
From the Department of Rehabilitation Medicine, Hannover Medical School, Hanover, Germany
Objective: Strengthening of health-related rehabilitation services must start from the needs of persons with health conditions experiencing disability and should be implemented within health systems. The implementation of rehabilitation services in health systems should be planned and realized according to the World Health Organization’s 6 constituents of health systems (i.e. health service delivery; health workforce; health information systems; essential medicines; financing; and leadership and governance). The development of recommendations based on situation analysis and best-available data is crucial.
Methods: In order to facilitate such data collection at a national level, a checklist and a related questionnaire (Rehabilitation Service Assessment Tool (RSAT)) were developed and implemented. The following steps were followed to develop a checklist for implementation of rehabilitation services: a literature search, drafting, checking and testing the list, and development of the RSAT.
Results: The RSAT comprises 8 sections derived from 5 main domains of the most important areas of information (i.e. country profile; health system; disability and rehabilitation; national policies, laws, and responsibilities; and relevant non-governmental stakeholders).
Conclusion: The implementation of RSAT in different missions has shown that the principles are working well and that RSAT is feasible and helpful. Further field testing is important and the development of an internationally agreed tool should be promoted.
Key words: rehabilitation service assessment; health system building blocks; rehabilitation service implementation.
Accepted May 11, 2017; Epub ahead of print Jun 28, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Christoph Gutenbrunner, Department of Rehabilitation Medicine, Hannover Medical School, Carl-Neuberg-Str.1, 30625-Hannover, Germany. E-mail: Gutenbrunner.Christoph@mh-hannover.de
Responding to the Global Disability Action Plan 2014–2021 (GDAP) of the World Health Organization (WHO), “the implementation of measures that are designed to meet the rights of persons with disabilities” is a high priority for all member states of the United Nations. In order to develop national implementation plans, methods and tools are needed for the analysis of rehabilitation needs and existing policies, services and workforce.
This paper describes the development of a draft Rehabilitation Service Assessment Tool (RSAT) and provides a draft proposal for such a checklist/questionnaire. The aim is to provide a feasible tool for collection of information relevant to the development of National Disability, Health and Rehabilitation Plans (NDHRP) for supporting countries to develop policies on disability and rehabilitation, and to implement rehabilitation services including training of a highly qualified rehabilitation workforce (1).
According to the WHO the following 6 components are essential in order to build health systems and/or implement health services (2):
1. health service delivery;
2. health workforce;
3. health information systems;
4. access to essential medicines;
5. financing;
6. leadership and governance.
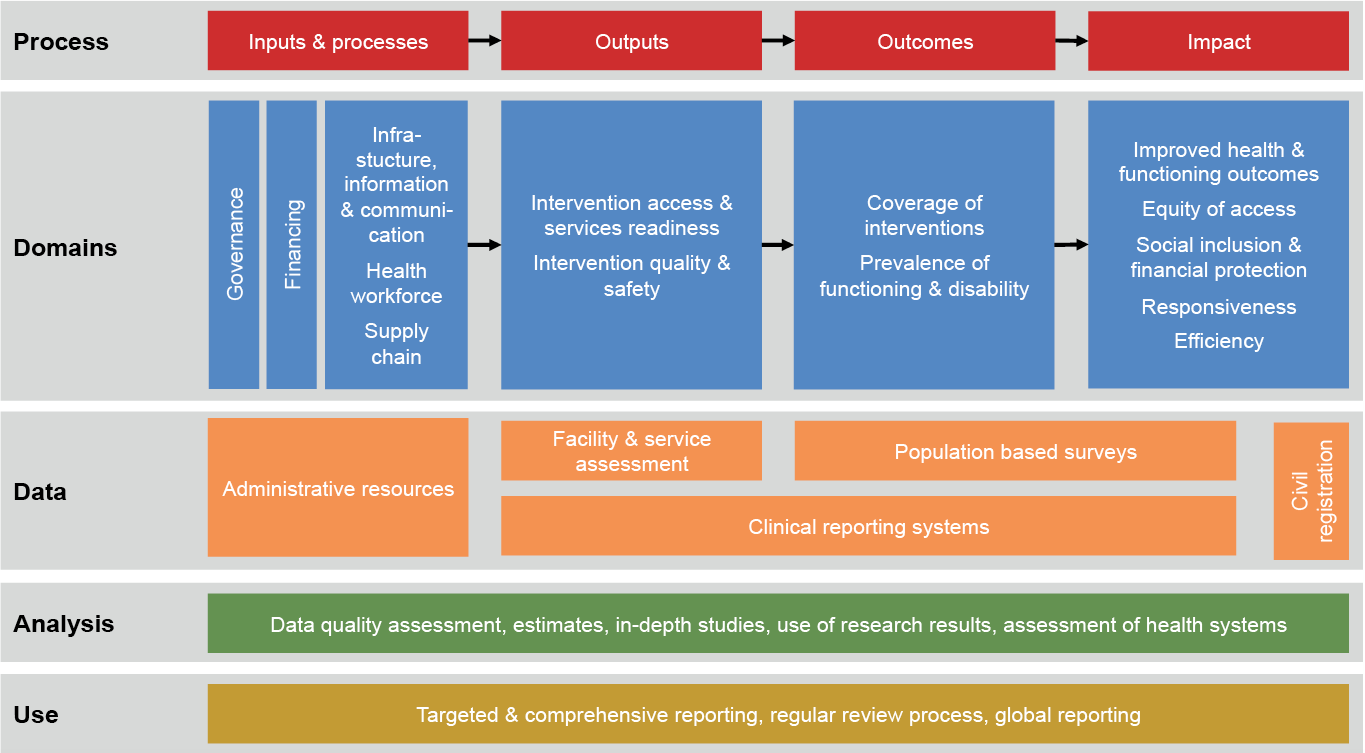
For monitoring and implementation of health services, the WHO suggests the sequence shown in Fig. 1. This is also relevant for implementing (new or additional) rehabilitation services in health systems and for monitoring and evaluation of such services. Thus, the assessment of rehabilitation services should include the following domains:
1. Governance and financing as an essential precondition of rehabilitation service delivery.
2. Infrastructure technologies, workforce, supply chain and information as essential parts of rehabilitation service organization (domains 1 and 2 represent inputs and processes).
3. Rehabilitation interventions including access, readiness, quality and safety (outputs).
4. Coverage of rehabilitation interventions (including assistive devices) and prevalence or level of impairment (outcome).
5. Improved health and functioning as well as equity, social and financial risks (impact). This also will improve responsiveness to the need of persons experiencing disability and efficiency of service delivery.
To evaluate domains 1 and 2 administrative sources must be assessed. Information on domain 3 comes from facility assessments. Domains 4 and 5 are in in the outcomes and impact, respectively. These can be done by population-based surveys which can provide information, including prevalence of disability, life situation, participation and inclusion of persons with disabilities and social status (see Fig. 1). As shown in Fig.1, all aspects must be covered by data quality assessment, estimates and projections, in-depth studies, use of research results, assessment of progress and performance and efficiency of health systems, and should be used for targeted and comprehensive reporting, regular review processes and global reporting. This matches the development of National Disability, Health and Rehabilitation Plans (NDHRP) (1) and their implementation monitoring and evaluation.
Fig. 1. Principles of monitoring and evaluation of health systems strengthening (from WHO 2009-modified; (3)).
According to the GDAP, health system constituents, in combination with rehabilitation principles, are crucial for the process of rehabilitation service implementation (4). Thus, these principles have been used to develop a RSAT for use in missions developing NDHRP.
In order to develop a checklist for important information for rehabilitation service implementation the following steps were undertaken by the authors in iterative discussion with teams in the missions (5–7):
Drafting the preliminary RSAT using principles as defined in the World Report on Disability (8), the WHO GDAP (4), the health system building blocks (3), the International Classification of Health Accounts (9), available definitions and descriptions of rehabilitation services (8, 10, 11), and based on the experiences gained during the technical consultancy to develop a National Disability and Health Plan for Egypt (6);
Testing the draft preliminary RSAT by using it for the development of a NDHRP for Ukraine (5) and modifying it on the basis of the model testing; and finally,
Developing a RSAT, which has been tested in a mission for the Democratic People’s Republic of Korea (7).
With regard to rehabilitation service implementation the 6 health system building blocks (12) can be modified as follows:
A. Rehabilitation service delivery (e.g. rehabilitation units in hospitals, rehabilitation centres, community-based rehabilitation services, assistive devices, integrated and multi-professional service delivery).
B. Rehabilitation workforce (e.g. physical and rehabilitation medicine, physiotherapy, occupational therapy, speech and language therapy, prosthetics and orthotics, rehabilitation engineer, psychotherapy, social work).
C. Information systems on rehabilitation services (including implementation of knowledge of rehabilitation service into curricula of all health professionals, information to healthcare providers, information to the public).
D. Access to essential treatments and rehabilitation interventions (provision of and access to rehabilitation treatments and interventions, such as medication, physiotherapy and other physical treatments, occupational therapy, psychotherapy, assistive devices and others).
E. Financing (integration of rehabilitation services in health service financing, e.g. national health system, health insurance, and coverage of cost as other elements of universal health coverage).
F. Leadership and governance in disability and rehabilitation issues (understanding and definition of disability at national level, laws on disability and rehabilitation, responsibilities on rehabilitation in Ministry of Health, communication and coordination between Ministries).
Based on these principles, the the amount of information required has been determined.
As described above, the checklist was developed for assessing existing rehabilitation services in health systems. The checklist includes the following 5 main domains:
A. Country profile information
B. Information about the health system.
C. Information about disability and rehabilitation
D. Information about national policies, laws, and responsibilities in the area of disability and rehabilitation
E. Information about relevant non-governmental stakeholders
These domains should include the following categories of information outlined below.
A. Country profile information. This domain has 3 subdomains:
a. Country profile/characteristics: number of population, socio-economic factors, and infrastructure are relevant factors in order to learn about the situation of the country. In addition to the number of population size and gross domestic product (GDP), information will be collected about the proportion of GDP spending on health and the situation regarding the country’s infrastructure.
b. Cultural background: it is already known that language, ethnicity, belief/religion, and social attitudes are relevant factors related to cultural competencies. These factors are relevant to reduce disparities in health service delivery (13, 14).
c. Epidemiology: epidemiological data are necessary to gain an overview of the situation related to the health condition of the country, including risk factors, prevalence and incidence of diseases and causes of death. More specifically, prevalence of disability caused by health conditions, trauma and injury are also important.
i. Risk factors, prevalence and incidence of diseases, causes of deaths;
ii. prevalence and incidence of disability caused by health conditions (including mental disease and congenital disorders);
iii. incidence of disability caused by trauma and injury (number of traffic accidents, work accidents, private accidents, and victims of violence and type of injury);
iv. information on the need for rehabilitation (including assistive devices) and number (percentage) of persons in need receiving rehabilitation services.
B. Information about the health system. All of the 6 health system building blocks need to harmonize effectively and efficiently in order to attain the overall goal of improved health, responsiveness, social and financial risk protection, and outcome. The following information is needed as a basis for analysis of the country’s health system:
a. Health service delivery: good health service delivery is the highest priority of the 6 health system building blocks. Good health service delivery can be denoted as a service that can deliver effective, safe, good-quality personal and non-personal care to those who need it, with minimum waste (2). Information that should be collected includes general organization of health services, both state and private sector, as well as access to services.
b. Health workforce: spectrum of the number of health professionals covering the country in proportion to the population, and how these health professionals are distributed within the country.
c. Health information: information on the prevalence and incidence of disability that is relevant for planning rehabilitation services; responsibility and quality of data collection and publication parameters of data collection.
d. Medicine, vaccine and technology: information regarding assistive devices for people with disabilities (policy, standard) is relevant.
e. Health system financing: general information regarding financing issues (state funding, insurance, out of pocket (paid for with your own money).
f. Leadership and governance: including information about the structure of the health system
C. Information about Disability and rehabilitation.
a. Definitions and terminology used to describe “disability” (e.g. WHO definition, number of persons applying for disability compensation). It is important to gather information regarding the definition and description of disability and its related terminology.
b. Disability category: information regarding how the country’s health system classifies the type and severity of disability is important.
c. Need for rehabilitation (including assistive devices) and number (percentage) of persons in need receiving rehabilitation services.
d. Rehabilitation services organization and issues regarding provision of assistive technology. Information about rehabilitation-related professionals falls under the domain of rehabilitation workforce.
i. Number of rehabilitation services (at primary, secondary, and tertiary level, and along the continuum of care);
ii. structure of existing rehabilitation services (technical equipment, team structure, etc.);
iii. provision of assistive devices including prostheses (availability, costs, individual adaptation and training, technical maintenance);
iv. role of peers and families in caring of persons with disabilities (including children and people with old age);
v. links of health-related rehabilitation with vocational rehabilitation, education and other important life areas.
e. Rehabilitation workforce
i. Name, definition, education (including institution), training, accreditation;
ii. number and distribution of rehabilitation professionals (per profession, local distribution and places of work).
f. Research and data collection: research institutes and projects on disability and rehabilitation: disability surveys (including method of data collection and results), rehabilitation outcomes, development of national guidelines, etc.
D. Information about national policies, laws, and responsibilities in the area of disability and rehabilitation
a. Laws and regulations on disabilities and rehabilitation
i. Signature and ratification of the United Nations Convention on the Rights of Persons with Disabilities (UN-CRPD).
ii. Comprehensive law on disability, functioning and health law (or fragmented paragraphs in other laws).
iii. Relevant regulations (e.g. right to rehabilitation, disability assessment and compensation).
b. Government policies and responsibilities
i. Policies and responsibilities of Ministry of Health and Ministry of Social Affairs.
ii. Policies and responsibilities of other ministries (e.g. infrastructure, education, labour, justice).
iii. Policies and responsibilities within ministries (e.g. department for disability and rehabilitation or fragmented responsibilities).
iv. Policies and responsibilities communication and coordination among ministries.
c. Policies and responsibilities of insurances system, non-governmental organizations (NGOs), private sectors and others (other stakeholders).
E. Information about relevant non-governmental stakeholders.
a. Number, types and role of organizations of persons with disabilities.
b. National and international humanitarian organizations and their role in health and social system.
c. Professional organizations and their position.
In order to facilitate the collection of information needed prior to country visits for the development of NDHRPs (see (1)) the above-mentioned dimensions were transformed into a draft questionnaire (preliminary RSAT). It was designed with the WHO Ear and Hearing Care Situation Analysis Tool (15) as a blueprint. After testing it with the missions in Ukraine(5) and the Democratic People’s Republic of Korea (7) a revised list of information was extracted and RSAT, below, was developed.
The RSAT comprises 8 sections.
In addition, the questionnaire contains initial information on the assessment method and appendices with definitions and explanations, and guidance on how to use the tool.
During the 3 testing phases the information list and questionnaire were improved continuously. This, in particular, involved the inclusion of a more detailed list of disabling health conditions, a description of prototype rehabilitation services, and enhanced lists of rehabilitation professionals and assistive devices. After the third testing phase the authors considered that it could be used for field testing in other contexts and by other working groups.
In detail, the beta version of the questionnaire contains the items outlined below.
Section 1: General country information, public health indicators and health system information
1.1. General country information
1.1.1. Total population
1.1.2. Age distribution
1.1.3. Sex distribution
1.1.4. Rural–urban distribution
1.1.5. Education
1.1.6. Economy
1.1.7. Transportation infrastructure
1.1.8. Relevant cultural factors
1.1.9. Other relevant country information
1.2. Public health indicators
1.2.1. General health indicators
1.2.2. Main causes of death
1.2.3. Prevalence of diseases and injury
1.2.4. Risk factors
1.2.5. Other relevant epidemiological information
1.3. Health system information
1.3.1. Healthcare provision
1.3.2. (main) funding of health services
1.3.3. Health insurance (or other funding system)
1.3.4. Hospitals (in-patient services)
1.3.5. Out-patient services
1.3.6. Health workforce
1.3.7. Other relevant health system information
Section 2: Information on assessment and epidemiology of disability
2.1. Disability data
2.1.1. How is disability defined in laws and regulations?
2.1.2. Is the WHO International Classification of Functioning, Disability and Health (ICF) used as a framework for disability and rehabilitation policies?
2.1.3. Are there national surveys on the prevalence of disability?
2.1.4. Is there a plan for national surveys on the prevalence of disability?
2.1.5. Other relevant disability data
2.2. Epidemiology of disability
2.2.1. Overall estimation of disability
2.2.2. What is the prevalence of the most relevant disabling health conditions?
2.2.3. Most frequent impairments, activity limitations and participation restrictions
2.2.4. Do research institutions examine disability data collection? And how projects are funded
2.2.5. Other relevant disability data
Section 3: Information on disability policies and governmental and non-governmental stakeholders
3.1. Disability policy
3.1.1. Did the country sign the UN-CRPD?
3.1.2. Did the country ratify the UN-CRPD?
3.1.3. Does the country have a law on disability and rehabilitation?
3.1.4. Are there other binding rules on disability and rehabilitation?
3.1.5. Is there a classification and/or categorization of disability?
3.1.6. Is there a national disability, health and rehabilitation plan?
3.1.7. Other relevant information about disability policies
3.2. Responsibilities in the government
3.2.1. Which ministries have responsibilities in disability and rehabilitation?
3.2.2. At what level is disability and rehabilitation localized in the ministry?
3.2.3. How are activities coordinated between ministries?
3.2.4. What other governmental or legal organizations have responsibilities in disability and rehabilitation?
3.2.5. Other relevant information about responsibilities of the government
3.3. Non-governmental stakeholders
3.3.1. What are the relevant non-governmental stakeholders in rehabilitation and what are their respective tasks or areas of activity?
3.3.2. Other relevant information on NGOs
Section 4: Information about (health-related) rehabilitation service capacity
4.1. Health-related rehabilitation services
4.1.1. In-patient rehabilitation services
4.1.2. Access to rehabilitation services
4.1.3. Quality of care
4.1.4. Other information about rehabilitation services
4.2. Funding of services
4.2.1. Rehabilitation services payment
4.2.2. Payment (or cost-refund) for assistive devices
4.2.3. Payment (or cost-refund) for medicines relevant for rehabilitation (e.g. spasticity, pain)
4.2.4. Do research institutions examine rehabilitation systems and rehabilitation outcomes and how projects are funded?
4.2.5. Other relevant information about healthcare funding
4.3. Rehabilitation workforce
4.3.1. Physicians
4.3.2. Therapists
4.3.3. Other health and social professions
4.3.4. Other professionals relevant to health-related rehabilitation
4.4. Technical equipment
4.4.1. Diagnostic tools
4.4.2. Technology for intervention
4.4.3. Other devices
4.5. Assistive devices
Section 5: Additional relevant information
Section 6: Evaluation of information
6.1. Preparedness of country for development and implementation of disability and rehabilitation care strategies
6.2. Existence and implementation of country on disability and rehabilitation care strategies
6.3. Situation of service provision regarding disability and rehabilitation care strategies
6.4. Situation of human resources regarding availability of rehabilitation services
6.5. Situation regarding availability of educational facilities for training of human resources for disability and rehabilitation within the country
6.6. Situation regarding availability and accessibility of assistive devices in the country
6.7. Situation regarding health information systems in the country
6.8. Situation regarding the overall situation of health financing for rehabilitation services (not including assistive devices)
6.9. Situation regarding the overall situation of health financing for assistive devices
Section 7: List of sources
Section 8: Summary of information, recommendations and proposed projects
The questionnaire includes tick boxes for pre-formed answers and blank space for descriptive answers.
The WHO’s GDAP sets out clear guidance for strengthening rehabilitation services at national levels (4). This includes implementation of rehabilitation services, provision of assistive devices, development of the rehabilitation workforce, and others (1). The evidence-based Rehabilitation Guideline on service provision and financing (16) recommends that rehabilitation services should be implemented in health systems and be paid for by for health insurance, the public health system or other payment system, assuring equity of access. Both the GDAP and the Rehabilitation Guideline provide guidance on how to implement rehabilitation services that meet the highest possible level of quality and availability for persons in need. Thus, many countries that are willing to improve their national rehabilitation services seek guidance and advice. The WHO provides such advice to national governments on request, in collaboration with NGOs in official relation with the WHO Disability and Rehabilitation Team (1). These missions must be based on sound information about relevant factors, as well as a systematic approach in order to identify gaps and to recommend activities regarding how to close the gaps (1).
In performing such missions, the problem occurs as to how to collect all relevant data on a sound basis. This, on the one hand, must be done on the basis searching available sources of information (reports, statistics, publications and others). More detailed information can be collected through country visits and stakeholder interviews. However, it is important to check systematically whether all relevant information is available and what remains to be investigated. Secondly, it is helpful if the information is available prior to the country visit.
As no such checklists have been available, the authors designed a preliminary checklist of relevant information based on the 6 health system building blocks (12). This preliminary RSAT checklist was tested in 2 rehabilitation service implementation advisory missions (5, 6) and was shown to be feasible and helpful for the development of NDHRPs. However, in using the checklist, some points that would improve the quality of the list were identified.
As a second step, a questionnaire was developed, using the Ear and Hearing Care Situation Analysis Tool (15) as a blueprint. This questionnaire (RSAT) should enable the collection of information from governments or experts from the county of the national WHO offices. It was tested in a mission (in the Democratic People’s Republic of Korea (7)) and was shown to be useful. Further testing and evaluation of outcomes is needed.
This paper used a pragmatic approach to developing checklists and questionnaires for collecting all relevant information to develop NDHRPs. Testing of these instruments in different missions has shown that the principles work well, and that the tools are feasible and helpful. However, further testing is important and the development of an internationally agreed tool should be promoted. It is hoped that the work presented here will be useful as the basis for future developments.


 Click to show fullsize
Click to show fullsize