
From the 1Health Sciences, Faculty of Sport and Health Sciences, University of Jyvaskyla, 2Department of Physical Medicine, Central Finland Health Care District, Jyväskylä, Finland, 3Department of Rehabilitation Medicine and Department of Psychiatry, VU University Medical Center, Amsterdam, The Netherlands, 4Department of Orthopaedics and Trauma, Tampere University Hospital, Tampere, 5Department of Orthopaedic Medicine, Central Finland Health Care District, Jyväskylä and 6MedCare Foundation, Äänekoski, Finland
Objective: To study the effectiveness of a 12-month exercise therapy on kinesiophobia and physical activity in patients with spondylolisthesis after lumbar spine fusion.
Design: Randomized controlled trial.
Subjects: Patients (n = 98) with spondylolisthesis who had undergone lumbar spine fusion.
Methods: All patients (mean age 59 years) had received lumbar spine fusion surgery and identical postoperative instructions. Three months postoperatively, they were randomized into an exercise group (n = 48) or usual care group (n = 50). The exercise group received 12-month progressive home-based training with regular booster sessions, and the usual care group a single session of physiotherapy instruction. Kinesiophobia was assessed with the Tampa Scale for Kinesiophobia (TSK) and physical activity by the International Physical Activity Questionnaire (IPAQ) preoperatively, 3 months after lumbar spine fusion, and at the end of the 12-month intervention.
Results: Before the intervention, the median (first quartile; third quartile) of TSK was 32.5 (29.0; 37.0) in the exercise group and 30.0 (25.8; 36.0) in the usual care group, changing to 30.0 (25; 36) in the exercise group and to 30.5 (24; 36.3) in the usual care group (between-group p = 0.17). IPAQ metabolic equivalent minutes per week increased from 1,863 (1,040; 3,042) to 3,190 (1,634; 6,485) in the exercise group and from 2,569 (1,501; 4,075) to 3,590 (1,634; 6,484) in the usual care group (between-group p = 0.92).
Conclusion: Progressive 12-month home-exercise starting 3 months postoperatively was not superior to usual care in decreasing kinesiophobia or increasing physical activity in spondylolisthesis.
Key words: spondylolisthesis; spinal fusion; physical therapy modalities; exercise therapy; low back pain.
Accepted July 10, 2017; Epub ahead of print Sep 1, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Outi Ilves, University of Jyvaskyla, Faculty of Sport and Health Sciences, PO Box 35, Viveca Building, Viv281, FI-40014, Finland. E-mail: outi.e.ilves@jyu.fi
Fear of movement or re-injury, also known as kinesiophobia, is a common problem among patients with musculoskeletal pain (1). It may result in avoidance behaviour and inactivity, leading eventually to disability (2–5). Kinesiophobia also has a central role in the development of chronicity in low back pain (3, 5). Lumbar spine fusion (LSF) surgery may be a treatment option for chronic low back pain caused by spondylolisthesis if conservative treatment fails (6, 7). Physical activity and early return to normal daily activities after LSF surgery is considered important for several reasons. Patients concern over whether the fusion has healed may lead to inactivity and fear-avoidance behaviour. Physical activity enhances recovery from a prolonged period of back pain (8) as well as from surgery. Physical activity may also lower the risks of other health problems caused by inactivity (9, 10). Kinesiophobia can be considered a barrier to physical activity, as well as a condition that restricts social life following LSF surgery.
To the best of our knowledge, only 2 RCT studies have evaluated kinesiophobia in postoperative rehabilitation after LSF surgery (11, 12). In the study by Abbott et al. (11), psychomotor therapy with exercises was more effective than exercises alone in decreasing fear of movement. Monticone et al. (12) reported that combined exercise and cognitive-behavioural therapy was superior to an exercise programme alone in reducing disability, kinesiophobia-related dysfunctional thoughts and pain, and enhancing quality of life. Both short-term interventions were implemented during the first 3 postoperative months. Archer et al. (13) suggest that, in laminectomy patients (with or without arthrodesis) with high kinesiophobia, targeted cognitive-behavioural-based physical therapy 6 months postoperatively may improve pain, disability and general health more than an educational programme. No studies have evaluated the effects of lumbar spine fusion on kinesiophobia and physical activity, or the effectiveness of later postoperative exercise therapy compared with usual care on kinesiophobia and physical activity.
This study evaluated the effects of a 12-month postoperative back-specific exercise programme combined with aerobic training on fear of movement and physical activity compared with usual care in patients with isthmic or degenerative spondylolisthesis. The effect of surgery before the intervention is also reported.
This parallel group randomized controlled trial (RCT) (registration no: NCT00834015) was conducted at 2 Finnish hospitals: Tampere University Hospital and Central Finland Central Hospital. A sample size calculation was performed for the main outcome measure of the trial (pain, visual analogue scale) (14) and is explained in the RCT study protocol article by Tarnanen et al. (15). All patients scheduled for non-urgent LSF surgery for isthmic or degenerative spondylolisthesis, who were over 18 years of age were eligible for the study. Exclusion criteria were: severe cardiorespiratory or musculoskeletal disease, fracture, tumour, severe psychiatric disorder, extensive lower limb paresis, alcohol abuse and immediate complications after surgery that could prevent the patient from participating in the postoperative rehabilitation programme.
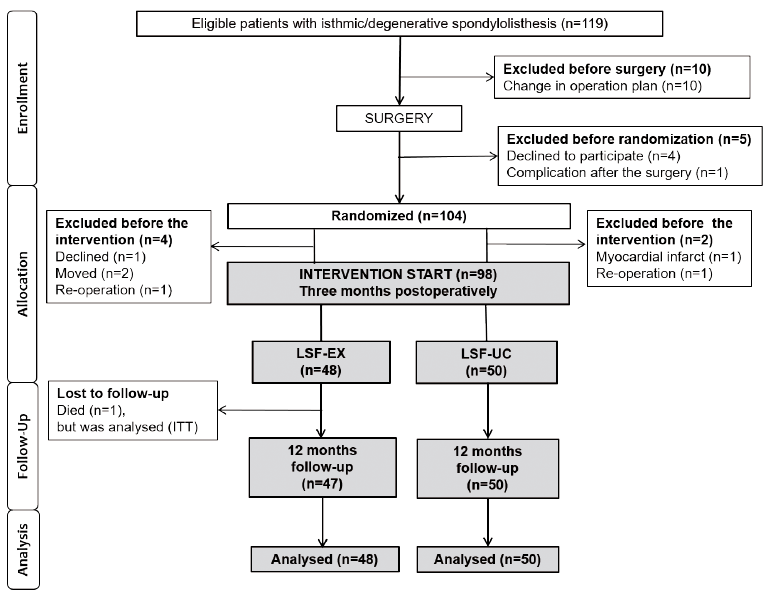
In total, 104 consecutive patients underwent LSF. Six patients were excluded before the start of the intervention, and thus the final number of participants was 98, of whom 48 were allocated to the exercise group (LSF-EX) and 50 to the usual care group (LSF-UC) (Fig. 1). The study was approved by the ethics committees of both study centres (recorded as decision 4E/2008 at Central Finland Central Hospital, and subsequently also confirmed by Tampere University Hospital).
Fig. 1. CONSORT (Consolidated Standards of Reporting Trials) patient flow diagram. LSF: lumber spine fusion; EX: exercise group; UC: usual care group.
Allocation to LSF-EX or LSF-UC was performed randomly using computer-generated 4-block randomization lists compiled by a biostatistician. Two lists were created: (i) isthmic and (ii) degenerative spondylolisthesis. Concealed randomization was used, and was conducted by nurses who were not otherwise involved in the study. The study questionnaires were collected and saved by research assistants who were blinded to treatment. However, owing to the nature of the study, the physiotherapists could not be blinded. To avoid confusion between the LSF-EX and LSF-UC treatments, each study arm in each hospital had its own physiotherapist. Participant preoperative recruitment started in September 2009 and ended in September 2010, when a sufficient sample size had been achieved. The last recruited participants completed the 12-month intervention in January 2012.
Surgical indications and techniques and the pre-and post-operative rehabilitation protocols were matched in the 2 hospitals before the study. Some of the operations were collaboratively performed by surgeons from both hospitals to ensure that the surgical techniques used were similar. All patients had postero-lateral instrumented fusion and 21% also had posterior interbody fusion. The frequencies of the techniques used were similar in both study groups: 20% in LSF-EX and 22% in LSF-UC had posterior interbody fusion, (χ2 test between groups p = 0.89). All patients were provided with similar postoperative instructions for up to the first 3 postoperative months. During the first few days after LSF, patients were encouraged to start light walking training and leg muscle stretching, as well as light trunk muscle contraction exercises to re-learn good posture of the upper body. They were also instructed to avoid continuous sitting for more than 30 min at a time during the first 4 weeks, after which the use of a cycling ergometer was encouraged. Six weeks after surgery, a physiotherapist at the outpatient clinic instructed all patients to gradually increase the amount of walking training time, to perform light abdominal, back and thigh muscle exercises, and to stretch their hip muscles. All patients were instructed to avoid extreme flexion and extension of the spine for the first 2 postoperative months, after which more strenuous physical activities were allowed.
The LSF-EX programme consisted of 12 months of progressive home-based back-specific and aerobic training together with fear avoidance counselling by a physiotherapist, starting 3 months postoperatively, i.e. at a time when the LSF healing process had advanced and it was safe to start progressive training. A physiotherapist gave each patient individual instructions on the exercises in accordance with the exercise protocol (15). The patients exercised independently at home, and had booster sessions with the physiotherapist every second month (6 meetings in total).
The main aims of the 12-month back-specific exercise programme were to improve lumbar spine control and to increase trunk and hip muscle coordination, strength and endurance. Exercises were selected partially on the basis of electromyographic studies in healthy subjects and LSF patients (16–22). The muscle groups trained were the abdominal, gluteal, thigh, and low back muscles. The hospital supplied the patients with 2–3 elastic bands of differing stiffness (Thera-Band®, The Hygienic Corporation, Akron, Ohio, USA) for use in some of the exercises. The programme was progressive, starting with exercises performed in the unloading position (supine, prone or 4-point kneeling). As the programme advanced, the strengthening exercises became more challenging in both the coordination and muscle strength required. The degree of difficulty was increased by increasing the functionality of the exercises and the resistance of the elastic band. Progression was also implemented by increasing the number of repetitions and sets from 2 × 10–20 to 2–4 × 10–20, depending on the exercise and the participant’s fitness level. The precise training resistance was re-evaluated at check-up visits by repetition maximum tests, and the stiffness of the elastic bands set to provide a training resistance of 50–70% of estimated maximum strength using the 10-repetition maximum method. The participants were instructed to perform the exercises at least 2–3 times a week.
The participants in the LSF-EX group were also instructed to increase the total number of daily steps during the intervention by walking training, performance of which was encouraged at least 3 times per week. To ensure that the walking was vigorous enough to obtain health benefits, the patients, after warming up, were instructed to perform walking sessions consisting of 30 s to 1 min of brisk walking, alternating with 3 min of walking at normal speed. At the beginning of the intervention, the duration of 1 walking session was approximately 25–30 min. Progression was increased based on a dose-response relationship (intensity/time). The number of steps per day and frequency of exercise sessions per week were noted in exercise diaries.
During the booster sessions in physiotherapy, barriers to physical activity, such as kinesiophobia or pain, were identified and discussed with the patient. The physiotherapist sought to allay harmful, irrational beliefs and fears regarding activity, and provided additional telephone support when needed. The physiotherapist also reviewed the patient’s experiences regarding the previous phase of the exercise programme, instructed the patient in the next phase of the programme, and defined the new target number of daily steps (walking training). The patients received pictorial and written instructions for the exercises.
The patients in the LSF-UC group received just one guidance session with a physiotherapist 3 months after surgery. The session consisted of instructions for the standard home exercises. The home exercise programme included light muscle endurance exercises (abdominal muscles, back muscles and hip muscles), stretching and balance training (1-leg standing). The patients were advised to perform the home exercises 3 times per week. Pictorial and written instructions for the exercises were issued.
Kinesiophobia was assessed with the Tampa Scale for Kinesiophobia questionnaire (TSK) (23–25). The TSK comprises 17 items rated on a 4-point Likert response scale (1 totally disagree to 4 totally agree), with total scores ranging from 17 (minimum – no fear) to 68 (maximum – intense fear) points. The TSK items are shown in Appendix I. Physical activity was measured with the short form of the International Physical Activity Questionnaire (IPAQ) (26). Physical activity is expressed as a continuous score of total metabolic equivalent minutes per week (METmins/week). According to the IPAQ Scoring Protocol, less than 600 METmins/week is considered inactive, 600–2,999 is considered moderate activity and 3,000 or more is considered highly active, and meeting the criteria for health enhancing physical activity (26, 27).
Appendix 1. Description of the Items of the Tampa Scale for Kinesiophobia (23)
In addition, age, weight, height, smoking status, education, employment, and duration of symptoms were gathered by questionnaire. The intensity of low back and leg pain during the previous week was measured using a 100-mm visual analogue scale (VAS) (28). During the intervention, the LSF-EX group recorded their back-specific exercises and number of steps per day measured by a pedometer (Omron HJ-113-E, Omron Health Care, UK) in their exercise diary.
Data were analysed according to the intention-to-treat principle. The results are expressed as mean (standard deviation: SD), with 95% confidence intervals (95% CI) or median (lower and upper quartiles: Q1; Q3), counts with percentages, or frequency distributions. The normality of the variables was tested by the Shapiro-Wilk W-test. Comparisons between the groups in preoperative descriptive data were made by independent samples t-test or bootstrapped type t-test for continuous variables and χ2 test were used for categorical variables. The intervention outcomes were analysed using the non-parametric independent samples Mann-Whitney U test for between-groups differences. The significance of change over time was assessed using the non-parametric-related samples Wilcoxon signed-rank test. Effect size (ES) was calculated by Cohen’s d (mean baseline scores minus mean follow-up scores, divided by the pooled standard deviation). An effect size ≥ 0.20 was considered small, ≥ 0.50 medium, and ≥ 0.80 large (29). The 95% confidence intervals (95% CI) of ES for the effect sizes were obtained by bias-corrected bootstrapping (5,000 replications). Pearson’s rho was used as a correlation coefficient. Statistical analysis was performed using IBM SPSS Statistics 20 software (IBM Corporation Armonk, NY, USA) and STATA 11.1 (StataCorp LP, College Station, TX, USA) software.
Mean patient age was 59 (range 32–84) years, and 74% were women. Almost half of the participants were retired, and one-third were employed. The diagnosis for surgery was degenerative spondylolisthesis in 69% and isthmic spondylolisthesis in 31% of cases. Mean (standard deviation; SD) preoperative duration of low back symptoms was 3.5 (3.4) years. Mean intensity was 60 (22) mm for low back pain and 61 (25) mm for radicular leg pain across the whole sample. No preoperative differences between the groups were found in socio-demographic or clinical data (Table I).
Table I. Preoperative clinical and socio-demographic data
Table II shows the main results of TSK, IPAQ and pain intensity in medians with first and third quartiles (Q1; Q3). During the exercise intervention, the mean change in the total TSK score in the LSF-EX group was –1.6 points (ES 0.23, 95% CI –0.05 to 0.51) and in the LSF-UC group 0.2 (ES –0.03 95% CI –0.28 to 0.21). The difference between the groups was not significant (p = 0.17) (Fig. 2b). When the items were analysed separately, a significant difference between the groups was found for TSK item 9 (“I am afraid that I might injure myself accidentally”) (p = 0.01).
Table II. Changes in kinesiophobia, physical activity and pain intensity during the 12-month exercise intervention
Fig. 2. Mean scores with 95% confidence intervals on the Tampa Scale for Kinesiophobia (TSK) before surgery and 3 months after surgery in (a) all patients and (b) by groups before and after the 12-month intervention. LSF: lumbar spine fusion; EX: exercise group; UC: usual care group.
The mean within-group change was significant in the LSF-EX group for items 1 (“I’m afraid that that I might injure myself if I exercise”) (p = 0.01) and 9 (p = 0.006) (Fig. 3). In the LSF-EX group, a high TSK score at the beginning of the intervention was associated with a larger decrease during the intervention (r = –0.29, p = 0.05). In the LSF-EX group, the median (Q1; Q3) IPAQ score was 1863 (1040; 3042) METmins/week before the intervention and 3190 (1,150; 6,384) METmins/week (p = 0.01) at intervention end. The corresponding scores in the LSF-UC group were 2,569 (1,501; 4,075) and 3,590 (1,634; 6,485) METmins/week (p = 0.01). The difference between the groups was not significant (Table II). No changes in low back or leg pain were observed within the groups during the 12-month intervention.
Fig. 3. Item-specific mean changes with 95% confidence intervals in the Tampa Scale for Kinesiophobia (TSK) during the 12-month postoperative intervention by groups. LSF: lumbar spine fusion; EX: exercise group; UC: usual care group.
Compliance was assessed by exercise diaries. The median (Q1; Q3) frequency of the back-specific exercise was 2.5 (1.9; 3.4) times per week during the first 2 months of the postoperative intervention in the LSF-EX group. During the last 2 months of the intervention, the frequency was 1.4 (0.6; 1.9) times per week (within-group change p < 0.001). The median (Q1; Q3) numbers of daily steps at the same time points were 6,138 (3,759; 8,907) and 5,870 (3,587; 8,024) (within-group change p = 0.24). No participant reported discontinuance due to harms caused by the exercise programme. Seven patients in LSF-EX discontinued the exercise intervention. Four patients discontinued due to difficulties in commuting to booster meetings. One patient presented with a sudden decline in haemoglobin and general condition and was referred for further examination. A physician advised 1 patient to discontinue exercising, owing to a problem with fixation (patient subsequently had a re-operation and was diagnosed with myopathy, leading to muscle weakness) and one died (myocardial infarction). The intention-to-treat method was used and all patients (n = 98) were thus included in the analysis in their original assigned groups.
The preoperative median (Q1; Q3) total TSK score was 39 (33; 44) points. At 3 months after surgery, it had decreased to 31 (26; 36) points (p < 0.001) across the whole sample (Fig. 2a). The effect size of the change in the TSK total score was 1.02 (95% CI 0.82–1.26). Three months after surgery, a significant improvement was observed in 11 of the 17 items. The largest changes were observed in items 3 (“My body is telling me I have something dangerously wrong”) and 11 (“I wouldn’t have this much pain if there weren’t something potentially dangerous going on in my body”). A higher pre-operative TSK score was associated with a larger decrease in the same score 3 months postoperatively (r = –0.62, p < 0.001). The preoperative median (Q1; Q3) IPAQ was 1,709 (1,396; 3,982) METmins/week, and at 3 months postoperatively it was 2079 (1,386; 3,792) METmins/week across the whole sample (p = 0.15). Three months after surgery, median (Q1; Q3) low back pain intensity had decreased from 61 (47; 76) to 14 (3; 30) mm, and leg pain intensity from 64 (43; 80) to 9 (2; 29) mm across the whole sample (p < 0.001). The association between the change in low back pain and the change in TSK score was r = 0.37 (p < 0.01).
The results of the study showed a slight tendency towards a decrease in fear of movement during the 12-month intervention in the LSF-EX group compared with LSF-UC group, especially in accidental injury-related fear. The preoperative measurements showed that kinesiophobia was at a high level before the LSF surgery, but had decreased by the 3-month follow-up after surgery. However, participants’ physical activity levels remained unchanged during the first 3 postoperative months.
The TSK total score decreased significantly soon after surgery. This was understandable, as pain relief was experienced after surgery. It is also possible that patients’ fear of movement is lessened by the belief that surgery has remedied their lower back problem. The reference values reported for the Finnish TSK are 32.9 in women and 34.2 in men (21); these levels had already been reached when the exercise intervention began, i.e. at 3 months postoperatively. Therefore, the mean decrease in the TSK total score during the intervention was rather small. In previous RCT studies evaluating kinesiophobia during the postoperative rehabilitation of LSF patients, the interventions were carried out soon after surgery (11, 12). Abbott et al. compared psychomotor therapy with exercise therapy during the first 3 postoperative months in LSF patients. The psychomotor therapy consisted of behavioural therapy and exercises based on lumbo-pelvic stabilization training and motor re-learning approaches and was shown to be superior to the exercise therapy in decreasing kinesiophobia at the 3-month follow-up. The improvement remained unchanged up to the follow-up 2–3 years later (11). Monticone et al. (12) started their hospital-based intensive 1-month therapy protocol soon after surgery. They compared cognitive-behavioural therapy combined with supervised exercises with supervised exercises alone. They found that fear of movement and re-injury improved significantly more in the combined than exercise-only group (12). However, the timing and contents of the therapy in these 2 studies differ from those in our study. The present study also focuses on patients with spondylolisthesis only, while in previous studies the selection of primary diagnoses has been wider, including spinal stenosis (11, 12) and degenerative disc disease (11). In addition to differences in timing and patient samples, the present intervention was implemented by a physiotherapist and the training protocol was more physical than the protocols used in the previous studies (11–13). Although the booster sessions in the present study were conducted by a physiotherapist, the guidance given was also partly structured based on the cognitive behavioural model of the fear of movement/(re)injury (2).
During the intervention, the confidence of the LSF-EX group in the use of the back and trunk improved. LSF-EX improved significantly more in item 9 (“I am afraid that I might injure myself accidentally”) than LSF-UC, whereas the other items showed no significant between-group difference. In LSF-EX, change over time was significant for item 1 (“I’m afraid that I might injure myself if I exercise”). No previous studies have examined the TSK items separately after treatment.
In this study, in terms of meeting the criteria set for the minimum amount of physical activity considered to be health-enhancing, the level of physical activity reached during the 12-month intervention was acceptable in both groups (26, 27). This observation may partly be a result of the nature of the support provided, such as encouragement, and, in both groups, also partly due to relief from pain and reduced kinesiophobia. Based on this study, we can only speculate on the underlying associations; interestingly, however, Koho et al. (24) found a significant inverse association between kinesiophobia and physical activity in patients with musculoskeletal disease, but not in the cardiovascular or mental disorder subgroups. We propose a cycle, in which the reduction in pain achieved by surgery provided a safe foundation for an intensive back-training intervention. As pain and kinesiophobia decreased, physical activity started gradually to increase. The time-frame might also explain the increase in physical activity during the intervention in both groups: the first 3 months are the most critical phase in the postoperative healing processes, after which the majority of mobility limitations are removed. Because no severe adverse events or discontinuance due to intervention harms were observed, a programme like the present one seems to be feasible, also for elderly persons undergoing LSF. However, long distances (up to 150 km) from the hospital were challenging for some elderly patients, especially for attendance at booster sessions, and thus patient guidance should be organized closer to their homes.
The strengths of this study include the well-planned RCT setting. The data collection was well organized between the 2 hospitals, and special attention ensured that the treatment protocols were similar in both settings. The intervention was performed by physiotherapists skilled and experienced in scientific research and clinical practice. The exercise protocol and patient education materials were pre-planned by a multidisciplinary team, and based on previous scientific research (15). The drop-out rate and number of discontinued participants was very low, which adds to the credibility of the study. However, the study has some limitations. The nature of the study meant that it was not possible to blind caregivers and patients. Also, we did not collect data on the number of steps or exercise data from the LSF-UC participants, as the use of pedometers and exercise diaries could have affected their behaviour. Regardless of the regular booster sessions and individual guidance, compliance decreased during the intervention, and this may have influenced the results. When the TSK items were analysed separately, we did not use multiple testing, which may have affected the findings on the between-group differences for specific TSK items.
In conclusion, the progressive 12-month home-exercise programme, starting 3 months postoperatively, and including patient education and regular follow-up meetings, was not more effective than usual care after LSF in relieving kinesiophobia or increasing physical activity.
This study was funded by the Academy of Finland (133336) and grants from the Medical Research Funds of Tampere University Hospital (9M065, 9N048) and Central Finland Central Hospital (B12101, B13101 and B1403). The authors thank Kati Kyrölä, MD, Kirsi Piitulainen, MSc and Mirja Vuorenmaa, MSc from Central Finland Central Hospital and Ilkka Marttinen, MD, Kimmo Vihtonen, MD, Seija Rautiainen, Päivi Kolu, MSc, Saku Aalto and Tiina Kaistila, MSc, from Tampere University Hospital.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize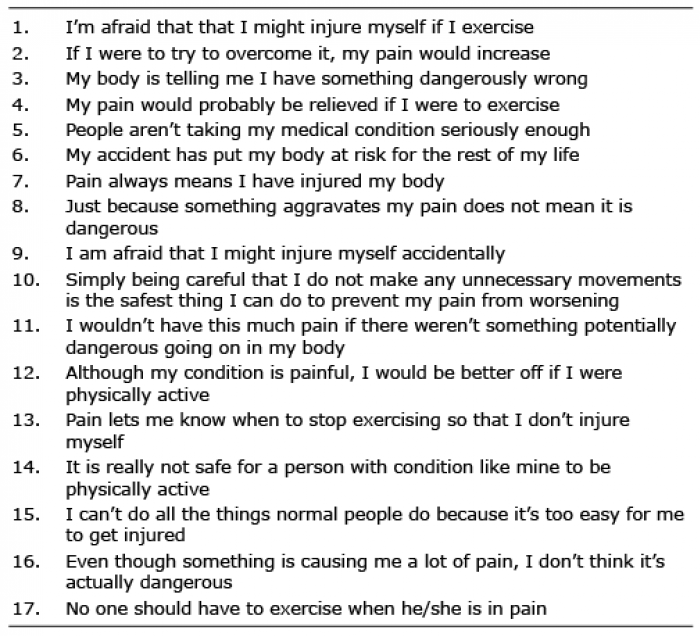 Click to show fullsize
Click to show fullsize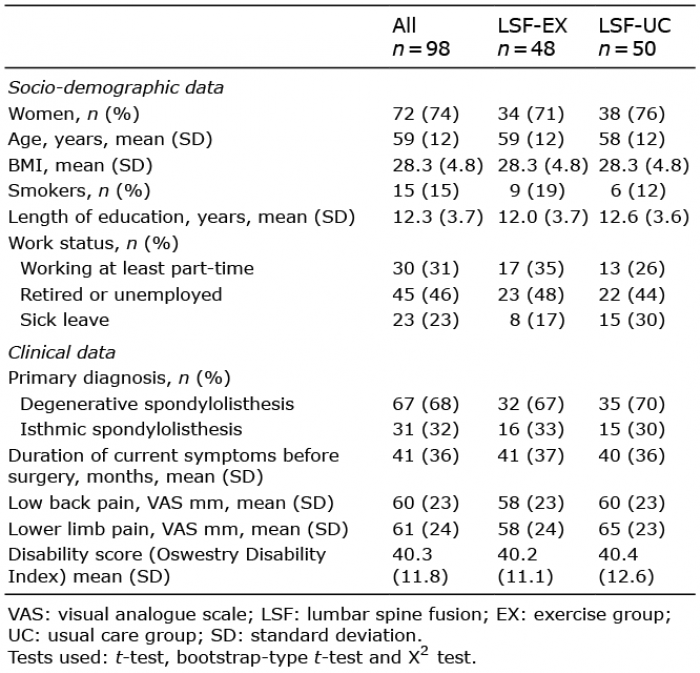 Click to show fullsize
Click to show fullsize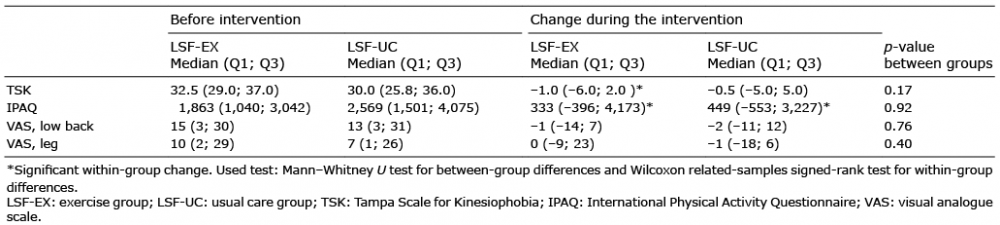 Click to show fullsize
Click to show fullsize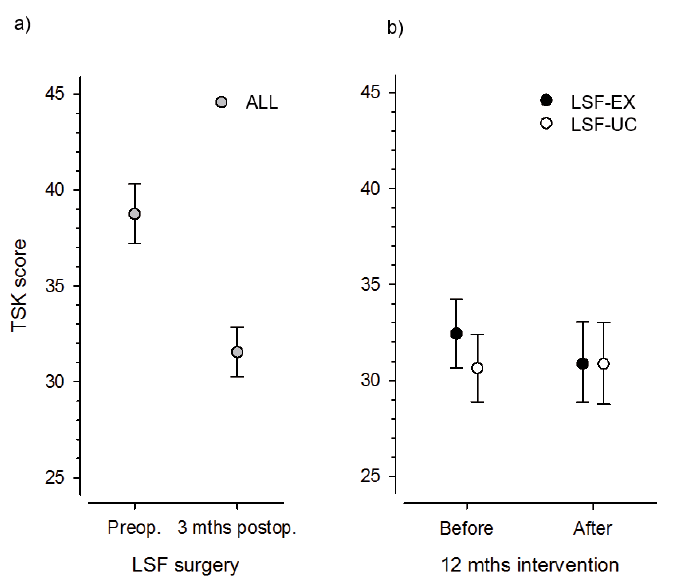 Click to show fullsize
Click to show fullsize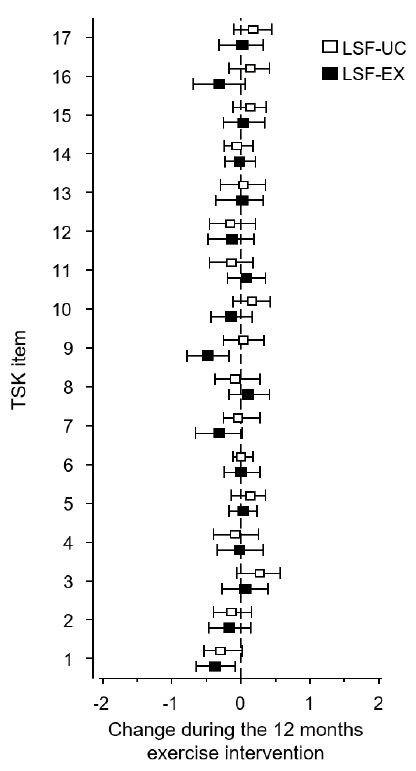 Click to show fullsize
Click to show fullsize