
From the Department of Clinical Neuroscience and Rehabilitation, Institute of Neuroscience and Physiology, Sahlgrenska Academy, University of Gothenburg, Sweden
Objective: To explore motor function, health-related quality of life and impact on activities of daily living 5 and 6 years after reperfusion treatment in patients with stroke.
Methods: A total of 75 patients with first-time stroke received either thrombectomy or thrombolytic treatment at the Sahlgrenska University Hospital in Gothenburg during an 18-month period in 2009–2010. Follow-up involved questionnaires and clinical examinations, 5 and 6 years post-stroke. The results were compared with an individually matched reference group.
Results: At follow-up 54 persons with reperfusion-treated stroke were alive, of whom 31 (57%) answered the questionnaires and 16 agreed to a clinical examination. The Stroke Impact Scale showed impact in several areas, with the emotion domain being the most affected. The reperfusion-treated group reported significantly better strength and hand function compared with the reference group. Of those clinically examined, 44% were dependent in activities of daily living and 38% had cognitive impairment.
Conclusion: Long-term outcome after reperfusion treatment is relatively good, with treated individuals having better strength and hand function compared with a reference group. However, emotional and cognitive problems persist and need to be addressed.
Key words: activities of daily living; long-term; quality of life; reperfusion; stroke; treatment outcome.
Accepted Jan 3, 2017; Epub ahead of print: Feb 17, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Oscar Mühr, Sahlgrenska Academy, University of Gothenburg, Sweden. E-mail: oscar.myhr@gmail.com
In general, there has been a decline in the mortality rate from stroke over the past 20 years in high-income countries, Sweden included (1). However, stroke remains a leading cause of long-term disability worldwide, with at least 10 million people every year having a stroke (1). The distribution of stroke subgroups differs between countries. In Sweden, approximately 85% of strokes are due to cerebral infarction and 15% are haemorrhagic (2). Impairment after stroke is common and the sequelae vary widely (3).
There are different types of reperfusion treatments used for ischaemic stroke in the acute setting. Intravenous thrombolytic treatment is the most common and intra-arterial thrombectomy is an increasingly common treatment. Five major studies published in 2015 showed beneficial results in terms of functional recovery 3 months after combined thrombectomy and thrombolysis compared with thrombolytic treatment alone (4–10). Another study concluded that, based on the results from these 5 major studies, it would be cost-effective to add thrombectomy to standard care, with substantial clinical benefits (11).
Since both thrombectomy and intravenous thrombolysis are relatively new methods, there is an absence of long-term studies regarding the outcome of these treatments (11). Little has been reported on the impact of reperfusion treatment on health-related quality of life (HRQoL) and activities of daily living (ADL) (12). Intravenous thrombolysis has been associated with improved HRQoL (13). Data from persons with stroke and the impact of cognitive deficits on various domains of health outcomes in the long-term are scarce (14).
The overall purpose of this explorative study was to gain a better understanding of the long-term impact of reperfusion treatment, by exploring motor function, HRQoL and impact on ADL, 5 and 6 years after treat
ment.
This explorative cohort study consists of 2 parts. First, the 2 sets of questionnaires sent to the participants’ homes (5 and 6 years post-stroke) were compiled with a retrospective study of baseline characteristics of the participants. Secondly, a clinical examination at a home visit or examination at the Department of Rehabilitation Medicine at Sahlgrenska University Hospital was performed 6 years post-stroke. The guidelines of Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (15) were followed.
The participants were participants in the SALGOT-Extended (16), a cross-sectional study of patients with stroke at Sahlgrenska University Hospital, Sweden, 2009–2010. Inclusion criteria were: age 18 years or older; living within 35 km of the hospital; and first-ever clinical stroke according to the World Health Organization (WHO) (17). For the present study, participants who had an ischaemic stroke and received either a thrombectomy and/or thrombolysis were selected. In total, 75 persons fulfilled the inclusion criteria. Patients treated with a combination of thrombolysis and thrombectomy were included in the thrombectomy-treated group in this study.
Each of the included participants was individually matched with a person from SALGOT-Extended (16) who had not received reperfusion treatment (the reference group). In the matching process the variables were prioritized as follows: stroke severity at admittance, according to the National Institutes of Health Stroke Scale (NIHSS), age, sex, and functional outcome at discharge with the modified Rankin Scale (mRS). Differences between the reperfusion-treated group and the reference group were analysed with Wilcoxon signed-rank test. There were no significant differences between the reperfusion-treated group and the reference group in terms of stroke severity (NIHSS, p = 0.411, individually matched within ± 6), age (p = 0.851, individually matched within ± 7), sex (p = 1.000, individually matched within ± 0) and stroke outcome (mRS, p = 0.504, individually matched within ± 1).
Baseline characteristics were gathered from medical records. Stroke severity was assessed with the NIHSS on arrival at the hospital (18) and with the mRS at discharge from the hospital (19).
The NIHSS (0–46, lower being better) assesses the stroke severity according to the patient’s symptoms. The modified Rankin Scale (0–6, lower is better) is a validated clinician-reported instrument used to measure the degree of impairment in daily activities (19, 20). A mRS score > 3 can be used to define a poor outcome (21).
The first set of questionnaires was sent by post to the participants treated with reperfusion and to the reference group, 5 years post-stroke (median 57.5 months). The set of questionnaires included; European Quality of Life-5 Dimensions (EQ-5D) (22), Swedish Stroke Register questionnaire (23) and Stroke Impact Scale (SIS) (24). A second set of questionnaires was sent by post 1 year later (median 71 months post-stroke) to the reperfusion-treated group (not the reference group) that answered the first set of questionnaires, containing only the EQ-5D and the SIS. This was posted prior to the scheduled clinical examination and reviewed at the time of examination.
An extended version of the original Swedish Stroke Register questionnaire (23) was used in the 1-year follow-up post-stroke. In the present study questions evaluating the participants current living condition, stroke relapse, pain, depression and the rate of return to work were used.
The SIS is a self-reported questionnaire, used to evaluate how the stroke has affected the patient’s health and life (24, 25). The SIS consist of questions with 5 nominal categories in 8 domains: strength, hand function, ADL and mobility, communication, emotion, memory/thinking, and participation, with a total of 59 questions. Each domain is transformed (24) to a value of 0–100, where 100 indicates not being affected by the stroke. The SIS also includes a visual analogue scale (VAS) on which the patients assess total recovery after stroke (0 = no recovery, 100 = full recovery).
The EQ-5D is a standardized questionnaire used to estimate the participants perceived health status and HRQoL (22) and includes 5 domains; mobility, self-care, usual activities, pain/discomfort and anxiety/depression, and a VAS scale on which the patients assess imaginable health status (0 = worst, 100 = best). The EQ-5D has been validated and proven reliable for different diagnostic groups, including stroke (26–28).
During the clinical examination, 6 years post-stroke (median 71 months), the participants underwent a general medical examination including NIHSS (18) and Barthel Index (29) and an interview, complemented with a cognitive screening using Montreal - Cognitive Assessment (MoCA) (30). The interview involved questions of an open nature regarding the stroke and what impact it may have had on their life at the present time. For the participants who completed the questionnaire but declined the examination, their questionnaires were reviewed by phone in the case of missing data or inconsistently answered questions. The MoCA (0–30, higher is better) is a reliable and validated instrument used to evaluate the patient for persistent cognitive problems (30). A MoCA score < 26 indicated cognitive impairment (31). The Barthel index (0–100 higher is better) measures the patients’ independency in ADL and is a valid and reliable instrument, particularly for stroke populations (29, 32, 33). Only the results from the most recently answered questionnaire were presented regarding EQ-5D and SIS. By doing so, some missing data from the questionnaires were supplemented and thereby addressed.
The SIS and EQ-5D answers from the reperfusion-treated group were compared with the reference group, which was involved in the first set of questionnaires (median time 59 months post-stroke). The EQ-5D answers were compared with a study by Burström et al. 2013 (34), in which the EQ-5D answers from the general population of Sweden (in total 45,000 people) have been compiled. The present study was approved by the Regional Ethical Review Board in Gothenburg both in 2008 and in 2013. The principles of the Declaration of Helsinki were followed and all participants gave informed written consent.
Statistical analyses were performed with IBM SPSS Statistics 21 program. A p-value ≤ 0.05 was considered statistically significant. Descriptive statistics were used and differences between groups were analysed with Mann–Whitney U test when the data was ordinal or continuous, and in the case of dichotomous variables the Fisher’s exact test was used.
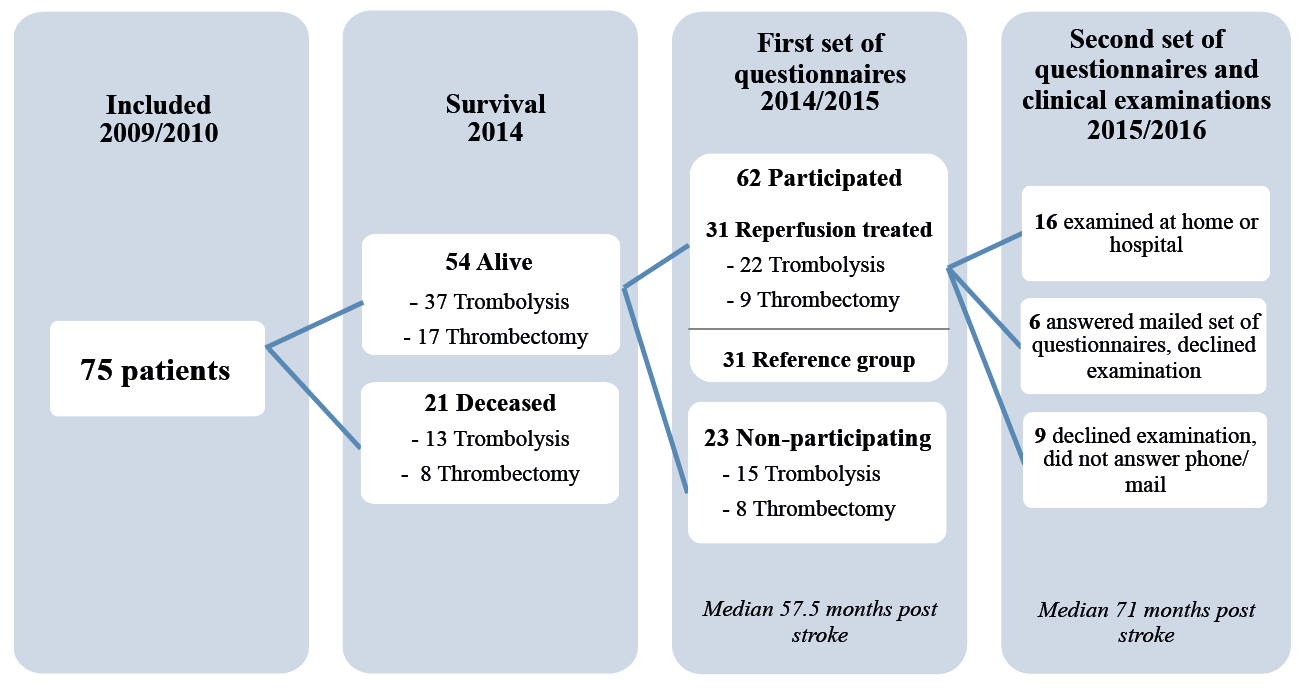
Five years post-stroke, 54 of the original 75 reperfusion-treated persons had survived, of whom 31 (57%) agreed to participate in the first set of questionnaires, 5 years post-stroke. The flow chart in Fig. 1 illustrates the inclusion process. There were no significant differences between participants (n = 31) and non-participatants (n = 23) in age (p = 0.306), stroke severity (NIHSS, p = 0.337) and stroke outcome (mRS, p = 0.730), or sex (p = 0.053). There were no significant differences between the reperfusion-treated and the reference group in any of the domains in the characteristics table (Table I).
Fig. 1. Flowchart of study participants.
Table I. Overview of study participants
Six years post-stroke, 22 participants repeated the questionnaires (second set of questionnaires) and 16 agreed to the clinical examination, of whom 13 agreed to home visits and 3 agreed to be examined at the hospital. When using the most recent questionnaire answer from EQ-5D and SIS, the median time from stroke onset to questionnaire answer was 68 months.
As seen in Table II, the participants who had been treated with reperfusion reported more problems in every domain of the EQ-5D, except for extreme problems with pain/discomfort, compared with the general Swedish population by Burström et al. (34). Likewise, the VAS score from EQ-5D was lower compared with the general Swedish population, mean 79.5 compared with mean of 73.1 in the present study. Twenty-one out of the 30 in the reperfusion-treated group had a VAS-score ≥ 70.
Table II. European Quality of Life-5 Dimensions (EQ-5D) answers presented in frequency, compared with the general population in Sweden presented by Burström (34) and Stroke Impact Scale (SIS) domains’ score 5–6 years post-stroke
No statistical significant differences were seen in the EQ-5D for the reperfusion-treated group compared with the reference group; however, it could be noted that mobility issues were more common in the reference group, whereas the reperfusion-treated group reported having more issues with self-care.
There are still perceived problems in all the SIS domains for the reperfusion-treated group with the emotion domain having the lowest score, i.e. being the worst affected domain (Table II). The reference group reported having more issues in all domains except Emotion and Communication compared with the reperfusion-treated group. However, only the differences in the domains regarding Strength and Hand function were statistically significant (p = 0.017 and p = 0.011, respectively). The reference group only participated in the first posted questionnaires, 5 years post-stroke, resulting in a higher internal dropout (Table II).
Out of the 31 participants treated with reperfusion, 9 had been treated with thrombectomy and the remaining 22 had been treated with thrombolysis. The thrombectomy-treated group initially had a more severe stroke (NIHSS median 18) compared with the thrombolytic-treated group (NIHSS median 6.5). No significant differences could be seen between the 2 groups regarding any of the domains of the SIS and the EQ-5D.
During the clinical examinations, the majority of participants had very mild severity stroke symptoms (NIHSS ≤ 2). Approximately 40% were measured as having issues with dependency in ADL (Barthel Index) and/or suggested cognitive impairment (MoCA) (Table III). Ten participants (62.5%) had a MoCA score of 26 or above and were deemed to not have any cognitive impairment, while the remaining 6 participants were assessed as having a cognitive impairment (MoCA score 15–25).
Table III. Montreal - Cognitive Assessment (MoCA), Barthel Index and National Institutes of Health Stroke Scale (NIHSS) scores from follow-up examination 6 years post-stroke
Approximately 56% were independent in ADL, with a Barthel Index score of 100. The main reasons for a reduced score were occasional bladder incontinence and problems with transfers from lying down to sitting up. Two participants had difficulty feeding and dressing themselves.
The NIHSS score 6 years post-stroke showed that the majority of participants treated with reperfusion had sequelae from the stroke corresponding to very mild severity stroke symptoms. When comparing the stroke severity from stroke onset and the severity of symptoms 6 years post-stroke in Fig. 2, the NIHSS score had decreased for all participants except one. Notably, the participants with highest initial NIHSS score (treated with thrombectomy) had the largest improvement at the 6-year follow-up. Two participants scored higher than the others (NIHSS 7 and 10) 6 years post-stroke, mainly due to being paralysed in 1 or 2 extremities.
Comorbidities, such as osteoarthritis, poor eyesight and obesity, combined with loss of flexibility were reported as factors affecting the answers in SIS. All participants reported still being affected by their stroke. A commonly experienced sequelae was fatigue. Furthermore, dizziness and vertigo were frequent complaints from the participants during their clinical examination. However, a negatively affected balance could not be seen, except in 2 participants who had a positive neurological balance test.
This study shows that patients who have undergone reperfusion treatment have a rather good recovery 5–6 years post-stroke. However, some issues remain regarding mobility, dependency in ADL and cognition. The participants reported problems in all domains of the EQ-5D. There was a significant difference at 6 years post-stroke between the reperfusion-treated group and the reference group, in which the reperfusion-treated group had a better outcome regarding strength and hand function.
The majority (75%) of patients in the reperfusion-treated group presented very mild stroke symptoms 6 years post-stroke. However, the participants experienced that the stroke had an impact on everyday life, which was not fully captured by the measurements. The participants describe symptoms, such as depression and fatigue, compared with prior to stroke. This shows that the instruments available have not covered all aspects of the difficulties experienced after stroke that may affect HRQoL, as well as ADL and experienced motor function. As seen in a study evaluating the consequences of mild stroke, hidden dysfunctions were not easily discovered within the hospital context, due to, among other factors, ceiling effects from measurement scales such as the Barthel Index (35).
The proportion of patients with cognitive impairment in the present study (37.5%) can be compared with the already high prevalence of persons with cognitive impairment without dementia in Sweden, where 25% of a population of twins over 65 years of age were assessed as cognitively impaired (36).
The majority of participants were independent in all domains of ADL. Only 1 participant had severe dependency issues that resulted in a need for care at a nursing home. The SIS ADL domain showed that the participants still experienced some problems, but that they were considerably better than what was experienced by the participants in the larger 12 months post-stroke follow-up (n =204) by Guidetti et al. (37). It is not known whether the different findings are due to a low study sample size in the current study, or are the result of better treatment or adaptation to new life situations. The current study showed that 44% of the 16 patients who were clinically examined were dependent in 1 or more activities of the Barthel Index. A similar outcome, which showed that 55% of all persons with stroke had dependency issues in ADL, can be seen in the Swedish Stroke Register annual follow-up from 2014 (23).
Both the participants treated with reperfusion and the reference group reported lower results in the VAS score from EQ-5D compared with the general Swedish population, as well as having higher frequencies of perceived problems and severity levels in all 5 categories (except in the item regarding extreme problems with pain/discomfort). Fischer et al. (38) considered an EQ-5D score over 70 to be an indication of good HRQoL, and this was the case in 70% of the reperfusion-treated group in the present study. The overall high independency in ADL and low severity of stroke symptoms for the majority in the present study may be one factor explaining the good VAS score, together with the acceptance of their diagnosis that, in general, the persons with stroke have achieved by 6 years post-stroke.
When comparing the reference group with the reperfusion-treated group, the hand function and strength domains in the SIS showed statistically significant differences, with a better outcome for the reperfusion-treated group. It was assumed that the mobility domain would also be affected, since this domain is associated with strength; however, this domain did not show a significant p -value (p = 0.055).
This study has some limitations. Comorbidity was not taken into consideration, and this may affect the questionnaire answers when exploring the outcome post-stroke. The modest sample size made it difficult to distinguish any significant differences in the outcome for thrombectomy compared with thrombolytic treatment. Furthermore, the study was limited by the fact that the reference group was created after data collection had already taken place, which meant that the reference group was not followed up with a second set of questionnaires and clinical examinations.
A larger study population is needed to better explore the outcome and to understand what type of treatment would have the best results in patients with stroke. Furthermore, for future studies it would be interesting to include data on comorbidity, especially diseases that might impact on mobility and ADL, as well as to factor in the time of ischaemic exposure before treatment when comparing the outcomes.
In conclusion, the majority of participants treated with reperfusion had a good HRQoL and the severity of their stroke symptoms was very mild 6 years post-stroke. However, more than one-third reported mobility issues and the overall strength domain was more affected than the mobility domain. Furthermore, issues remain with many being dependent in ADL and cognitively impaired. The reperfusion-treated group reported having a significantly better outcome regarding the SIS domains strength and hand function compared with the reference group. Long-term outcome after reperfusion treatment is quite good, but there are emotional and cognitive problems that persist, as well as a need for a contact with primary healthcare providers that ought to be addressed.
This study was funded in part by the Swedish Heart and Lung Foundation and the Swedish Brain Foundation.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize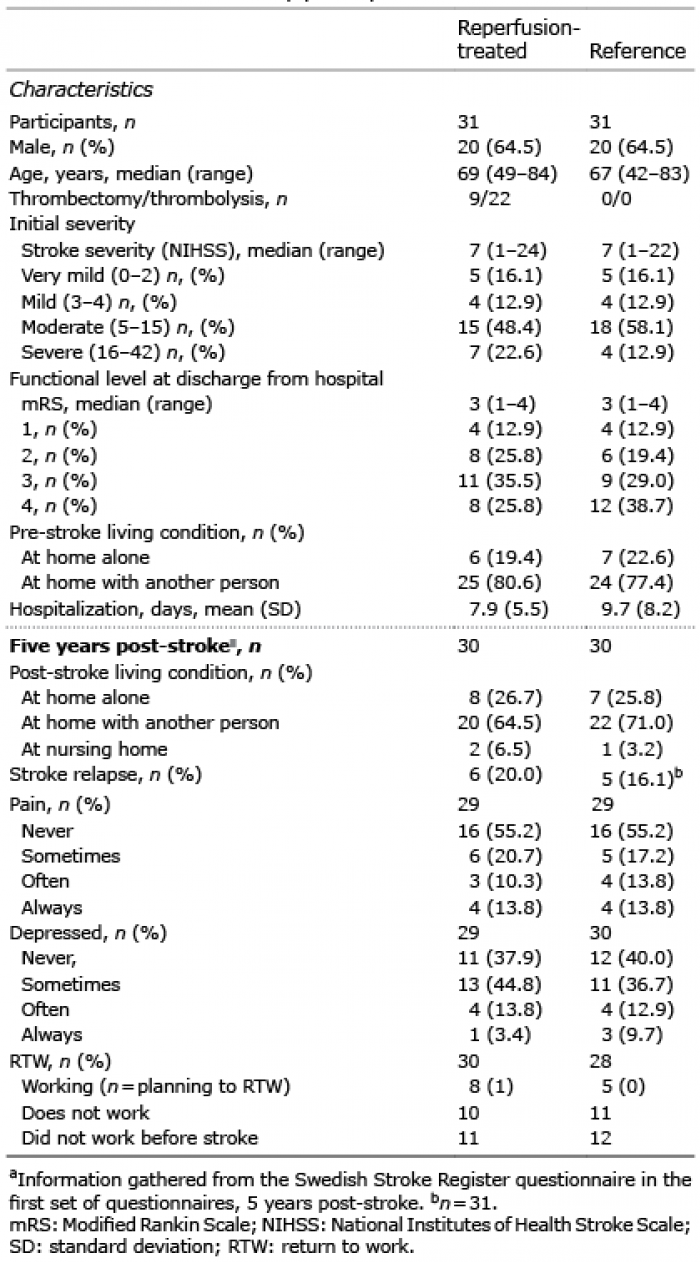 Click to show fullsize
Click to show fullsize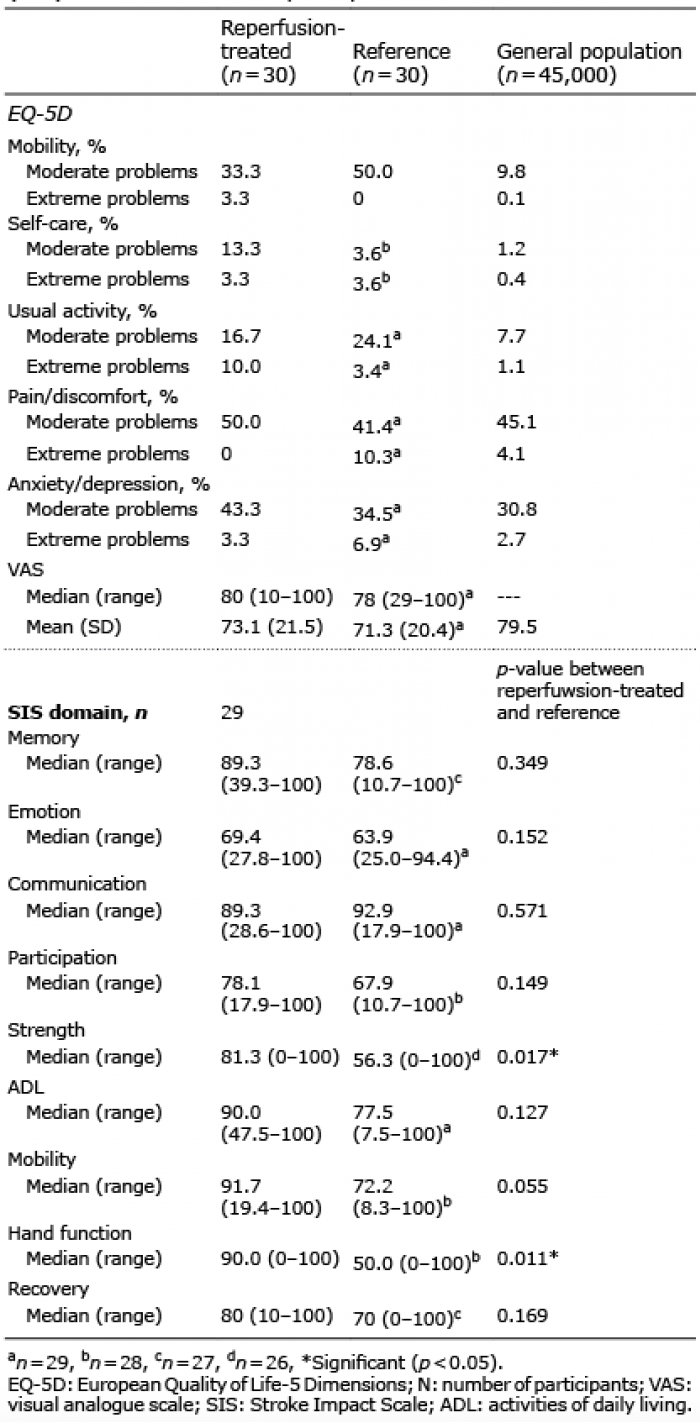 Click to show fullsize
Click to show fullsize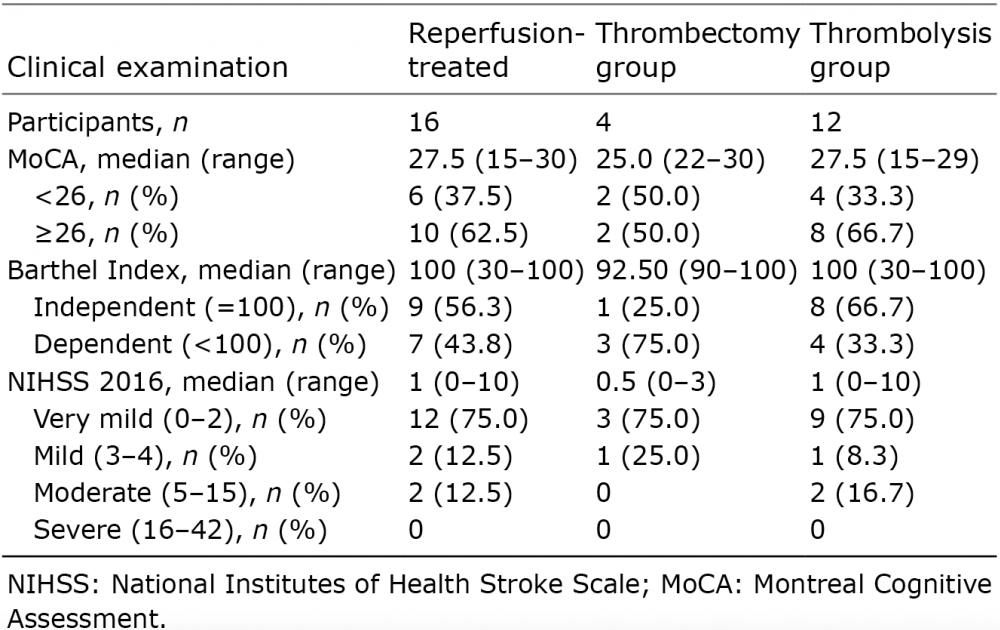 Click to show fullsize
Click to show fullsize