not recorded due to lack of funding. Further monitoring of participants would track the longevity and duration of gains with CBT. Patients who complete PR would typically return to their premorbid state (18). Furthermore, other factors which may be affected by PR, including the number or exacerbations or hospitalizations, were not recorded.
In conclusion, this study shows that the addition of a non-exercise intervention improves the efficacy of a PR programme. Non-physical exercise interventions should be considered in all PR programmes. Further research is required to determine which interventions are most effective.
The authors are grateful to all participants in this study. The authors thank the team at Melbourne Easy Breathers and Dr S. Kofoed for patient assessments and Dr L. Ng for assistance with ethics submission.


 Click to show fullsize
Click to show fullsize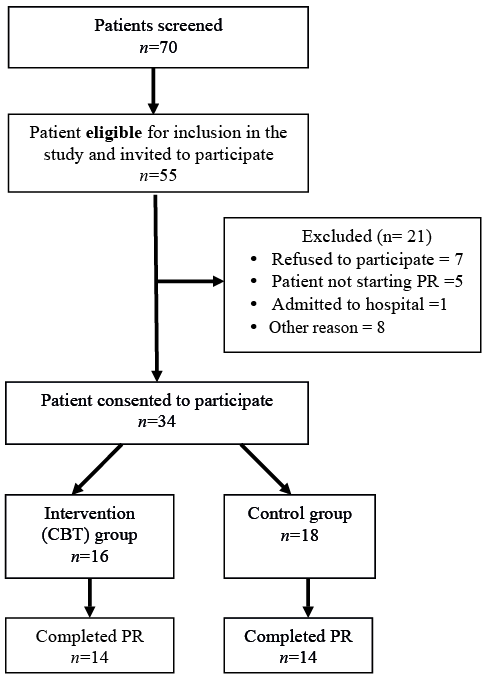 Click to show fullsize
Click to show fullsize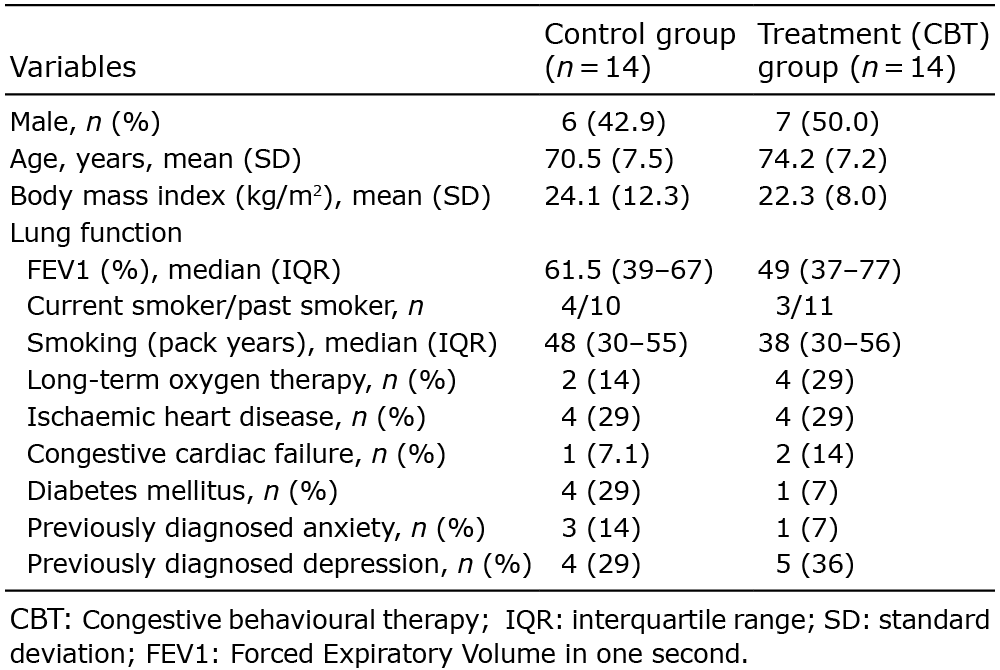 Click to show fullsize
Click to show fullsize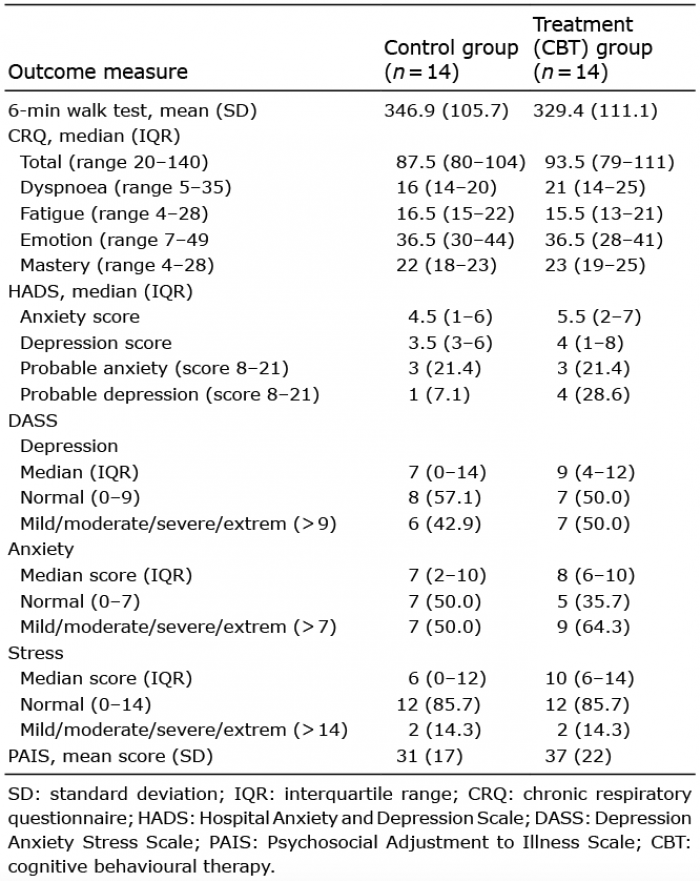 Click to show fullsize
Click to show fullsize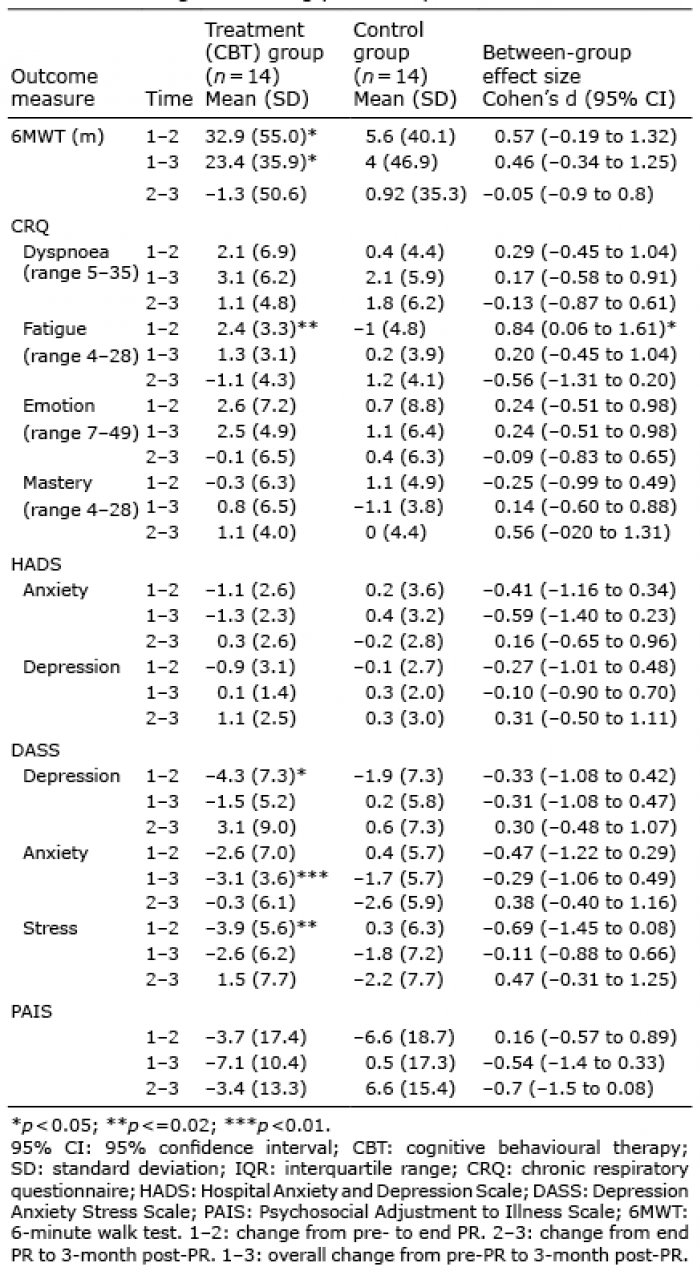 Click to show fullsize
Click to show fullsize