
From the 1Rijnlands Rehabilitation Centre, Leiden, 2Sophia Rehabilitation Centre, 3Department of Medical Psychology and 4Department of Neurology, Reinier de Graaf Gasthuis, Delft, The Netherlands
Objective: Life satisfaction is reduced in stroke patients. However, as a rule, rehabilitation goals are not aimed at life satisfaction, but at activities and participation. In order to optimize life satisfaction in stroke patients, rehabilitation should take into account the determinants of life satisfaction. The aim of this study was therefore to determine what factors are independent determinants of life satisfaction in a large group of patients early after stroke.
Methods: Stroke-surviving patients were examined by a specialized nurse 6 weeks after discharge from hospital or rehabilitation setting. A standardized history and several screening lists, including the Lisat-9, were completed. Step-wise regression was used to identify independent determinants of life satisfaction.
Results: A total of 284 stroke-surviving patients were included in the study. Of these, 117 answered all of the Lisat-9 questions. Most patients (66.5%) rated their life as a whole as “satisfying” or “very satisfying”. More depressive symptoms were independently associated with lower life satisfaction (p < 0.001).
Conclusion: Most stroke-surviving patients are satisfied with their life early after a stroke. The score on the Hospital Anxiety and Depression Scale depression items is independently associated with life satisfaction. Physicians should therefore pay close attention to the mood of these patients.
Key words: stroke; depressive disorder; depression; life satisfaction.
Accepted Dec 7, 2017; Epub ahead of print Feb 17, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Daniëlla Oosterveer, Rijnlands Rehabilitation Centre, Wassenaarseweg 501, NL-2333 AL Leiden, The Netherlands. E-mail: dmo@rrc.nl
Stroke is an important healthcare problem worldwide. In the Netherlands there were 11.7 stroke patients per 1,000 inhabitants on 1 January 2007 (1). A large number of patients return home after discharge from hospital or after a clinical period in a nursing home or rehabilitation centre.
Life satisfaction is reduced in a large proportion of stroke patients (2–4). However, the rehabilitation goals of these stroke patients are not based on life satisfaction, but on the reduced level of activities and participation due to the stroke (5). This emphasis on the consequences of health conditions in terms of activities and participation is based on the International Classification of Functioning Disability and Health (ICF), a model currently used in rehabilitation medicine (6). A small study including 56 stroke patients showed a correlation between this life satisfaction and activity level (7). However, we hypothesize that other factors, such as sex, fatigue or depression, may also influence life satisfaction in stroke patients. These factors were found to be associated with life satisfaction in a population of patients with Parkinson’s disease (8). Greater knowledge of the determinants of life satisfaction shortly after discharge would provide direction to rehabilitation goals. The aim of this large study was therefore to investigate the determinants of life satisfaction in stroke patients shortly after discharge from hospital.
The study population included stroke patients who were admitted to the Department of Neurology, Reinier de Graaf Gasthuis, the Netherlands between 2009 and 2011. This population was previously used to study caregiver strain (9). There were 5 possible treatment options after discharge, for which the indication was made by the neurologist, together with the patient, their relatives and caregivers, the rehabilitation physician and therapists from the hospital: (i) the patient goes home without therapy; (ii) the patient receives mono-disciplinary therapy at home, (iii) the patient attends an outpatient rehabilitation programme at the rehabilitation centre; (iv) the patient participates in a rehabilitation programme in a rehabilitation centre; or (v) the patient participates in a rehabilitation programme in a nursing home. With the exception of the patients who stayed permanently in a nursing home after a rehabilitation programme, all patients were seen 6 weeks after discharge or after finishing the rehabilitation programme by a nurse and a neurologist with special interest in stroke care. Before this appointment patients and their caregivers completed 5 screening questionnaires at home. A standardized history and results of the screening questionnaires were used in order to obtain an inventory of complaints of the patient and caregiver.
All patients were diagnosed with a stroke, defined as: (i) acute onset of 1 or more neurological deficits indicating central dysfunction; (ii) the neurological deficits were present for more than 24 h; and (iii) presence of recent haemorrhage or infarction on computed tomography (CT) imaging or the absence of another explaining cause on CT imaging of the brain executed on the day of admission. In case there was any doubt about the diagnosis, magnetic resonance imaging (MRI) of the brain was performed to confirm the diagnosis. Patients with pre-existing dementia (according to their medical documents) and patients with terminal conditions (malignancy) were excluded from the study. The medical ethics committee approved the study protocol.
Life satisfaction was measured with the Life Satisfaction Questionnaire (LiSat-9). This validated questionnaire is frequently used in stroke patients (10–12). Patients were asked to rate 9 domains of their life (see Table II). The ratings range from 1 (very dissatisfying) to 6 (very satisfying) and the mean of the resulting 9 ratings forms the final score.
Patient characteristics and stroke-related characteristics were collected retrospectively by the principal investigator from the patients’ medical documents. The following patient characteristics were collected: date of birth; sex; presence of hypertension and diabetes; smoking habits; adiposity (defined as body mass index > 25kg/m2); type of house (with or without stairs); presence of a partner or other house-mate; and presence of children. Type and location of the stroke, duration of hospital stay, policy after discharge, Barthel Index during hospital stay, Berg Balance Score during hospital stay, and modified Rankin Scale score (at admission, at discharge and after 3 months) were the stroke-related characteristics collected.
Fatigue was measured using the Fatigue Severity Scale (FSS), a validated self-report questionnaire to measure the severity of fatigue (13). The final score is the mean of the 9 items of the FSS. Each item can be graded between 1 (strong disagreement) and 7 (strong agreement).
The Hospital Anxiety and Depression Scale (HADS) is a questionnaire consisting of 14 items to measure anxiety and depression (14). A score of 8 and higher per subscale indicates a possible anxiety disorder or depression; and a score of 11 and higher indicates a probable anxiety disorder or depression (15, 16).
Activities and participation after discharge was measured using the Frenchay Activities Index (FAI). This reliable test scores the frequency of 15 activities and is validated for measurement at 3 and 6 months (11, 17–19). A shortened version was used, in which the frequency of 10 activities after discharge were measured, leading to a score between 0 (inactive) and 30 (highly active).
All data were anonymized when entered into a database and were analysed with SPSS for Windows. A 2-sided p-value of 0.05 was considered statistically significant.
A step-wise backward regression was used to identify determinants that are independently associated with life satisfaction. In this analysis the mean of the individual questions of the Lisat-9 was used as the dependent variable. For this analysis only fully completed questionnaires were used. As possible determinants we used age, sex, type of cerebrovascular accident (CVA), diabetes, hypertension, type of house, presence of a partner or other house-mate, presence of children, anxiety symptoms measured with the HADS, depressive symptoms measured with the HADS, fatigue complaints measured with the FFS and activity level measured with the FAI. In addition, the mean Lisat-9 was compared in the binary variables and a Pearson correlation between the Lisat-9 and the other variables was calculated.
In addition, several items of the Lisat-9 were analysed in more depth. The answers to the standardized history were also used for these analyses. χ2 tests were used to compare between groups. For these analyses all available answers were used for each domain of the Lisat-9. The Lisat-9 ratings of were grouped as satisfied (rating 4–6) or dissatisfied (rating 1–3).
A total of 284 patients were included in the study (Table I). Of these, 117 answered all of the Lisat-9 questions. There were some differences between the patients who completed the Lisat-9 and those who did not; those who did not complete the Lisat-9 were older, less frequently lived in a house with a stairs, and were more often living alone (Table I).
Table I. Population characteristics
The results of the Lisat-9 are shown in Table II. Most patients (66.5%) rated their life as a whole as satisfying (scale 5 out of 6) or very satisfying (scale 6 out of 6).
Table II. Life Satisfaction Questionnaire and frequencies
The majority of missing values were related to rating their sexual life (n = 126) and their partner relationship (n = 114). The mean score among all completed Lisat-9s was 4.85, with a range of 2–6. Patients who went home without therapy and those who received an outpatient or clinical rehabilitation programme in a rehabilitation centre had a higher life satisfaction score (5.05–5.09) than those who went home with monodisciplinary therapy (4.67) and those who received a rehabilitation programme in a nursing home (4.08; Table III).
Table III. Mean scores with standard deviations (SD) per treatment option on the Lisat-9 and depressive subscale of the Hospital Anxiety and Depression Scale (HADS)
Diabetes mellitus was associated with life satisfaction (p < 0.001) and the FFS, the FAI, the HADS depression score and the HADS anxiety score were correlated with the Lisat-9 (p < 0.001, p < 0.01, p < 0.001 and p < 0.001, respectively; Table IV). In a stepwise-backward regression model the score on the depressive scale of the HADS was the only independent determinant of life satisfaction (β –0.63, p < 0.001).
Table IV. Patient characteristics and their association with life satisfaction as measured by the Lisat-9
The standardized history taken asked patients whether they had financial problems due to their stroke. The majority (n = 189) did not have financial problems due to their stroke, but, despite this, 11 (5.8%) rated their financial situation as dissatisfying (rating 1–3). A further 11 patients reported that they did have financial problems due to their stroke, and, of these, 7 (63.6%) rated their financial situation as dissatisfying. This is significantly more often than in the group without financial problems due to their stroke (p < 0.001).
Patients were asked whether they had problems with sexuality. The majority (n = 103) had no problems, but, of these, 31 (31.1%) were not satisfied with their sexual life. Nineteen patients reported having problems with sexuality, 12 of whom were not satisfied with their sexual life. Although there seems to be a trend towards dissatisfaction with their sexual life when patients had sexuality problems, this difference was not significant (p = 0.07). Dissatisfied patients were more likely to live alone: 24.5% (n = 13) vs 9.6% (n = 9) of the satisfied patients. Of those who did not rate their sexual life (missing value), 52.4% lived alone.
In the majority of patients nothing changed in their family life after their stroke (n = 227, 92.3%), and most were satisfied with their family life (n = 144 of 151, 95.4%). In 19 patients family life was changed after their stroke. Of these 19 patients 14 patients completed the question concerning family life in the Lisat-9. All of these 14 patients answered that they were satisfied with their family life (n = 14 of 14, 100%, p for difference = 0.41). Most patients had children: 172 vs 14 without children. Patients with children were more often satisfied with their family life than those without (94.8% vs 78.6%, p = 0.018).
For 209 patients (73.6%) contact with friends and acquaintances was not diminished, nevertheless 6.3% (n = 11 of the 175 who answered Lisat-9) patients were not satisfied with these contacts. However, more patients were dissatisfied with their contact with friends and acquaintances in patients whose contact with friends and acquaintances was diminished (p = 0.002): 22.2% (n = 8 of the 36 who answered Lisat-9) patients were dissatisfied. One FAI question involves the frequency of social outings. This was answered “never” by 41 patients, and was dissatisfying for 11 patients (26.2%). Thirty-three patients answered “once or twice in the last 3 months”, which was dissatisfying for 2 patients (6.1%). “Three to 12 times in the last 3 months” and “at least weekly” was reported by 31 and 83 patients, respectively, and 1 (6.1%) and 3 (3.6%) patients in these groups were dissatisfied with this. In conclusion, the more social outings patients undertook, the more patients were satisfied with their social life (p < 0.001).
Forty-eight patients (20.3%) had a high score (8 or more) on the HADS-depression scale, indicating that they might have depression. There was no significant difference in the prevalence of high scores between men (19.4%) and women (21.5%). When a more sensitive score of 11 and more was used, 19 patients (8.1%) had depression, and again there was no significant difference between men (7%) and women (9.3%). Patients who received a rehabilitation programme in a nursing home had the highest mean score of depressive symptoms (Table III).
Most stroke patients rated their life as a whole as “satisfying” early after a stroke, and the mean life satisfaction score was 4.85 out of 6. More depressive symptoms were independently associated with lower life satisfaction. Other factors, i.e. age, sex, type of CVA, diabetes, hypertension, type of house, presence of a partner or other house-mate, presence of children, anxiety, fatigue and activity level, were not independently associated with life satisfaction early after a stroke. In 20.3% of patients there was a possible indication of depression, with a higher prevalence in women than in men, although this difference was not significant.
We had no data on life satisfaction prior to the stroke incident or on life satisfaction of a comparable general population with which to compare the current results. However, previously Aström et al. (20) compared 50 patients 3 years post-stroke with a general elderly population and found that stroke-surviving patients had reduced life satisfaction. Contacts with friends and neighbours declined early after stroke, as was seen in 26.4% of our patients. These contacts remained lower than in the general elderly population. In addition, they found that between 3 and 12 months after a stroke both the prevalence of major depression and life satisfaction improved. This is in line with our results, showing that more depressive symptoms are associated with lower life satisfaction.
In agreement with this, Laurent et al. (21) found decreased life satisfaction in 80 stroke-surviving patients in the chronic phase compared with controls, and life satisfaction in these patients correlated with depression. Our study indicates that depressive symptoms and low life satisfaction also correlate early after a stroke.
In addition to the important impact of depression on life satisfaction in stroke-surviving patients, it was previously shown that ongoing depression and a history of having a stroke increased 5-year mortality compared with having only a history of a stroke (22). Furthermore, post-stroke depression might have a negative impact on recovery of daily living and on rehabilitation outcomes (23). Depression in stroke-surviving patients was also associated with higher caregiver strain (24). This emphasizes the importance of diagnosing and treating depression, particularly because depression is more prevalent among stroke-surviving patients than among persons without stroke (25).
Previously it was also shown that illness cognitions, i.e. helplessness, acceptance and perceived benefits, influenced life satisfaction (26). Unfortunately, we had no data to replicate this finding. Another previous study found an association between global life satisfaction and occupational gaps 12 months post-stroke (27). We could not demonstrate an independent association between participation in several activities measured with the FAI. Although this is surprisingly, this finding is in line with a study of Bergström et al. (28), who found low correlations between the number of occupational gaps and life satisfaction in stroke patients after 3–6 months. We also found no independent association between life satisfaction and fatigue shortly after stroke. Previously, no association was found 6 years after stroke (29).
Functional deficits post-stroke could certainly affect life satisfaction and depression, however there was too much missing data regarding our indicators of stroke severity (Barthel Index, Berg Balance Score and modified Ranking Scale) to include these indicators in our analyses.
Next to the impact on patients, we demonstrated previously that caregivers experience more caregiver strain when patients are less satisfied with their lives (9).
In comparison with contact with friends and neighbours, a larger percentage of our population (91.5%) perceived no changes in their family life. Furthermore, patients who did notice changes in family life still rated their family life as satisfying. The consequences of stroke on family relationships was reviewed previously in patients younger than 65 years old (30). In the 13 studies found, 5–54% of patients experienced family problems after their stroke. Our study shows a more positive result. An explanation for this difference could be a difference in age distribution. It is likely that there are different expectations related to family life in younger patients compared with in older patients, as the role of the parent changes. In addition, patients were asked shortly after discharge about the consequences on their family life; negative consequences such as divorce might be clearer after a longer interval.
The differences in life satisfaction and depression between patients with different treatments are interesting (Table III). One can imagine that patients who are discharged without therapy are those who have little neurological sequelae and therefore have a higher life satisfaction and fewer depressive symptoms. The differences between patients receiving the other treatment options might be explained by more attention being paid to depressive symptoms by rehabilitation physicians and by differences in availability of social workers and psychologists. However, these results should be interpreted with care, because we could not include all consecutive patients who were admitted to the neurology department. We included only those patients who were seen by the specialized nurse. However, some patients died during their hospital stay or before this appointment. Other patients stayed permanently in the nursing home after a period of rehabilitation. In addition, some patients were not able or were not willing to attend the appointment with our nurse. Unfortunately, we had no data about these patients. Patients who did not fully completed the Lisat-9 were older and more often living alone than those who did complete the Lisat-9. They often did not answer the questions about their vocational life, sexual life or partner relationship, because they no longer worked, had no sexual intercourse, or had no partner, and therefore thought that they could not answer that specific question. Thus, there may be some bias influencing the general results and the results per treatment option.
In conclusion, most stroke-surviving patients are satisfied with their life early after a stroke. However, life satisfaction is reduced by depressive symptoms. A previous study also found reduced 5-year mortality in depressed stroke-surviving patients compared with non-depressed stroke-surviving patients. Physicians should therefore regularly ask stroke-surviving patients during the rehabilitation process if they have depressive symptoms, and treat depression when diagnosed.


 Click to show fullsize
Click to show fullsize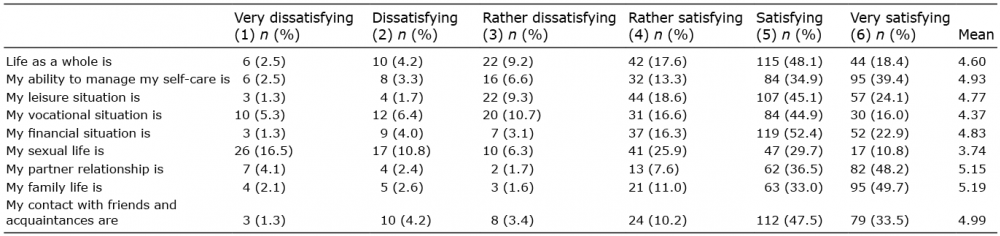 Click to show fullsize
Click to show fullsize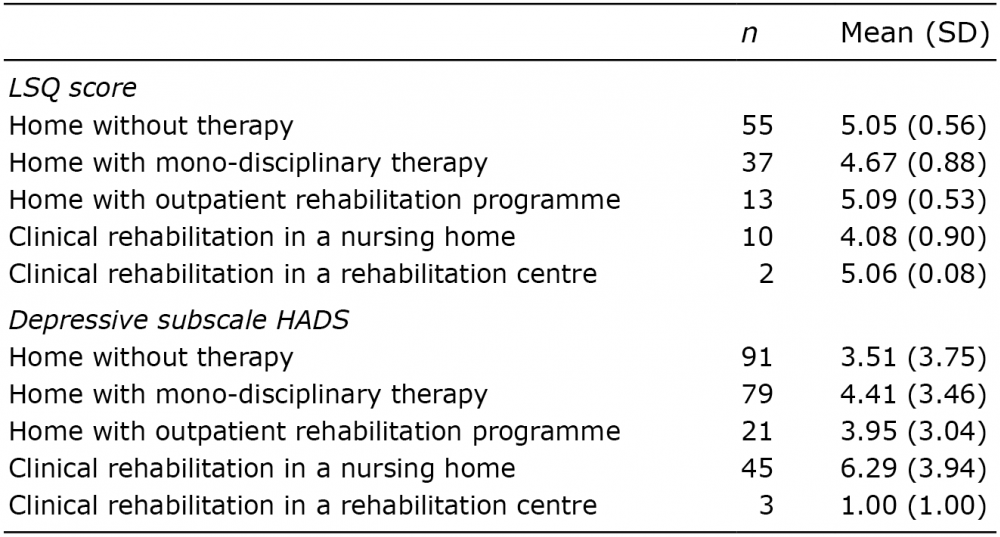 Click to show fullsize
Click to show fullsize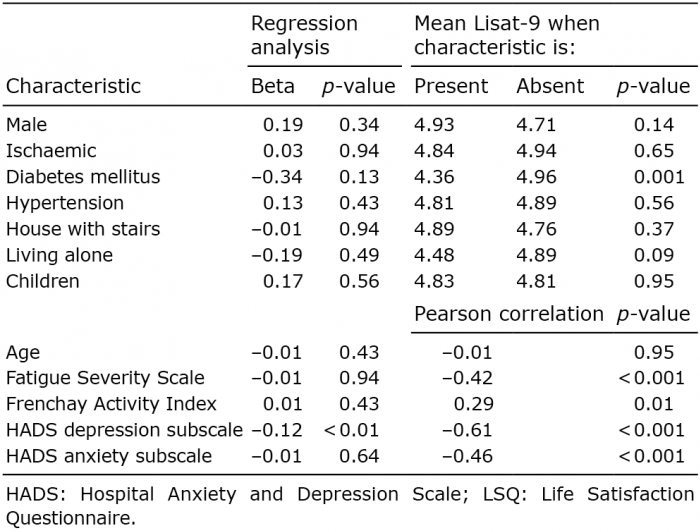 Click to show fullsize
Click to show fullsize