
From the 1Division of Physiotherapy, School of Health and Rehabilitation Sciences, The University of Queensland, 2Recover Injury Research Centre, The University of Queensland, Brisbane, Australia, 3Department of Medical and Health Sciences, Division of Physiotherapy, Linköping University, Linköping, 4Rehab Väst, County Council of Östergötland, Motala, 5Department of Rehabilitation and Department of Medical and Health Sciences, Linköping University, 6Physiotherapy Department, School of Health, Care and Social Welfare, Mälardalen University, 7Centre for Health and Medical Psychology, Örebro University, Sweden and 8School of Public Health, The University of Queensland, Brisbane, 8School of Medicine and Public Health, The University of Newcastle, Newcastle, Australia
Objective: To investigate the efficacy of exercise interventions and factors associated with changes in work ability for people with chronic whiplash-associated disorders.
Design: Secondary analysis of a single-blind, randomized multi-centre controlled trial.
Setting: Interventions were conducted in Swedish primary care settings.
Patients: A total of 165 individuals with chronic whiplash-associated disorders grade II–III.
Methods: Participants were randomly allocated to neck-specific exercise, neck-specific exercise with a behavioural approach, or prescribed physical activity interventions. Work ability was evaluated with the Work Ability Index at baseline, 3, 6 and 12 months.
Results: The neck-specific exercise with a behavioural approach intervention significantly improved work ability compared with the prescribed physical activity intervention (3 months, p = 0.03; 6 months, p = 0.01; 12 months, p = 0.01), and neck-specific exercise at 12 months (p = 0.01). Neck-specific exercise was better than the prescribed physical activity intervention at 6 months (p = 0.05). An increase in work ability from baseline to one year for the neck-specific exercise with a behavioural approach group (p < 0.01) was the only significant within-group difference. Higher self-rated physical demands at work, greater disability, greater depression and poorer financial situation were associated with poorer work ability (p < 0.01).
Conclusion: This study found that neck-specific exercise with a behavioural approach intervention was better at improving self-reported work ability than neck-specific exercise or prescribed physical activity. Improvement in work ability is associated with a variety of factors.
Key words: employment; whiplash injuries; exercise; persistent neck pain.
Accepted May 31, 2018; Epub ahead of print Aug 8, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Venerina Johnston, Division of Physiotherapy, School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Australia. E-mail: v.johnston@uq.edu.au
Most people who have sustained a whiplash injury return to, or remain in, work. However, some people with whiplash injury experience ongoing problems, with difficulty performing pre-injury work duties. This study investigated the efficacy of 3 different exercise interventions on self-reported work ability for individuals with chronic whiplash. Compared with prescribed physical activity, a 3-month neck-specific exercise intervention with a behavioural approach (including education on managing relapses and stress) was significantly better at improving work ability immediately after the intervention, and at 6- and 12-month follow up. The neck-specific exercise intervention with a behavioural approach was also more effective than neck-specific exercise alone after 12 months. Poorer work ability was associated with high physical demands at work, disability, depression and poorer financial situation. Physical therapists can improve work ability for individuals with chronic whiplash through a specific exercise regime with a behavioural approach.
Whiplash-associated disorders (WAD) following road traffic accidents are a common cause of persistent pain and disability (1), posing a significant burden on society (2, 3). There is also a financial burden on the individual with WAD in terms of long-term sick leave (4), slower and lower return-to-work rates than individuals sick-listed due to other musculoskeletal disorders (5) and lower employment opportunities compared with the general population (6).
Published rates of return to work (RTW) after WAD vary: from 44% (7) to 70% (8) after one year. Discrepancies in rates of RTW are probably due to heterogeneous study populations, varying legislation and benefits, definitions of RTW and study design. Nevertheless, the majority of individuals with a whiplash injury do RTW, although approximately half will continue to experience symptoms (9). These persisting symptoms are likely to impact on work, requiring a period of modified duties and/or reduced hours. Buitenhuis et al. (10) found that, of those in paid work after a WAD (total n = 733), 58% continued to be work disabled at one year. Similarly, Elfving et al. (11) showed that, while individuals with chronic WAD increased their working time after a 4-week rehabilitation programme, 62% continued to report problems with heavy work and lifting. A systematic review (12) of the effects of individual and work-related factors on work ability, as defined by the Work Ability Index (WAI), concluded that poor work ability was associated with a lack of leisure-time vigorous physical activity, poor musculoskeletal capacity, older age, obesity, high mental work demands, lack of autonomy, poor physical work environment, and high physical work load. Thus, interventions that address these factors are needed for individuals with WAD.
To date, most interventions considering work outcomes in people with WAD have been observational cohort studies (11, 13–15). The few randomized trials conducted in which work outcomes were reported included a heterogeneous sample of individuals with acute (16–18) or subacute WAD (19). No randomized trials were found that included individuals with chronic WAD. The interventions tested showed small or no improvement in work outcomes. Outcomes that have been used previously, such as RTW (yes/no) or duration of sick leave are not appropriate, as they are tied to the current social security system, employer or country. A measure such as the WAI better reflects an individual’s ability to meet the occupational demands of their job and enables comparisons between studies, organizations and countries.
The current study is a secondary analysis of data to compare the efficacy of a neck-specific exercise intervention with (NSEB) and without (NSE) a behavioural approach, and prescribed physical activity (PPA), on self-reported work ability for individuals with chronic WAD grade II–III over a 12-month period. We hypothesized that participation in the NSEB would demonstrate a greater improvement in work ability compared with the other interventions. A secondary aim is to determine which of several individual, psychosocial, work and condition-specific factors is associated with changes in work ability following exercise interventions in chronic WAD.
This prospective randomized controlled trial was registered at ClinicalTrials.gov (NCT01528579) (20). The sample size was calculated based on the primary outcome measure (7% change in Neck Disability Index) (21). Assessors were blinded. However, participants and treating physical therapists could not be blinded due to the nature of the treatment. Informed consent to participate in the study was obtained before randomization.
The intervention was delivered by experienced physical therapists in the Swedish primary-care setting. Potential participants who had sought medical assistance for WAD from Swedish healthcare in 6 counties were recruited from February 2011 to May 2012, until the calculated sample size was achieved.
Participants aged between 18 and 63 years, diagnosed with WAD grade II/III, with persistent pain and disability associated with WAD that occurred 6–36 months before recruitment, who reported a score of at least 20% on the Neck Disability Index and/or 20 mm on a pain visual analogue scale (VAS) were eligible. Participants were excluded if they had persistent symptoms due to other neck trauma, previous neck surgery, spinal infection, tumour, myelopathy, signs of traumatic brain injury, a more dominant or generalized pain in other body regions, serious neck pain causing absence of work for more than one month in the previous year, or other conditions that would limit full participation in the study, such as drug abuse, a severe psychiatric disorder or limited ability to communicate in Swedish.
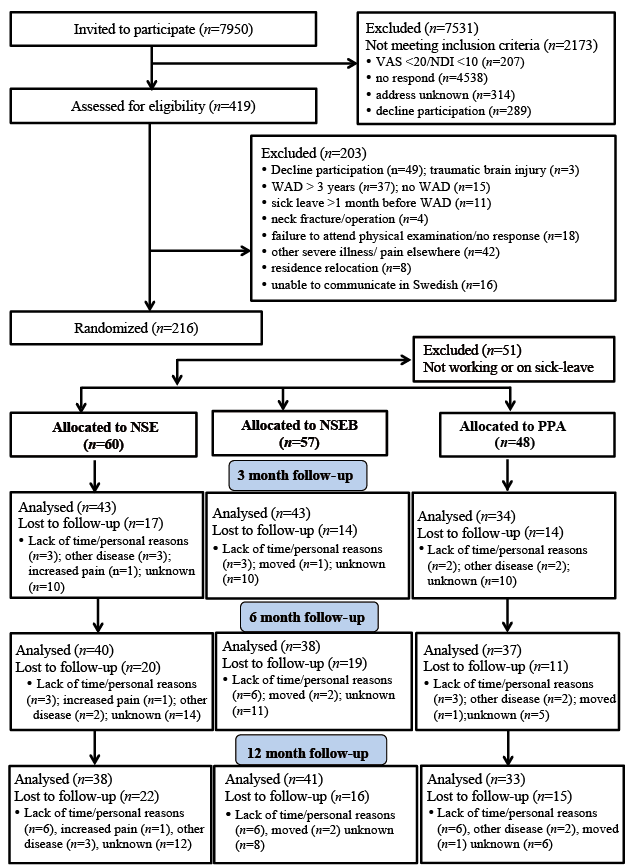
Potential participants were invited by post (n = 7,950). Those who responded and met the self-reported inclusion criteria received a phone interview to confirm their eligibility (n = 419), followed by a physical examination conducted by a physical therapist to confirm WAD grade (n = 216). Specific for this secondary analysis, only those who were currently employed, or who were employed at the time of their accident, constituted the sample population (n = 65) (Fig. 1). Further details of participant recruitment are provided in Ludvigsson et al. (20).
Fig. 1. Flow diagram of participants through the study. NSE: neck-specific exercise; NSEB: neck-specific exercise with a behavioural approach; PPA: prescribed physical activity intervention; VAS: visual analogue scale; NDI: Neck Disability Index; WAD: whiplash-associated disorder.
Participants were randomly assigned to receive NSE, NSEB or PPA. An independent researcher allocated participants into different groups using a computer-generated list compiled by a statistician. Individual results were placed in opaque envelopes and sent to the independent treating physical therapists.
The interventions (published in detail elsewhere) (20) were led by physical therapists who received one day of standardized practical and theoretical training from project leaders prior to commencement of the study. Guidance from project leaders was also provided as required. Participants were encouraged not to receive other physical treatment for their neck problem during the 3-month intervention. On completion, participants were encouraged to continue with the prescribed exercises.
Neck-specific exercise. The NSE intervention was supervised by physical therapists and performed twice weekly for 3 months. Patients were encouraged to practice the exercises at home. Education on the musculoskeletal system of the neck and information about WAD were provided. Patients were encouraged to avoid pain aggravation during the exercises. The exercises were low load initially then gradually progressed, with increased repetitions and resistance (22). Postural control was also introduced to facilitate deep cervical muscle function. On completion, a written exercise programme and prescribed general exercise were provided to encourage participants to continue those exercises.
Neck-specific exercise group with behavioural approach. The exercise component of the NSEB intervention was the same as in the NSE group, with the addition of a behavioural component. The concept of graded activity was used to educate patients not to focus on temporary increases in neck pain. As WAD has a strong psychosocial component and several psychological and social work factors contribute to work ability (23), a behavioural approach was added to moderate the detrimental effect of some psychological factors. The behavioural component included education on the basic neuroscience of pain and how to manage pain, including relapses. Patients were also taught relaxation exercises and to decrease stress and muscle tension. Moreover, participants were empowered to set specific, measurable, achievable, realistic and time-bound (SMART) goals and progress exercise with guidance from the physical therapist. Similar to the NSE group, participants were encouraged to continue exercise after the intervention period.
Prescription of physical activity. In the PPA group, a motivational interview and physical examination was conducted in the first week by a physical therapist to inform an individualized physical activity plan. It aimed to increase the level of physical activity to improve fitness, with participants expected to complete the prescribed exercise outside the Swedish healthcare system or at home. No neck-specific exercises were prescribed. Participants were encouraged to receive either a phone call or attend a follow-up visit to monitor their progress, but this was optional (20).
The WAI was used to evaluate self-reported work ability and has been demonstrated to be a reliable and valid tool to predict work disability and retirement (24). It consists of a 7-item self-assessment of: current work ability compared with lifetime best, work ability in relation to the physical and mental demands of the job, number of current diagnosed diseases, estimated physical work impairment due to disease, sick leave during the last year, self-rated prognosis of work ability 2 years from now, and mental resources. The total score, between 7 and 49, was used to categorize participants into poor (7–27), moderate (28–36), good (37–43) and excellent (44–49) work ability (25). WAI scores were recorded at baseline before group allocation, and at 3, 6 and 12 months after commencement of the intervention. The change in WAI scores was included as the dependent variable in all analyses.
Potential explanatory variables assessed at baseline include: demographic (age in years, education level, financial situation, smoking status, body mass index), individual, psychosocial, work- and condition-specific, exercise factors and beliefs. Current employment status and employment status prior to their accident was determined by a series of questions about their main source of income prior to and after their WAD (paid employment, retirement, sick leave, parental leave, student aid, unemployment benefits, social security benefits, other). If not working because of their injury, the date of the last working day was recorded. Further details of the included measures are provided in the protocol for this trial (21).
Individual factors: EuroQol Five Dimension Scale and EuroQol VAS were used to measure health-related quality of life. Self-reported financial situation (good/normal/bad) and whether patients were worried about their financial situation were collected, as socio-economic inequalities have been shown to be significantly associated with work ability (26).
Psychosocial factors. Pain catastrophizing was evaluated with the Pain Catastrophizing Scale. The Tampa Scale of Kinesiophobia was used to measure fear of movement. Anxiety and depression was evaluated with the Hospital Anxiety and Depression Scales. Self-efficacy of performing daily activities with pain was rated with the 20-item Self-Efficacy Scale (0–200).
Work-specific factors. Flexibility of the work place was rated trichotomously (never/sometimes/always) for the possibility of: obtaining help from colleagues, choosing work tasks, having longer breaks at work than usual, working at home and working undisturbed. Change of work tasks, satisfaction with work tasks and the workplace were recorded dichotomously (yes/no). Perceived neck load at work was also measured with one question: “Do you consider the load on your neck at work is: light, moderate or heavy”. The Borg scale (6–20) was used to indicate the intensity of physical demands at work. A binary scale (hardly ever/frequently) was used to measure the frequency of having arms above shoulder height for more than 30 min. The Effort-Reward Imbalance Scale was used to measure work-related stress. The type of employment was also recorded (full-time/part-time).
Condition-related factors. WAD grade (II/III) and time since the accident (months) were recorded. Treatment received after their WAD injury, consultation with a physical therapist, other health professionals and use of pain medication (yes/no) were recorded. The presence of previous neck pain, back pain and current arm symptoms were also recorded dichotomously (yes/no). The frequency of symptoms was measured dichotomously (occasionally, frequently) for neck pain, arm pain, headache, paraesthesia, neck stiffness, nausea and dizziness. Frequency of problems with swallowing, jaw, hearing, vision, sleeping, concentrating and arm lifting were also measured dichotomously. A VAS was used to record neck pain and pain bothersomeness (0–100 mm, 100 = worst pain, and extremely bothersome). The level of disability due to chronic pain and neck pain were measured with the Pain Disability Index (score range 0–70) and Neck Disability Index (NDI, 0–100%), respectively.
Exercise factors and beliefs. Exercise Self-Efficacy Scale was used to rate participants’ confidence on doing exercise (0–100) (27). Activity level was evaluated with International Physical Activity Questionnaire (low/moderate/high) (28). The expected treatment result was recorded on a 4-point scale (fully recovered/substantial improvement/some improvement/no expectation).
Adherence during the active intervention period was recorded by the physical therapists in the NSE and NSEB groups and from exercise diaries of participants in the PPA group after the 3-month intervention. Maintenance of the exercise intervention after completion of the intervention at the 6- and 12-month follow-ups was determined by self-report response to one question. Exercise adherence during the active participation and maintenance phase was recorded as greater or less than 50%.
The analysis was performed with an intention-to-treat approach. Descriptive statistics used to summarize all included baseline variables were one-way analysis of variance for continuous variables and χ2 tests for categorical variables. Generalized estimating equations (GEEs) were used to investigate whether a statistically significant effect of the interventions on WAI was evident over time. GEEs were used to account for correlation between participants after repeated measures, all variations in missingness of data, and unevenly spaced observations in longitudinal data. A Gaussian distribution, identity-link function GEE model was applied in the analysis and adjusted for significant factors of association with the changes in WAI scores (dependent variable). All independent variables were tested for their association with the dependent variable through a series of univariate analyses. Variables were retained if significant at 5% and model correlation structure was assessed using the Quasi-likelihood Information Criterion (QIC), a version of the Akaike Information Criterion (AIC). Interactions between independent variables (group × time, group × age and group × sex) were taken into consideration. Sex, age, group, time and group × time interaction were forced into the final model. Pairwise comparisons were used to compare between (intervention groups) and within differences (time points). STATA version 14 (Stata Corporation, College Station, TX, USA) was used for all data analysis and p < 0.05 was accepted as statistically significant, with no adjustments for multiple comparisons.
Of the 216 participants randomized, 165 met the employment inclusion criteria and completed the WAI and were thus included in the study (Table I). Overall, baseline background characteristics between the 3 intervention groups were similar. There were no significant differences in mean WAI score at baseline (35.3, 36.0 and 34.9, p = 0.64) and percentage of female participants (73.3%, 66.7% and 52.1%, p = 0.07) in the 3 intervention groups, NSE, NSEB and PPA, respectively. However, participants in the NSE and NSEB groups were significantly younger than those in the PPA group (mean age 39, 40 and 44 years, respectively, p = 0.03). More participants in the NSE intervention had received treatment after WAD than in the NSEB and PPA groups (p = 0.01). The mean and SD for the factors significantly associated with WAI in the final model are shown in Table I. The mean WAI raw values and the relative percentage change from baseline at each time-point for each group are shown in Table II. There was a relative increase in work ability from baseline for participants in both exercise groups, with a corresponding decrease in the PPA group. Participants lost to follow-up at 12 months did not significantly differ in baseline characteristics or measures (age, sex, WAD grade II–III, level of pain, self-reported work ability, neck disability score and pain disability measure, p > 0.21).
Table I. Baseline background characteristics of participants
Table II. Work Ability Index score: raw values and percentage change from baseline at each time-point
Between-group differences for the WAI at 3, 6 and 12 months are shown in Table III. The NSEB intervention was significantly better in improving work ability than the PPA intervention immediately after the intervention (3 months, p = 0.03) and at all the follow-ups (6 months, p = 0.01; 12 months, p = 0.01). However, the NSEB intervention only showed significant improvement in work ability compared with the NSE intervention at 12 months (p = 0.01). There was a significant difference between the NSE and PPA interventions only at 6 months.
Table III. Differences in Work Ability Index between groups over timea
Within-group differences for work ability demonstrated that participants in the NSEB intervention significantly improved work ability from baseline to one year (p < 0.01), although no significant short-term improvement was observed. Only a trend of improvement over one year for participants in the NSE intervention was observed (Table IV). In contrast, those in the PPA intervention had a trend of decreasing work ability over time.
Table IV. Within-group changes in Work Ability Index over time for each groupa
In preliminary testing, there were no significant interactions between group and age (group × age, p = 0.93) or sex (group × sex, p = 0.33). However, interaction between group and time was significant (p = 0.03). An unstructured correlation structure was used in the modelling as it produced the lowest QIC value compared with other alternatives, such as independent or exchangeable. Table V displays the results of the final model for the interventions on WAI after controlling for significant variables and adjusting for age, sex, time and group × time interaction. Overall, group allocation was not significantly associated with the score on the WAI over one year (p = 0.16). In the final predictive model, in order of magnitude of coefficients the variables associated with a decrease in WAI over one year were: moderate and heavy load on the neck at work, poorer financial situation, depression and greater pain-related disability (p < 0.01).
Table V. Factors associated with changes in Work Ability Index (WAI) over one year using generalized estimating equations (GEE)a
Adherence to the PPA intervention (50%) was significantly less than to the NSE (72%) and NSEB (80%) interventions (p = 0.02) at 3 months. However, the percentage of participants who had completed more than half of their prescribed exercise during the maintenance phase was similar at 6 months (p = 0.55) and 12 months (p = 0.26). At 6-month follow-up, participation in exercise was 42%, 51% and 48% in the NSE, NSEB and PPA groups, respectively. At 12 months, participation in the NSE group was still lower (26%) than in the NSEB group (33%) and both were higher than the PPA group (18%).
This study investigated the efficacy of 3 different exercise interventions on self-reported work ability for individuals with chronic WAD grade II–III and which baseline characteristics were associated with the WAI over time. The results show that NSEB intervention was significantly better than PPA intervention for improving work ability. An improving trend in work ability was found only in the NSE and NSEB interventions, with participants in the NSEB intervention having significantly improved work ability after one year. Of concern was the trend of decreasing work ability in those participating in the PPA intervention. Overall, the NSEB intervention was more efficacious in improving self-reported work ability than the NSE and PPA interventions.
The conceptual background of work ability is based on the stress-strain concept and balance model, in which a balance between a person’s resources and work demands is required to safeguard health (29). The finding that the overall mean baseline self-reported work ability of the participants in this study was 35.4, indicating moderate work ability, suggests that individuals with WAD are under some strain requiring additional support. This score is higher than workers with chronic neck pain and those on long-term sick leave (mean score 19.1) (30). This is not unexpected, as only those who were employed completed the WAI, and they would have higher work ability than those on sick leave.
These results support our hypothesis that NSEB is superior in improving self-reported work ability compared with the other 2 exercise interventions tested (NSE and PPA) despite similar adherence during the maintenance phase at 6- and 12-month follow-ups. The addition of a behavioural component may have allowed patients to problem-solve their symptoms during a relapse, learn skills to manage pain with relaxation exercises, and succeed in exercise progression. It is recognized that work ability is related to both condition-specific and psychosocial factors for individuals with chronic WAD (31). The addition of the behavioural approach may address the psychosocial risk factors, similar to that of a psychosocial risk reduction intervention, which is suggested to be effective in improving function and return to work for people with WAD (32). Our results are similar to a study that showed that exercises with a cognitive behavioural approach improved self-evaluated work ability in workers with low back pain (33).
The results suggest that the NSE intervention is more efficacious in improving work ability than is PPA, but only at 6 months. A possible explanation for this is that NSE alone was insufficient to improve work ability, as work ability is dependent on the interactions between organizational factors involving the work environment, work content and demands, the work community, and leadership (34). The NSEB intervention was only statistically significant in improving work ability at one year compared with baseline, with an increase of at least 3 points previously accepted as “improved work ability” (35). This suggests that behavioural skills might take time to develop and master.
The PPA group showed a trend of decreasing work ability over time, even though physical exercise has been shown to maintain work ability for workers in the metal and retail industry (36). This may be due to lower participation in the PPA group than either of the neck-specific exercise groups during the intervention period and at 12 months, or that general exercise alone is insufficient to create change in chronic WAD. This finding suggests that the chronic WAD population is at risk of decreasing work ability if their concerns are not addressed, and increasing physical activity alone may not be effective in improving work ability. In the final model time was not significantly associated with work ability, indicating that work ability does not improve over time without specific interventions in individuals with chronic WAD. As self-reported work disability is less likely to change over time for individuals with WAD, early intervention should be implemented to maintain and improve work ability even if workers have returned to work. This study also shows that existing work ability for individuals with chronic WAD grades II and III can be improved with appropriate treatment.
The following baseline characteristics: increased perceived neck load at work, greater disability due to pain, greater depression and poorer self-rated financial situation were significantly associated with a reduction in WAI over one year. Similar findings have been reported in the literature for populations with WAD, in that a combination of work-related, pain-related, psychological and individual variables is prognostic for work-related outcomes (31).
Several individual and work-related factors were associated with work ability for individuals with WAD, of which some were consistent with a recent review (12). Increased perceived physical neck load at work was significantly associated with poorer work ability. This is consistent with previous reports that high physical demands at work may impair work ability (35). As the majority of participants in this study (83%) reported moderate to heavy physical neck load during work, it is possible that delivering an NSEB intervention with ergonomic advice on safe work procedures may achieve additional gains in work ability. At an organizational level, employers can contribute to improving work ability through ergonomic interventions, as workplace ergonomics can significantly influence an individual’s work ability (35). Greater disability due to pain, as indicated by the Pain Disability Index, was one of the significant contributors to poorer work ability (37). It is possible that greater self-rated disability in normal life would translate to self-rated disability in work. This is consistent with the literature that greater disability is linked to increased recovery time (1). Our findings indicate that depression was significantly associated with poorer work ability. Consistent with the literature, workers with depression in the general population are at greater risk of having lower work ability in the long term (38). Depression is common in individuals with chronic WAD, thus mental health support may be needed for this population. Poorer self-rated financial situation was also found to be significantly associated with decreased work ability. Perceived financial situation is linked with mental health and perceived employment commitment (39).
This study has several strengths. It is the first to report the efficacy of an exercise intervention on work ability for individuals with chronic WAD grades II and III. In addition, the generalizability of our results is enhanced by the fact that participants were randomly allocated to the different interventions, conducted in multiple primary care centres.
Several limitations may have influenced the findings of this study. Firstly, it is a secondary analysis of a randomized controlled trial, which was not powered to detect a change in the WAI. Only those who were currently employed, or were employed prior to their WAD injury, completed the WAI questionnaire, which may explain the relatively high baseline WAI score and limited sample size. Secondly, this was an exploratory study, as a large range of baseline variables with the potential to influence work ability were included. However, controlling for the significant variables increases our confidence that any changes observed are probably due to the efficacy of the intervention. Participation in the intervention was reasonable during the active period, but reduced substantially over time. It is possible that stronger results would have been noted with better participation, although no minimum threshold has been established. The loss to follow-up over the 12-month trial varied from 24% to 30%, which may bring the validity of the results into question. However, at 12 months, the majority (> 63%) of participants remained in the study. It is possible that other factors not assessed in this study may have contributed to the changes observed. For example, Tuomi et al. (35) found that reduced management strain and improved work postures and greater satisfaction with the supervisor’s attitude was associated with improved work ability over an 11-year period, while Emberland et al. (23) found that role conflict and human resource primacy and positive challenge were most predictive of work ability in a 2-year prospective study. Nevertheless, the study is novel; the results provide insight into how best to improve work ability for individuals with chronic WAD. Further research is needed into how best to support individuals with chronic WAD to remain at work in the short term and how best to support those on sick-leave. Interventions that include the workplace, such as enhancing the individual’s self-management skills to make adjustments at work, and targeting the supervisors, may promote staying at work (37). This approach is consistent with the multidimensional model of work ability that emphasizes the importance of having control over one’s work and the way in which it is organized (40).
In summary, a NSEB intervention was better at improving self-reported work ability than NSE alone or PPA. The results of this study suggest that improvement in work ability is associated with work-related, pain-related, psychological and individual factors. A NSEB intervention shows promise for improving work ability in those remaining at work with a WAD grade II–III injury. Further research is needed to identify interventions that will be effective in promoting work ability in the short- and long-term in this population.
The authors thank all the participants, physical therapists and staff involved in any stage of the study.
The Regional Ethics Committee at the Medical Faculty at Linköping University in Sweden provided ethics and has granted approval for the protocol (2010/18888-31 and 2011/262-32).
The study was funded by the Swedish government through the Swedish Research Council, in cooperation with the Swedish Social Insurance Agency through the REHSAM Foundation Stockholm, Sweden, and the regional Centers for Clinical Research and the County Council of Östergötland, Linköping, Sweden and Sörmland, Uppsala, Sweden Research Council of Southeast Sweden.


 Click to show fullsize
Click to show fullsize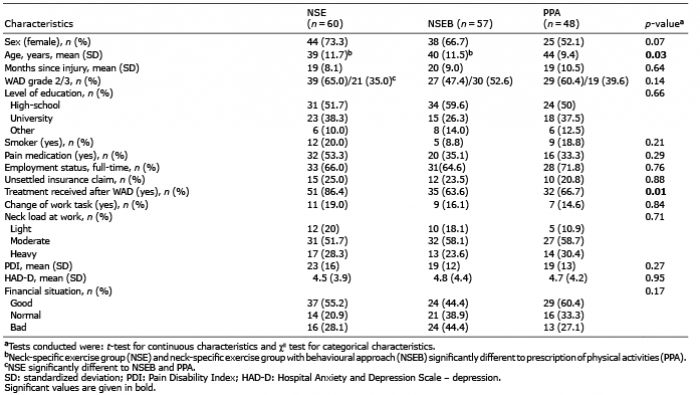 Click to show fullsize
Click to show fullsize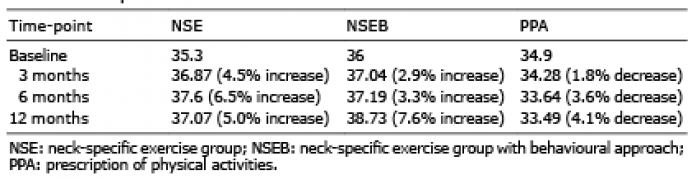 Click to show fullsize
Click to show fullsize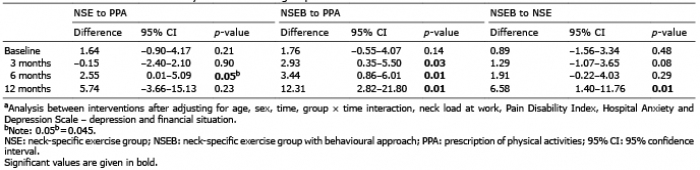 Click to show fullsize
Click to show fullsize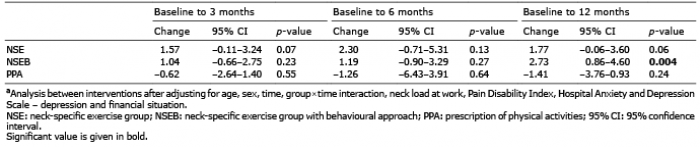 Click to show fullsize
Click to show fullsize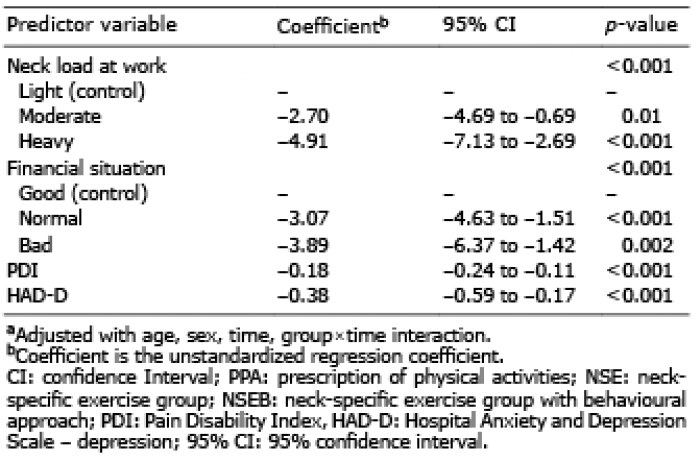 Click to show fullsize
Click to show fullsize