
From the 1Department of Physical Medicine and Rehabilitation, Shuang Ho Hospital, Taipei Medical University, New Taipei City, 2Department of Physical Medicine and Rehabilitation, Wan Fang Hospital, 3Graduate Institute of Injury Prevention and Control, College of Public Health, 4Department of Physical Medicine and Rehabilitation, School of Medicine, College of Medicine, 5Department of Physical Medicine and Rehabilitation, 6School of Gerontology Health Management, College of Nursing, Taipei Medical University, Taipei and 7Graduate Institute of Sports Science, National Taiwan Sport University, Taoyuan, Taiwan. #,*These pairs of authors contributed equally to this study.
Objective: To investigate the effects of Kinesio taping for stroke patients with hemiplegic shoulder pain.
Design: Double-blind, placebo-controlled clinical trial.
Subjects: Twenty-one stroke patients with hemiplegic shoulder pain within 6 months of stroke onset in the rehabilitation ward of a medical university hospital in Taiwan.
Methods: A 3-week intervention involving a conventional rehabilitation protocol and therapeutic Kinesio taping was conducted with an experimental group of 11 stroke patients. A control group of 10 stroke patients underwent an identical conventional rehabilitation programme and sham Kinesio taping on the hemiplegic shoulder. Numerical rating scale scores, Shoulder Pain and Disability Index, ultrasound findings and pain-free passive range of motion of the affected shoulder, were evaluated before and after the intervention. Mann–Whitney test was used to compare within-group continuous variables before and after the intervention. Wilcoxon signed-rank test was used to analyse the differences and changes in values between study and control groups.
Results: There was no statistical difference in demographic variables between the 2 groups. Both groups showed improvement in passive range of motion of the shoulder, (mean numerical rating scale 2.36 (standard deviation (SD) 1.03)), and mean Shoulder Pain and Disability Index (16.64 (SD 2.62)) after the intervention (p < 0.001); however, no significant between-group differences were observed in the numerical rating scale score, pain-free passive ROM, and ultrasound findings for the shoulder after 3 weeks of treatment. Concerning the variables changes, the therapeutic Kinesio taping group showed more improvement in the numerical rating scale (p = 0.008), shoulder flexion (p = 0.008), external rotation (p = 0.006), internal rotation (p = 0.040), and Shoulder Pain and Disability Index (p < 0.001) than the sham Kinesio taping group.
Conclusion: Stroke patients with hemiplegic shoulder pain can experience greater reductions in Shoulder Pain and Disability Index, pain, and improvement in shoulder flexion, external, and internal rotation after 3 weeks of Kinesio taping intervention compared with sham Kinesio taping. Kinesio taping may be an alternative treatment option for stroke patients with hemiplegic shoulder pain.
Key words: Kinesio taping; hemiplegic shoulder pain; stroke; ultrasound imaging; subluxation.
Accepted Dec 6, 2016; Epub ahead of print Feb 24, 2017
J Rehabil Med 2017; 49: 208–215
Correspondence address: Shih-Wei Huang, Department of Physical Medicine and Rehabilitation, Shuang Ho Hospital, Taipei Medical University, 291 Jhongjheng Rd, Jhonghe, New Taipei City 235, Taiwan. E-mail address: 13001@s.tmu.edu.tw
Stroke is the most common cause of disability among elderly people, often resulting in dependence in activities of daily living (1). Rehabilitation after stroke is crucial, especially during the golden period of functional recovery (2, 3). However, post-stroke hemiplegic shoulder pain (HSP) is a common complication that often hampers rehabilitation (4). Incidence of HSP is approximately 65–70% in acute and chronic stroke patients. The incidence of HSP in the past decade was approximately 17–37% in people with acute stroke, increasing to 47% in people with chronic stroke (5–9). HSP negatively affects daily activities and quality of life, and can increase duration of hospitalization (10, 11). This is often because shoulder pain occurring after a stroke is caused by weakness in the rotator cuff muscles, or because the effects of gravity can cause subluxation or tendon inflammation, resulting in the need for shoulder rehabilitation. Possible causes of HSP are subluxation (12), rotator cuff tears, rotator cuff and deltoid tendinopathy (13, 14), and bicipital and supraspinatus tendon tenderness (7). It is critical to prevent shoulder pain during post-stroke rehabilitation; however, there is limited evidence regarding the direct relationship between subluxation and HSP. Shoulder subluxation has been associated with rotator cuff tears, and thus it may be an indirect cause of HSP (15). No single type of shoulder pathology can account for all shoulder pain after stroke, and more than one type of shoulder pathology can cause pain within an individual. The pathogenesis of post-stroke shoulder pain has not been studied rigorously and remains controversial. Because several possible aetiologies of HSP exist, numerous treatment methods have been suggested, including electrical stimulation, acupuncture, strapping, sling, handling, positioning and massage and pharmacological therapy. However, none of these treatments has been shown to be significantly superior to others (16–18). Evidence supporting specific interventions for the management of HSP is limited. Several interventions have been developed for treatment, but evidence for these interventions remains insufficient (16).
Kinesio taping (KT) was developed by Kenzo Kase in the 1970s and has gradually become widely used as a clinical intervention in the treatment of musculoskeletal disorders (19). The product is a thin, elastic cotton tape applied to the skin, which can stretch to up to 140% of its original length. The tape can reduce mechanical retention and restriction of movement. The effects of KT include facilitation of muscle activation and increased blood and lymph circulation (20). Prescribed wear time for 1 application is usually 3–4 days. Several studies have focused on balance and posture control in post-stroke patients (21–23).
According to Jaraczewska & Long (24), KT could facilitate or inhibit muscle function, support joint structure, reduce pain, and provide proprioceptive feedback to achieve and maintain preferred body alignment. Some studies suggest that KT could decrease pain, improving range of motion (ROM) and motor performance in stroke patients (25, 26). Since there are few studies of the effect of KT in treating HSP, the aim of the current study was to undertake further assessment in this area. In addition, no imaging studies have assessed the effectiveness of KT on post-stroke shoulder protection. Therefore, this study used musculoskeletal ultrasound to assess shoulder conditions in addition to functional assessment scales. No imaging studies have assessed the effectiveness of KT on protection of rotator cuff injuries and tendonitis during rehabilitation among stroke patients. Therefore, in addition to a functional assessment scale, we used musculoskeletal ultrasound to evaluate the rotator cuff status of patients with HSP.
The aim of this double-blind, randomized, placebo-controlled study was to investigate the effects of KT on HSP among stroke patients. Specifically, we investigated the effects of KT on patient-centred measures, such as pain with motion, pain with passive ROM performed by a therapist, pain and disability (Shoulder Pain and Disability Index (SPADI)), and investigated changes in the subacromial space and rotator cuff pathology using diagnostic ultrasound to explain the findings from a pathological standpoint.
This double-blind, placebo-controlled clinical study was performed in the rehabilitation ward of a medical university hospital in Taiwan between January 2013 and December 2014.
Thirty eligible participants were initially recruited for this study. All participants met the following inclusion criteria: (i) unilateral ischaemic or haemorrhagic stroke lesion confirmed by computerized tomography or magnetic resonance imaging; (ii) first incidence of stroke, with onset less than 6 months prior to discharge; (iii) pain in the affected shoulder; (iv) adequate communication ability and intact cognitive function (Mini-Mental Status Examination scores ≥ 24 points). Exclusion criteria were: (i) shoulder pain or a history of surgery in the affected shoulder before the onset of stroke; (ii) skin problems, wounds, or infection on the affected shoulder; (iii) experience of using KT; (iv) a history of allergy to KT. After inclusion and exclusion processing, a total of 21 patients were enrolled in the study.
Participants provided informed consent following explanation of the study aim and procedures. The study protocols were approved by Taipei Medical University’s Institutional Review Board (TMU-JIRB-201308045).
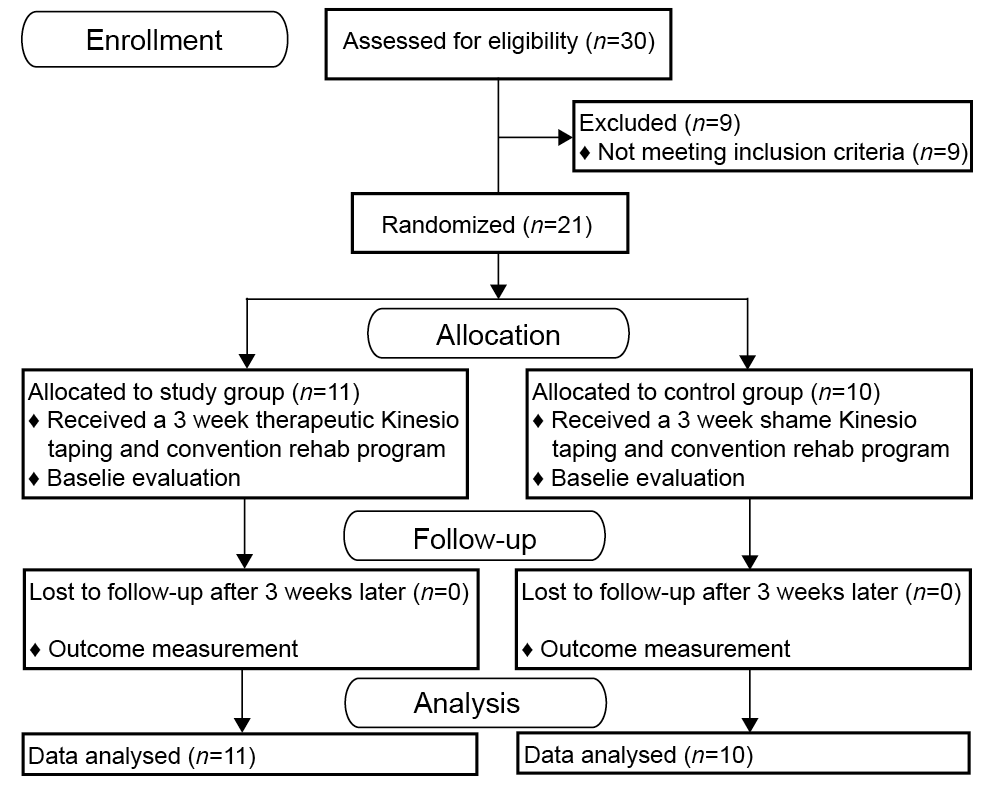
The 21 participants were randomly assigned to 2 groups: a therapeutic KT group and a control group. Concealed allocation was performed using a computer-generated randomized table of numbers created prior to data collection by an investigator who was not involved in the assessment or treatment of the participants. Before treatment and after 3 weeks of treatment, assessments were performed by an independent physician who was blinded to the identity of each group allocation and patients’ clinical information. There was a separate form for outcome assessment, which was given to the assessor during the evaluation. KT was applied by a certified physiotherapist immediately following initial measurements. Taping in both therapeutic KT and control groups was applied by the same physiotherapist, who was not involved in the rehabilitation programme or outcome assessment. None of the participants had received previous KT treatment (Fig. 1).
Fig. 1. Study flow chart. SPADI: Shoulder Pain and Disability Index; PROM: pain-free passive range of motion; NRS: numerical rating scale.
Patients were evaluated in a separate room and the KT was removed before outcome measurement. After the intervention process, all patients were asked which group they thought they had participated in and no statistical difference was noted using χ2 analysis.
In the therapeutic KT group, KT was applied using the insertion-origin muscle and space-correction technique. Nitto Denko kinesiology tape (NITTO Kinesiology Tape, Nitto Denko Corporation, Osaka) (50 mm × 4 m) was used and taping applications were performed using a modified method according to ?im?ek et al. (27). Because biceps tenosynovitis is a common finding in HSP in stroke patients, one tape was applied over the long head and short head of the biceps tendon (28). At first, I-type strips were used with light tension (15–25%) for the supraspinatus with the arm in adduction. The strip was crossed over the line of shoulder joint. A Y-shaped strip was then applied to the biceps and deltoid muscles with light tension (15–25%) using the insertion-origin muscle technique. The head of the second strip was applied to the radial tuberosity where the biceps is inserted. The first tail of the second strip was applied along the short head of the biceps tendon to the deltoid muscle. The other tail of the second strip was applied along the long head of the biceps tendon to the deltoid muscle. Finally, the third strip was applied from the anterior to the posterior shoulder, covering the acromioclavicular joint with a 50–75% stretch (Fig. 2A).
Fig. 2. (A) Therapeutic Kinesio taping for study group. (B) Sham Kinesio taping for control group.
In the control group with sham KT, the participants were given similar taping patterns, but without tension, which did not cover the joints. I-type strips were used without tension for the supraspinatus with the arm in a neutral position. The strips did not cross the shoulder joint. A Y-shaped strip was then applied to the biceps and deltoid muscles without tension and without the joint region involved. The third strip was applied to the lateral deltoid without tension and did not cover the acromioclavicular joint (Fig. 2B). All taping was applied by the same physiotherapist in all participants. Although the taping applications seem different, they were well concealed under clothes, thus we considered the blinding of subjects was not compromised.
Participants were told to leave the tape in situ for 3 consecutive days and then remove the tape, clean the skin, and treat the skin with a moisturizing lotion. The participants went without tape for 1 day for 24 h to allow the skin to recover appropriately, and then new tape was reapplied. The skin was examined after each removal of tape for any changes in skin integrity and rash or allergy due to tape application. Participants from both groups had the tape reapplied twice per week for 3 weeks, for a total of 6 applications.
Both groups underwent identical conventional rehabilitation programmes including physical therapy and occupational therapy sessions, each lasting 60 min per day for 5 consecutive days per week. Speech therapy was administered according to individual needs. The physical and occupational therapists were trained to refrain from commenting on the KT when performing the routine rehabilitation intervention.
Pain intensity. Shoulder pain was assessed according to an 11-point numerical rating scale (NRS) (29). This tool was simple to use and was highly correlated with the visual analogue scale, verbal rating scale, and Faces Pain Scale – Revised. The NRS is considered a valid and reliable pain assessment tool (30). The pain intensity was graded from 0 (no pain) to 10 (the most intense level of pain). Participants reported their pain level at rest and during the movement of the shoulder joint in all directions. The most painful movement score was used for further data analysis. Jensen & McFarland (31) indicated that the highest test-retest reliability was 95% and the internal consistency of coefficient alpha ranged from 0.89 to 0.98 for chronic pain. The minimal clinically important difference (MCID) was 2.17 points for shoulder pain (32).
Shoulder Pain and Disability Index. The Shoulder Pain and Disability Index (SPADI), a self-administered assessment tool, was used to measure pain and disability related to shoulder pathology. The SPADI consists of 5 pain and 8 disability items measured on a visual analogue scale. Pain and disability subscales were calculated as the mean of the corresponding items on a 0–100 scale; the highest score indicating the most severe pain and disability. The total outcome score used for statistical analysis was calculated as the sum of the pain and disability subscales. A systemic review revealed that the intraclass correlation coefficient (ICC) was greater than 0.89 (33). Internal consistency was high, with Cronbach’s α typically exceeding 0.90 (33, 34). An 8-point change in SPADI was reported as the MCID among patients with shoulder pain (35).
Ultrasound examination. Ultrasonography was used as an explanatory measure for the participants in the KT and sham taping groups before and after intervention. Ultrasonography of the shoulder was performed by one physiatrist who had at least 5 years of experience and was certified by the Chinese Ultrasound Academy. A 5–12 MHz high-resolution linear scanner (Toshiba Aplio 300 Model TUS-A300, Toshiba Medical System Corporation, Tokyo) was used for the ultrasound examination, and participants were evaluated while maintaining a sitting posture. The techniques for evaluating shoulder muscles and tendons were adapted from the methods of Middleton (36).
Musculo-tendon pathology. The status of the biceps and supraspinatus patency was evaluated using both longitudinal and transverse views. The findings of the ultrasound examinations were classified as either normal or abnormal (tear or tendonitis). A tear was defined as a discontinuity in the normal homogeneous echogenicity of the tendon, whereas tendonitis was defined as a thickening or hypoechogenicity of the tendon in the absence of a border defect.
The diagnostic criteria of biceps tenosynovitis and subacromial bursitis were adopted from Bruyn et al. (37). Biceps tenosynovitis was defined as tendon sheath fluid accumulation (abnormal hypoechoic or anechoic accumulation relative to subdermal fat; occasionally isoechoic or hyperechoic) in intra-articular material that is displaceable and compressible by ≥ 3 mm. Subacromial bursitis was defined as a bursal thickness ≥ 3 mm. The outcome score used for statistical analysis is the presence or absence of pathology. With respect of accuracy of ultrasound for rotator cuff tendinopathy, a recent meta-analysis combining 5 studies (311 shoulders; arthroscopy or open surgery as reference standard) estimated the overall sensitivity was 0.79 and specificity was 0.94 for rotator cuff tendinopathy (38).
Sub-acromial distance. According to the method described by Kumar et al. (39), the subluxation distance was measured by determining the distance from the lateral border of the acromion to the greater tuberosity of the humerus (Fig. 3). The participant was seated in the same position for physical and ultrasound examination radiographic examination (with the arm in a neutral position, hanging by the side). The outcome score is the distance in mm between the lateral border of the acromion to the greater tuberosity of the humerus. According to a previous study, the normative value for acromial to greater tuberosity is 2.24 ± 0.45 cm (40). The ICC for within-day reliability was 0.98 and minimal detectable change was ± 0.2 cm for the affected shoulder among stroke patients (41).
Fig. 3. Ultrasound measurement of shoulder subluxation. The lateral distance (LD) was measured from the lateral border of the acromion to the greater tuberosity of the humerus. AC: acromion, GT: greater tuberosity.
Pain-free passive range of motion of the shoulder. Pain-free passive range of motion (PROM) of the shoulder was designated as the ROM attained in the most painful position and was measured using a digital goniometer in 6 directions: flexion, extension, abduction, adduction, external rotation, and internal rotation. Five directions of the shoulder joint were measured (flexion, abduction, adduction, internal rotation, and external rotation) while participants were lying in a supine position. In addition, shoulder extension was measured in the side-lying position.
Data analyses were performed using SPSS. Descriptive statistics were used to describe the demographic data and clinical characteristics of the participants. The Wilcoxon signed-rank test for continuous data and the χ2 test for non-continuous data were used to determine baseline group differences. Based on the psychometric standardization properties of the outcome measures used, priority was given to the numerical pain scale, and the SPADI as outcome measures, with the PROM and US used as explanatory outcome measures. Mann–Whitney test was used to compare the improvement in continuous variables before and after intervention in both groups. Wilcoxon signed-rank test was used to compare the difference between groups. The χ2 test was used for comparing ultrasound findings between groups. The significance level was p < 0.05.
Thirty patients with HSP were screened for eligibility between January 2013 and December 2014. Twenty-one patients satisfied the inclusion criteria, agreed to participate, and were randomized into the KT group (n = 11) or control group (n = 10). Fig. 1 depicts a flow diagram of participant recruitment and reasons for ineligibility. No adverse effects due to the taping treatments were reported. All 21 participants completed all 3 weeks of treatment. No significant differences were observed in the demographic data or clinical characteristics between the groups (p > 0.05), as shown in Table I. The pretreatment parameters included pain intensity during the most painful movement. No significant differences were observed between groups in the NRS, pain-free PROM, and SPADI scores of the shoulder at baseline (p > 0.05) (Table II).
Table I. Baseline demographic and clinical characteristics of stroke patients in Kinesio taping and sham taping groups
Table II. Baseline clinical characteristics of participants in Kinesio taping and sham taping groups
Primary outcome measures: numerical pain and SPADI. Significant differences were observed in favour of the KT group regarding improvement in numerical pain (p = 0.008) and SPADI (p < 0.001) scores after treatment. However, no significant between-group differences were observed in the NRS (p = 0.705) and SPADI (p = 0.251) score after intervention (Table II).
Secondary, explanatory outcome measures: pain-free ROM and ultrasound examination. No significant between-group differences were observed in the degrees of pain-free ROM. However, there was significant improvement in degrees of pain-free ROM in flexion (p = 0.008), external rotation (p = 0.006) and internal rotation (p = 0.004) in the KT group. (Table II). Ultrasonography was used to assess the presence of biceps tenosynovitis, supraspinatus tendonitis, and subacromial bursitis, and to measure subluxation distance in the 2 groups. No significant differences were observed in the ultrasound diagnostic findings and the subacromial distance between the 2 groups before and after treatment (Table III).
Table III. Ultrasonography findings of participants in Kinesio taping and sham taping groups before and after intervention
This double-blind, randomized, placebo-controlled study evaluated the effects of KT on the treatment of HSP after stroke. To our knowledge, this was the first study to include ultrasound examination for evaluation of shoulder subluxation. Participants with HSP who received therapeutic KT experienced more improvement in NRS (p = 0.008), shoulder flexion (p = 0.008), external rotation (p = 0.006), internal rotation (p = 0.040), and SPADI (p < 0.001) than the sham KT group. In addition, there was no allergy episode or other specific complaint about KT during the whole study period. This study suggests that KT is generally a safe therapy for treating HSP.
In this study, painful shoulder movements reported by all participants consisted of flexion, extension, abduction, adduction, external rotation, and internal rotation. The pain resulted in a limited ROM of the shoulder in the corresponding directions. These HSP characteristics are in accordance with studies by Lo et al. (42) and Suriya-amarit et al. (43), who reported that shoulder movement was restricted in these directions. Other studies have suggested an improvement in ROM with KT. Merino-Marban et al. (44) reported an immediate increase in dorsiflexion of the ankle in athletes when KT was applied to the calf muscles. In another study, Yoshida & Kahanov (45) suggested that KT provides improved ROM in the lower part of the body.
Numerous studies have focused on taping therapy for post-stroke shoulder pain. However, findings regarding the effects of taping on post-stroke shoulder pain remain controversial. Several studies have suggested positive effects of taping on shoulder pain (46–48). One study and 1 review reported insufficient findings (49, 50). Our study found that the SPADI of stroke patients with HSP can be reduced after 3 weeks of KT intervention. Additional studies with longer follow-up periods and larger populations are necessary.
SPADI is a valid measure for assessing pain and disability in people with shoulder pain, according to a population-based study (51). In a study by Thelen et al. (52), results revealed negative change scores in the SPADI when KT was applied to college students with shoulder pain. In this study, we found significant differences in favour of the KT group according to changes in SPADI scores after treatment, providing evidence of the efficacy of KT in treating HSP in stroke patients.
Although the mechanism of action is unclear, it is thought that KT enhances blood and lymph circulation in the application area by lifting the skin and precluding the conduction of pain at the spinal level through a gate control mechanism (53, 54). Numerous studies have suggested that KT has clinical effects; however, 2 recent clinical systematic review articles reported insufficient evidence to support the use of KT over other modalities in clinical practice (55, 56). In addition, Thelen et al. suggested that KT may be of some assistance to clinicians for improving pain-free active ROM immediately after tape application in patients with shoulder pain (52). However, in the current study, no significant differences were observed in pain-free PROM between the 2 groups after taping treatment. Concerning the variable changes, the therapeutic KT group had more improvement in shoulder flexion (p = 0.008), external rotation (p = 0.006), and internal rotation (p = 0.040) than the sham KT group. A possible reason for this could be that conventional rehabilitation is more effective than KT for improving pain-free PROM in the acute stage of stroke.
We believe that this is the first double-blind, randomized, placebo-controlled clinical trial to examine the effects of KT on HSP by using ultrasonography. Two previous studies have assessed the effects of taping on post-stroke shoulder subluxation (46, 57). These studies applied physical examination to assess the degree of shoulder subluxation. Both studies revealed taping to be a promising adjunct to the management of hemiplegic shoulder subluxation. Our study employed ultrasonography to assess shoulder subluxation, which is considered to be more precise than physical examination. However, our study showed no significant differences in shoulder subluxation between the therapeutic KT group and the control group. In addition, there was no significant difference in biceps tenosynovitis, supraspinatus tendonitis and subacromial bursitis. Thus, the mechanism of pain reduction seems not relate to improved structure. Further research is necessary to clarify the effects of taping.
This pilot study has several limitations that should be addressed. First, the sample size was limited and only the short-term results of KT were investigated. Studies with larger sample sizes and longer follow-up periods are recommended. Secondly, this study focused on acute and subacute stroke patients within 6 months of stroke onset. Therefore, conclusions cannot be drawn regarding chronic stroke patients. Finally, due to ethical considerations, we did not monitor or prohibit the use of analgesic medications. In order to minimize bias caused by medication, no steroid injections were administered to any of the patients during the study period.
Stroke patients with HSP can experience greater reductions in SPADI, and pain, and improvement in shoulder flexion, external, and internal rotation after 3 weeks of KT intervention. Although the effects of taping were limited in the current study, the taping was easy to apply. KT could be an alternative treatment option for stroke patients with HSP.
This study was funded by the Taipei Medical University and Shuang Ho hospital (study number 104TMU-SHH-15).
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize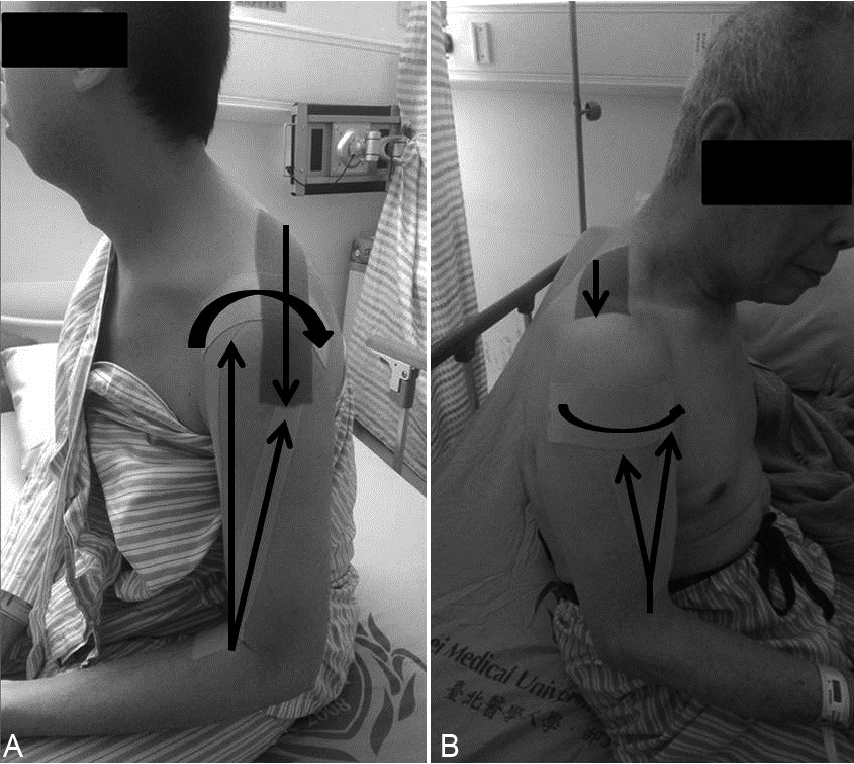 Click to show fullsize
Click to show fullsize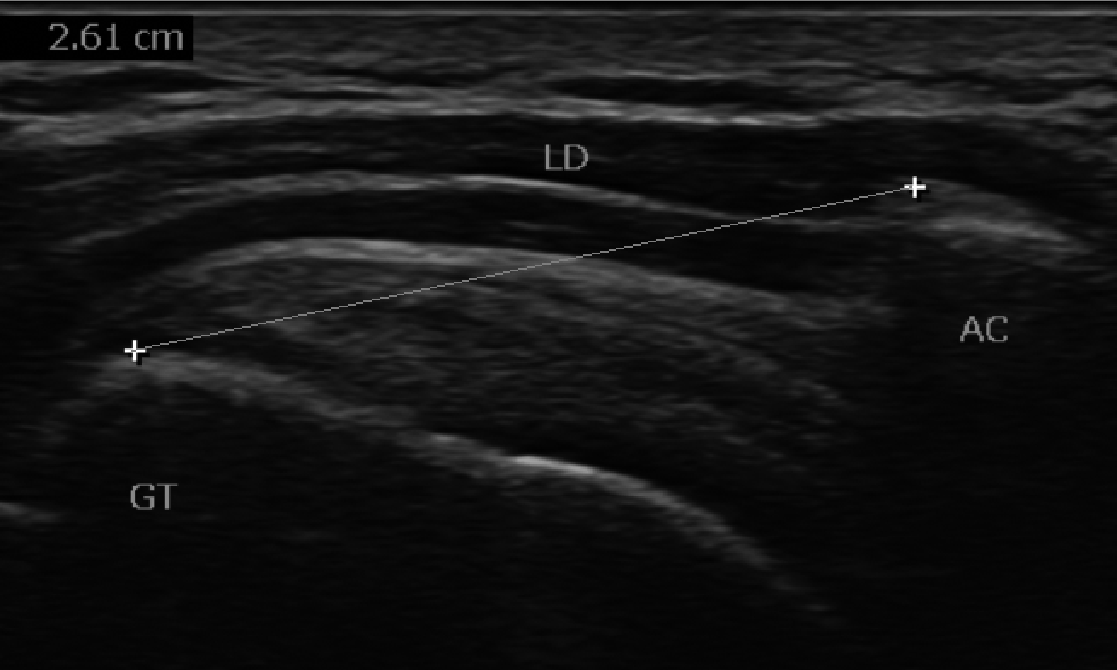 Click to show fullsize
Click to show fullsize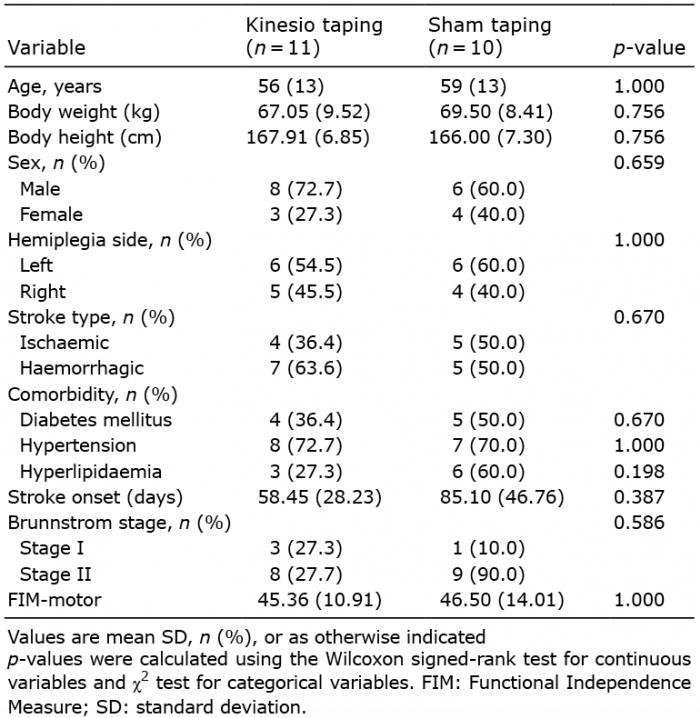 Click to show fullsize
Click to show fullsize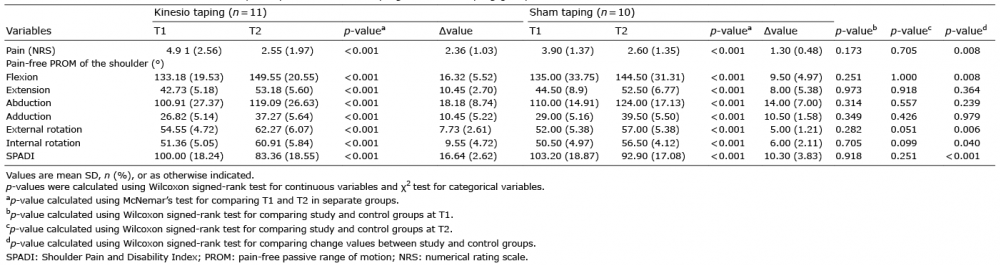 Click to show fullsize
Click to show fullsize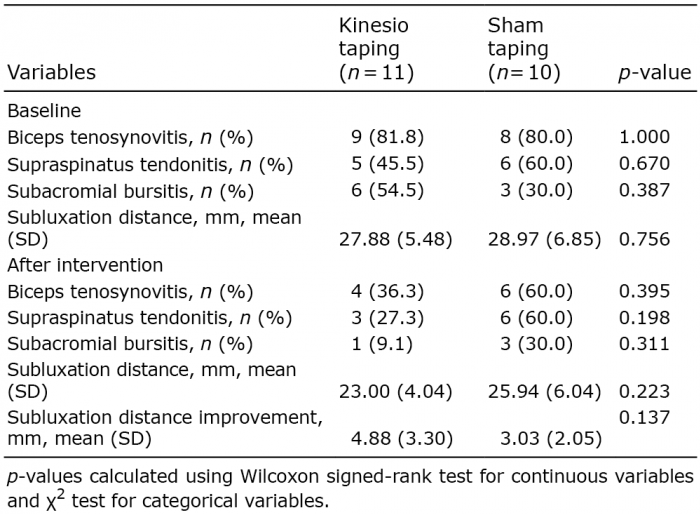 Click to show fullsize
Click to show fullsize