
From the 1Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Rehabilitation, 2Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Neurology, Nijmegen, The Netherlands
Introduction: Balance impairments are common in patients with hereditary spastic paraplegia and are among the most debilitating symptoms, as they frequently result in falls and fall-related injuries. Several features of hereditary spastic paraplegia contribute to balance impairments and multiple treatment options exist. However, an overview of these underlying mechanisms and their treatment is currently lacking.
Methods: This paper reviews the pathophysiology, diagnostic workup, and management of balance impairments in hereditary spastic paraplegia. Recommendations are based on scientific evidence, when available, and otherwise reflect practice-based evidence supported by clinical experience.
Conclusion: Through diligent history-taking and clinical examination, followed by multidisciplinary treatment tailored to the identified underlying mechanisms, balance capacities can be improved in patients with hereditary spastic paraplegia and at least a proportion of falls can be prevented.
Key words: hereditary spastic paraplegia; HSP; balance; falls; treatment; fall prevention.
Accepted Mar 13, 2017; Epub ahead of print Apr 27, 2017
J Rehabil Med 2017; 49: 369–377
Correspondence address: Jorik Nonnekes, Radboud University Medical Centre, Donders Institute for Brain, Cognition and Behaviour, Department of Rehabilitation, Expertise Centre for Hereditary Movement Disorders, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: Jorik.nonnekes@radboudumc.nl
Hereditary spastic paraplegia (HSP) is a diverse group of inherited disorders that are clinically characterized by progressive spasticity, muscle weakness and reduced proprioception in the lower extremities (1, 2). In addition, many patients experience urinary problems related to a spastic bladder. The common underlying mechanism of these symptoms is retrograde axonal degeneration of the corticospinal tracts, posterior spinal columns and, to a lesser extent, the spinocerebellar fibres (3, 4). HSP can be divided into pure (uncomplicated) and complicated forms, depending on the presence of other neurological symptoms, such as ataxia, optic atrophy, mental retardation, extrapyramidal signs, dementia, deafness and epilepsy (2). The first presenting symptoms and signs of HSP are subtle, with development of leg stiffness and minor gait impairments. Although the disease may manifest at any age, the first symptoms and signs mostly occur before the age of 40 years (5–7). As the disease progresses, balance impairments develop, which may result in falls and fall-related injuries. Unfortunately, the prevalence of balance impairments and frequency of falls in HSP has, to our knowledge, not yet been studied. Moreover, the consequences of balance impairments and falls have been mapped insufficiently, but clinical experience shows that these may seriously impact on daily life, as they result in fall-related injuries, fear of falling, reduced mobility (approximately 10% of the patients with pure HSP become wheelchair-bound (8)), loss of independence, and reduced quality of life.
Most publications about HSP concern its genotypes and genotype-phenotype coupling. Far fewer publications have considered the functional consequences of HSP, and most of these address the (management of) spastic gait impairments such as “foot drag”, “crouch gait”, and “scissoring” (4, 9, 10). Very few publications have been focused on balance impairments and related falls as specific consequences of HSP (11). To fill this gap, we elaborate here on the pathophysiology, diagnostic workup, and management of balance impairments and falls in patients with HSP. This review is based on scientific evidence when available (see Box 1), and otherwise reflects practice-based evidence supported by clinical experience.
Box 1. Search strategy
In general, falls can be the result of intrinsic or extrinsic risk factors, or a combination of both (12). An icy pavement, wet bathroom tiles, or loose carpets are examples of extrinsic risk factors that may cause a trip or slip, inducing a fall. However, as in other neurological conditions such as stroke and Parkinson’s disease (13, 14), falls in HSP are mainly due to intrinsic risk factors. These intrinsic factors hamper feet-in-place balance responses and contribute to suboptimal stepping responses when a feet-in-place response is no longer sufficient to maintain balance. In HSP, 4 main contributors to balance impairments can be identified.
The first intrinsic risk factor is spasticity, which can have a direct (negative) influence on balance responses when fast muscle stretch, induced by active or passive body perturbations, results in destabilizing muscle responses. This is best documented for “toes-up perturbations”, during which rotation of the support surface induces fast ankle dorsiflexion and backward body perturbation (15). In healthy subjects, stretch-induced calf muscle activity is suppressed during these toes-up perturbations, allowing ventral leg and trunk muscles to pull the body forward and restore balance (16, 17). However, in patients with HSP, there is insufficient suppression of stretch-induced calf muscle activity due to reduced corticospinal inhibition of stretch reflexes, as part of the so-called “upper motor neurone syndrome” (11, 18). This may result in a destabilizing plantar flexion moment at the ankles that counteracts the ventral muscles, which pulls the centre of mass (further) backwards, and threatens balance (11). As such, toes-up perturbations may cause backward falls in HSP. However, as toes-up perturbations in daily life are relatively rare, their potential contribution to actual fall risk is probably limited. Moreover, the available evidence suggests that calf muscle spasticity does not contribute to balance impairments in HSP during backward balance perturbations induced by forward support-surface translations (when the calf muscles are shortened instead of stretched) or by any type of forward body perturbation (11). Hence, the direct contribution of spasticity of distal musculature to balance impairments in HSP seems limited. However, spasticity of proximal musculature (e.g. the adductors or hamstrings) may directly contribute to balance impairments as it hampers the capacity to make sufficiently fast stepping responses in situations where feet-in-place responses do not suffice. For example, hip adductor spasticity may reduce the efficacy of balance-correcting side-steps upon lateral perturbations and hamstrings spasticity may seriously limit the capacity to make a forward step of sufficient length upon forward body perturbations.
Although the direct contribution of leg muscle spasticity to impaired feet-in-pace balance may be limited, spasticity can indirectly contribute to balance impairments and falls in HSP, because it predisposes to the development of muscle contractures and joint deformities (the second risk factor), which negatively influences the ability to perform feet-in-place balance responses as well as stepping responses. The most commonly encountered deformity in patients with HSP is pes equino(varus) due to structural shortening of the calf muscles, long toe flexors and/or tibialis posterior muscle. Structural pes equinus results in a (severely) reduced base of support, particularly when the heels do no longer have contact with the ground. This situation prevents the use of normal “ankle strategies” for maintaining feet-in-place balance in the sagittal plane, requiring the recruitment of less efficient “hip strategies”. In addition, patients may adopt compensatory postural adjustments at the knees (e.g. hyperextension), hips (e.g. hyperflexion) and trunk (e.g. forward lean) in order to maintain balance when standing. In some patients, there is varus deformity at the ankles, which can be aggravated by a concomitant pes cavus. As a consequence, the base of support in the frontal plane will be reduced, which will impair the use of ankle strategies during one-legged stance, for example during the single-support phase of gait. Apart from a direct influence on balance, pes equinovarus obviously predisposes to gait impairments such as “foot drag” and “hooking”, which increases the risk of tripping over one’s own feet while walking or when making a balance-correcting stepping response. Moreover, varus deformity at heel strike and during the stance phase of gait will predispose to ankle instability, ankle sprain, and falling sideways. In addition to pes equinovarus, knee flexion contractures (due to shortened hamstrings) and hip adduction contractures (due to shortened hip adductors) are common in patients with HSP. In our experience, their impact on balance is, as with spasticity of proximal musculature, stronger through impaired stepping responses than through impaired (feet-in-place) equilibrium reactions.
The third intrinsic risk factor for balance impairments and falls in HSP is muscle weakness. Indeed, there is evidence that reduced calf muscle strength is associated with postural instability during forward body perturbations induced by backward support-surface translations (11). In contrast, however, the relationship between tibialis anterior strength and backward body perturbations (induced by forward support-surface translations) appears to be less clear (11). Generally, muscle weakness does not seem to be the major impairment in patients with HSP, even though the name “paraplegia” suggests otherwise. There is growing support for the notion that muscle weakness induced by lateral corticospinal tract dysfunction can be compensated by reticulospinal activation originating from the brainstem (19, 20). Indeed, there is strong evidence for intact reticulospinal control over voluntary and postural leg movements in patients with HSP (21–23). Hence, compensatory reticulospinal activity may be quite effective to produce sufficient muscle strength, although less differentiated in comparison to the more selective corticospinal control over muscles (24). However, as with other neurological diseases (25), patients with HSP are prone to sarcopaenia and loss of muscle strength due to “disuse” induced by lack of activity. Lack of activity can have several reasons, one of which is fear of falling. Disuse-induced muscle weakness commonly induces a vicious circle in which balance impairments become worse, resulting in falls and fear of falling, and eventually more disuse.
A fourth, least known or appreciated, risk factor for balance impairments in HSP is reduced proprioception, resulting in delayed postural responses. We evaluated balance responses to forward and backward body perturbations in patients with pure HSP, and found that patients were less stable than healthy aged-matched control subjects, as reflected by a larger percentage of trials in which they had to take a corrective step or grasp a handrail (21). Moreover, compared with controls, their postural responses to backward and forward perturbations were, in mean, delayed by 38 and 34 ms, respectively (21). This delay may appear small in absolute terms, but entails a relative increase of 25–30% compared with healthy subjects. This delay in postural responses could theoretically be the result of a slowness of signals in the afferent (posterior spinal columns) or efferent (reticulospinal) tracts, or in a combination of both. By combining balance perturbations with an auditory startling stimulus we were able to disentangle both mechanisms (19, 22, 26). The results indicated that delayed postural responses in patients with HSP are primarily due to a delay of signals in the posterior spinal columns, i.e. due to impaired proprioception (21).
Overall, we believe that impaired feet-in-place responses in patients with pure HSP are mainly due to delayed postural responses and to the biomechanical influence of predominantly distal muscle contractures. In contrast, the contribution of distal muscle weakness and spasticity seems to be restricted to specific types of body perturbations. Nevertheless, spasticity, shortening, and weakness of the proximal leg muscles may hamper the capacity to make sufficiently fast and large stepping responses in situations where feet-in-place responses do not suffice. Obviously, it should be kept in mind that ataxia, extrapyramidal symptoms and/or visual impairments may contribute to balance impairments in patients with complicated forms of HSP.
Although balance impairments and falls in HSP are common, the presence and relative contribution of the various intrinsic and extrinsic risk factors may vary considerably between patients. Therefore, history-taking and clinical examination is necessary to determine the contribution of each factor to individual balance impairments (12). In this diagnostic process, it is important to value each risk factor as well as their possible interactions, as often multiple factors are relevant for individual patients.
In both healthy populations and in patients with a neurological disorder, the strongest risk factor for a fall is the presence of a fall-history (27, 28). It is therefore essential to ask whether the patient has fallen during the last year(s) and, if so, whether he or she has fallen recurrently, under which circumstances, and whether any injury has ever occurred. In the case of recurrent falls, it is important to establish whether there is a typical pattern or direction to the fall (12). Even if the patient indicates not to fall, the identification and treatment of risk factors is still important for the prevention of future falls. Patients with HSP can usually indicate whether they are easily “pulled backward” or whether they fall forward or sideways instead. It is not useful to ask for underlying mechanisms (e.g. spasticity, slowness, or contractures), as patients find it difficult to judge any of such possible relationships. Yet, fall circumstances, fall pattern, and type of injury can point towards a specific mechanism such as “backward instability”. When a patient has fallen, it is important to ask whether he or she recalls hitting the floor, in order to exclude loss of consciousness due to head trauma. Because patients with HSP rarely lose their consciousness when falling, other underlying mechanisms such as vasovagal syncope or cardiac arrhythmias should be suspected. As in the general population, use of medication, especially polypharmacy, can increment fall risk and, thus, an evaluation of prescribed drugs should take place. Benzodiazepines and antidepressants are notorious in this respect (29), in addition to neuroleptics, antihypertensive medication, and anti-arrhythmics (30). In addition to intrinsic factors, it is important to screen for the presence of extrinsic factors, for example the type of footwear and the home situation. It is not uncommon to discover that patients who experience recurrent falls live in a house with loose carpets and no grab rails in the bathroom or toilet.
Finally, it is informative to inquire about the impact of balance impairments, particularly fear of falling and a related reduction of indoor and outdoor activities. In this way, the clinician is also able to screen for disuse. In fearful patients, fall frequency is not an adequate measure of balance problems, as these patients have often adjusted their lives in such a way that falls hardly occur. The downside of this adjustment is, however, a seriously reduced quality of life, both for themselves and their relatives, as well as an enhanced risk of co-morbidity related to immobility, such as cardiovascular disease, osteoporosis and sarcopaenia, reinforcing a vicious circle of functional incapacity and inactivity.
When the patient’s history is suspicious of balance impairments, a thorough clinical examination is mandatory to confirm the presence of balance impairments and to identify underlying mechanisms. Table I provides an overview of useful clinical tests of balance, gait and neurological functions.
Table I. Key elements of the clinical examination in patients with hereditary spastic paraplegia
A useful test to indicate the presence of balance impairments is assessing the ability to rise from a chair, to stand on 2 legs as well as on 1 leg with the foot flat on the ground and eyes open. An inability to perform such tests without any external support strongly suggests the presence of balance impairments. A key element in the clinical assessment of postural instability is the retropulsion test, in which the assessor induces a balance perturbation by applying a (preferably unexpected) shoulder pull (31). The absence of a balance corrective step or a suboptimal quality of the balance corrective step is indicative of postural instability. In patients with HSP, we recommend to perturb the patient not only in the backward direction, but also in the forward and lateral directions to test the quality of the stepping responses in the other directions as well. By sitting on a stool in front of the patient the clinician can easily pull the pelvis forward or apply sideways forces to the pelvis, while the patient is able to grasp the shoulders of the clinician or the clinician can stop a falling motion when needed. As a more elaborate test we advise performing the mini-BESTest, consisting of a 14-item, 3-point rating scale evaluating 4 sub-items: transitions/anticipatory postural control, reactive postural control, sensory orientation, and stability in gait (32). Another option is the Berg Balance Scale (BBS) (33), which is a standardized 14-item, 4-point rating scale to indicate the presence of postural instability while sitting, standing and making postural movements in place. Both the mini-BESTest and the BBS include several elements of the tests described above. However, no standardized balance test has yet been validated for patients with HSP.
Balance capacity while walking can be assessed by testing tandem gait (i.e. the ability to take 10 consecutive steps along an imaginary line without one or more side-steps). This test is very sensitive for subtle balance impairments and often no longer possible in patients with HSP. Of course, the gait pattern should be observed for the identification of specific gait impairments that increase the risk of tripping and falling, such as foot drag, hooking of the feet, and excessive scissoring with collision of the knees.
The 4 main risk factors for balance impairments in HSP must always be identified by a systematic evaluation. We recommend assessing muscle tone of distal and proximal leg musculature using the Modified Ashworth Scale (MAS) (34), to evaluate joint mobility with goniometry using the Debrunner notation (35), and assessing muscle strength using the Medical Research Council (MRC) scale (36). Although both the MAS and the MRC scales have been criticized for their lack of reliability and sensitivity (37), alternative clinical tools for measuring muscle tone (e.g. the Tardieu scale (38) and strength (e.g. hand-held dynamometry) are quite time-consuming to be applied to all joints of the lower limbs and do not necessarily provide more reliable information. Importantly, with regard to management, the clinician should try to carefully discriminate loss of muscle length (contracture) from increased muscle tone (spasticity) using goniometry for all relevant muscle groups, with the calves evaluated with both an extended (gastrocnemius) and flexed (soleus) knee, preferably in a supine position. Regarding the evaluation of proprioception, it is useful to evaluate vibration sense at the lateral malleolus and at the first metatarsophalangeal joint. An easy way to evaluate the contribution of impaired proprioception to balance impairment is Romberg’s test, in which the clinician evaluates body sway and the presence of balance corrective movements of the head, trunk and arms while the patient stands erect with the feet together and the hands by the side. This test is performed with eyes open and closed and is considered positive when body sway increases to the extent that a patient tends to fall with the eyes closed compared with when they are open. A positive test is indicative of balance impairments due to sensory dysfunction and, thus, useful to find proof of impaired leg somatosensation in HSP. Nevertheless, a false-positive outcome may occur due to uncertainty or fear, while a false-negative outcome may be due to insensitivity to subtle sensory deficits. One study did not find increased postural sway in 4 patients with HSP compared with controls (18), but future studies are needed to further map postural sway in patients with HSP, both in mildly and severely affected patients.
Another functional test that is sensitive to somatosensory deficits is comparing comfortable gait speed with and without a walker. Although a walker may provide mechanical support and increase the base of support while walking, its most important influence is often the provision of sensory feedback through the upper extremities especially in patients that do not really lean on the walker. When such patients walk much faster with a walker than without, this finding is suspicious of impaired leg somatosensation. In the same way, providing “a finger tip” of support to the hand of a patient while standing or walking is also a strong indicator of reduced somatosensation (39), if it leads to better postural stability and higher gait speed.
As outlined in the introduction, patients with a complicated form of HSP can have a wide variety of other symptoms in addition to their spastic paraparesis, such as ataxia, signs of parkinsonism or visual disorders. As these symptoms may significantly contribute to the balance impairments, it is important to screen and monitor them and, if present, to manage treatable symptoms accordingly (this will not be covered in the management section of this paper).
In most patients, history-taking and clinical examination will be sufficient to obtain a good general overview of the presence and severity of the balance impairments and of the underlying risk factors. Yet, a more in-depth evaluation of balance impairments may be conducted with posturography.
Using “static posturography” equipment for recording quiet standing (40), body sway can be quantified and compared with reference values obtained from healthy, age-matched individuals. In addition, the Romberg quotient can be determined, which is the ratio between the body sway assessed with eyes closed divided by the sway assessed with eyes open (41). Such an instrumented Romberg quotient is much more sensitive than the clinical Romberg’s test, but the necessary equipment may not be available in many clinical practices.
So-called “dynamic posturography” is a technique that employs physical perturbations of stance (often by a motorized balance platform) to systematically and quantitatively evaluate both feet-in-place balance responses and stepping responses. Although this technique has proven its value for research purposes, it has so far no clear additional value for clinical practice in comparison to the tests described above (40). However, when balance impairments and gait impairments coincide, or when gait impairments frequently result in falls, instrumented assessment of the kinematics (joint motion), kinetics (joint moment of force and power) and muscle activations (electromyography) during walking (instrumented “gait analysis”) can be useful to analyse specific gait impairments to indicate the need for well-targeted interventions (e.g. focal spasmolysis, ankle-foot orthosis) (42, 43).
Adequate management of balance impairments and falls in patients with HSP will greatly depend on the identification of risk factors, as described above. In this section, we discuss the treatment options based on each of these factors. The evidence for these treatment options is sparse, because very few studies have been performed and the available studies are non-randomized. In addition, the evidence of these interventions on balance performance in other patient groups with an upper motor neurone syndrome is also sparse, as most studies evaluated the effect on gait and not on balance control or the prevention of falls (43–45). Hence, most treatment options are based on expert opinion.
If a patient’s history and clinical examination is indicative of calf muscle spasticity contributing to a tendency to fall backwards, focal spasmolysis of the calf muscles must be considered. The main treatment option is neuromuscular blockade by the administration of bilateral botulinum toxin type A (BTX-A) injections in the gastrocnemius and soleus muscles to reduce the amplitude of the balance destabilizing responses. The efficacy of these injections has, however, not yet been proven. We found 10% improvement of comfortable gait speed after such injections in patients with HSP, but no improvement in the BBS, dynamic posturography, or the Activities-specific Balance Confidence scale (ABC) (46). Despite the absence of a significant effect at group level on all balance-related outcomes, it is our clinical experience that well-selected individual patients with destabilizing calf muscle spasticity and a relative mild pes equinus contracture may profit from focal spasmolysis and subsequent stretching exercises of the calf muscles with regard to their backward postural stability. This notion is supported by a recent retrospective study reporting that focal spasmolysis with BTX-A combined with physiotherapy aimed at optimizing joint mobility of the treated segments helps to acquire an adequate postural alignment in patients with HSP (47). In addition to intramuscular injections with BTX-A, chemical or thermal neurolysis of the tibial nerve and selective surgical neurotomy of specific branches of the tibial nerve are techniques to reduce disabling calf muscle spasticity (48, 49). However, chemical or thermal neurolysis carries the risk of inducing sensory deficits and/or neuropathic complaints, while selective neurotomy is complex and performed only by very few expert teams worldwide.
As mentioned above, spasticity of the proximal muscles may hamper stepping responses in both the sagittal and frontal planes. As such, it would intuitively be right to apply focal spasmolysis by intramuscular BTX-A injections (followed by stretching exercises) for instance in the hamstrings to improve forward stepping and in the hip adductors to improve lateral stepping in individual patients with HSP. Currently, we are conducting an uncontrolled pre-post trial to study the efficacy of bilateral BTX-A injections in the hip adductors to improve spontaneous gait width as well as side-stepping responses upon lateral body perturbations in patients with HSP and hip adductor spasticity (Toetsingonline.nl: NL5353904.091.15).
The use of oral spasmolytic drugs is usually not effective to obtain focal results in specific muscles (50) and carries the risk of systemic side-effects, such as nausea, drowsiness, loss of (leg) muscle strength, and dizziness. Yet, oral spasmolytic drugs (e.g. baclofen, tizanidine or tolperisone) should be considered when there is severe “lower body” spasticity affecting several distal and proximal leg muscles, hampering effective stepping responses. When effective, such patients will probably also profit from this medication with regard to their gait capacity. If oral spasmolytic drugs are insufficient (and multilevel intramuscular BTX-A injections not feasible or impractical), intrathecal baclofen therapy (ITB) should be considered for this relatively severe subgroup of patients. ITB has shown to reduce spasticity-related complaints and improve walking capacity in these patients (51), but its effect on balance capacity has not yet been shown.
As stated above, pes equino(varus) is the main, and often first, deformity seen in patients with HSP due to shortening of the dorsal leg muscles. In addition to muscle contracture, spasticity may contribute to this deformity when spastic muscles are no longer able to relax fully. From this perspective, focal spasmolysis of the calf muscles, tibialis posterior and/or long toe flexors may also be indicated to reduce ankle deformity, but such treatment should always be accompanied by intensive stretching exercises to improve muscle length and inhibit muscle tone. In particular, selective BTX-A injections in the tibialis posterior muscle may be effective to reduce varus deformity, unless fixed varus contracture has developed. In the case of a fixed contracture, ankle deformity can be compensated by providing orthopaedic footwear, but the effectiveness of such footwear to improve balance capacity in patients with HSP has not yet been studied. The main goal of orthopaedic footwear is to restore a full base of support in both the antero-posterior and medio-lateral directions and to provide ankle stability in the case of structural varus deformity. When there is concomitant pes cavus, a well adjusted insole can accommodate for this latter deformity. Orthopaedic footwear should always be as light-weight as possible and allow sufficient mobility at the talocrural (superior) ankle joint for optimal use of ankle strategies and for an optimal roll-off motion during gait. In addition, the external sole should not aggravate any tendency towards foot drag.
Another option for restoring a normal base of support is to surgically lengthen the shortened dorsal muscles of the lower leg, particularly for more severe contractures and for those patients who do not want to rely on adjusted footwear. Usually, percutaneous Achilles tendon (AT) lengthening is sufficient to correct pes equinus. Interestingly, it is our experience that AT lengthening will often reduce the degree of post-operative calf muscle spasticity as well. Tenotomy of the tibialis posterior muscle may be effective to correct pes varus, but an (complementary) arthrodesis of the talonavicular joint may be a more viable treatment option. In addition, tenotomy of the long toe flexors may be necessary for the AT lengthening to be truly effective. Osteotomy of the first metatarsal bone can be performed to correct a concomitant severe and structural pes cavus.
Any treatment that is able to reduce equinovarus deformity at the ankle joints will eventually be beneficial for static and dynamic balance by allowing better use of ankle strategies in both planes and by a reduced risk of tripping, hooking, ankle instability or ankle sprain. Correction of equinovarus deformity will also improve standing posture by requiring less postural adjustments at the knees, hips and trunk.
Knee flexion and hip adduction contractures must preferably be treated by an intensive stretching regime, supported by BTX-A injections in the hamstrings and hip adductor muscles, respectively. As for the hip adductors, the adductor magnus, adductor longus, and gracilis are the most relevant target muscles, given their anatomical lever with respect to the hip joint (52). In our experience, the medial hamstrings are a better target than the lateral hamstrings if there is a tendency towards internal rotation at the hips. In addition to passive stretching exercises, active stepping and agility training is recommended to incorporate improved joint range of motion into the motor programmes used for standing and walking.
As indicated above, muscle weakness does not seem to be the major determinant of balance impairments in HSP. This is probably related to reticulospinal compensation originating from the brainstem (22). Exercise training to improve muscle strength is therefore not very likely to improve balance capacity in most patients with HSP. However, patients with HSP are prone to “disuse” phenomena due to lack of activity and fear of falling. So if a patient’s history and/or clinical examination indicates disuse, a comprehensive physical training programme, guided by a physical therapist, is recommended. As prolonged walking frequently leads to increased leg muscle tone, this may not be the optimal training activity for patients with HSP. We therefore advise regularly performing cycling exercises, preferably under natural circumstances using a (adapted) bicycle, or a home trainer. Most patients experience a beneficial effect of cycling exercises, not only on their muscular and cardiopulmonary endurance, but also on their leg muscle spasticity and stiffness during walking. Usually, this kind of aerobic training can be done at home or in a community-based fitness practice and needs merely remote guidance from a physical therapist. The effectiveness of regular (cycling) exercises to prevent disuse phenomena, to improve muscular and cardiopulmonary endurance, and to reduce leg muscle spasticity in HSP is an important topic for future research.
Unfortunately, it is not possible to restore impaired proprioception in patients with HSP. Management should therefore focus on the use of optimal compensation strategies. Compensation involves an increased reliance on other sensory resources than proprioceptive information from the feet and lower legs (such as visual input or somatosensory information from the upper legs or provided by a walking aid). To train this type of compensation, we recommend patients with HSP to perform daily balance exercises at home, e.g. by alternately standing on one leg, in front of a high table or low cupboard, while gradually reducing the amount of hand/finger contact with the object. In our clinical practice, all patients are taught how to perform these exercises by an expert physical therapist during one treatment session.
When balance impairments are so severe that falls occur regularly, the use of walking aids cannot be avoided. Preferably, patients should use such aids not to lean on, but to obtain extra somatosensory information through the upper extremities. Thus, Nordic walking sticks are preferred above conventional canes or crutches. Some patients prefer to use a walker, as these devices often provide additional useful features, such as a seat and basket. Even when patients start to rely on walking aids, they must be challenged to maintain their balance capacity by continuing the daily performance of balance exercises to avoid the detrimental consequences of disuse. Eventually, some patients may need to rely on a wheelchair, even to cross short distances, depending on the age of onset and the progressiveness of the disease. We recommend consultation with an occupational therapist for advice on suitable wheelchairs.
Balance impairments are an important and “independent” functional consequence of HSP. Inadequate feet-in-place responses are predominantly due to progressively delayed balance responses and contractures of distal musculature. In addition, spasticity, contractures and, to a lesser extent, weakness of proximal leg muscles, result in suboptimal stepping responses. Falls are a threatening consequence of balance impairments and many clinicians perceive falls in HSP as untreatable. However, it is our experience that diligent history-taking and thorough clinical examination, followed by a multidisciplinary treatment tailored to the identified underlying mechanisms, is able to ameliorate balance capacities in patients with HSP and to prevent at least a proportion of these falls. Many treatment options that we have discussed need to be validated by further research. We conclude this review with some examples of topics for future studies. We have highlighted the need for studying the effect of focal spasmolysis by intramuscular BTX-A injections followed by stretching exercises in proximal musculature to improve stepping responses. With respect to contractures, future studies need to investigate the timing of soft-tissue surgery. We hypothesize that timely surgical treatment, for example of a pes equino(varus) deformity, will improve balance capacities and prevent falls in comparison with prolonged treatment with orthopaedic shoes.
With respect to functional balance training, the use of new technological tools should be investigated. One example is C-mill training, during which a diversity of visual targets is projected on a treadmill that need to be hit (or avoided) with various degrees of complexity, while safety is ensured by 2 parallel bars that patients can grasp in case of balance loss. The type and complexity of the visual targets can be individually adjusted, which makes it possible that every patient can train at his or her own level and can experience both benefit and reward. In our centre, we regularly provide 10 sessions of C-mill training (2 sessions per week, during 5 weeks) to patients with HSP for improving their dynamic balance. Such a training has been shown to be effective for patients with stroke (53) and for patients with hereditary forms of (spino)cerebellar ataxia (54), but studies in patients with HSP have yet to be performed. Another potentially useful type of functional exercise is robotic training using the Lokomat, a robotic gait orthosis combined with a harness-supported body weight system. In an uncontrolled study of 13 patients with pure HSP (55), a 6-week robot-aided gait training significantly improved balance performance assessed with the BBS. Future work is needed to investigate whether these promising results can be replicated by controlled studies.
With respect to the organization of multidisciplinary treatment for balance impairments in HSP, we expect that in the near future, patients will be supported by specifically designed e-health systems, monitoring their individual condition and connecting them to their primary healthcare providers. The feasibility and clinical value of such e-health systems also needs to be evaluated in future studies.
BvdW is supported by research grants from Radboud university medical centre, Hersenstichting, Bioblast Pharma, and ZonMW. ACHG received unrestricted grants from Ipsen and Merz to conduct efficacy studies of botulinum toxin.


 Click to show fullsize
Click to show fullsize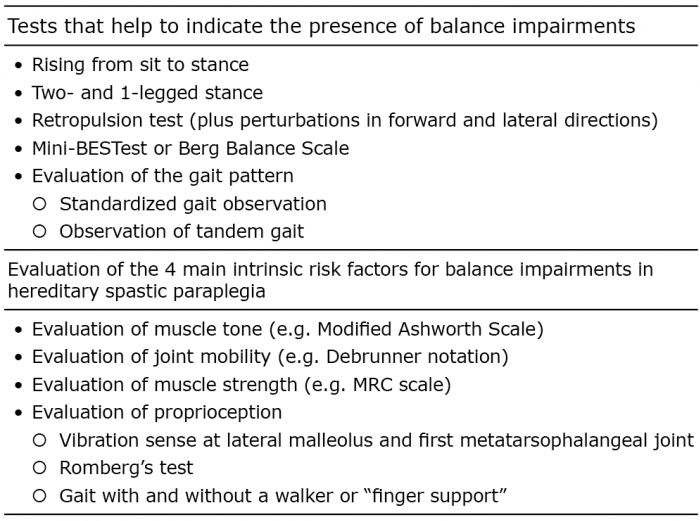 Click to show fullsize
Click to show fullsize