
From the 1Department of Clinical Neuroscience and Rehabilitation Medicine, Institute of Neuroscience and Physiology and 3Department of Health and Rehabilitation, Sahlgrenska Academy, University of Gothenburg, and 2Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden
Objective: To update the evidence surrounding the presence of anxiety after stroke.
Data sources: A search was conducted in EMBASE, MEDLINE, PsycINFO, Cochrane Library, AMED and CINAHL in May 2015 and repeated in April 2017.
Study selection: Clinical diagnosis of stroke and assessed for anxiety symptoms on a rating scale in the first year after stroke.
Data extraction: One reviewer screened and identified studies against the inclusion criteria. A second reviewer conducted a random check of approximately 10% of titles and abstracts. Two authors independently performed the final full-text review.
Data synthesis: Overall pooled prevalence of anxiety disorders was 29.3% ((95% confidence interval 24.8–33.8%), (I2 = 97%, p < 0.00001)) during the first year. Frequency 0–2 weeks post-stroke was 36.7%, 2 weeks to 3 months 24.1%, and 3–12 months 23.8%. There was a statistically high heterogeneity in this estimate (I2 = 97%, p < 0.00001).
Conclusion: Anxiety is common during the first year post-stroke. Since anxiety significantly influences quality of life and is a predictor for depression, it may be worth considering further routine screening post-stroke.
Key words: anxiety; epidemiology; stroke; review.
Accepted Jun 27, 2018; Epub ahead of print Sep 5, 2018
J Rehabil Med 2018; 50: 769–778
Correspondence address: Lena Rafsten, Institute of Neuroscience and Physiology, Rehabilitation Medicine, University of Gothenburg, Per Dubbsgatan 14, fl. 3, SE-413 45 Gothenburg, Sweden. E-mail: lena.rafsten@vgregion.se
Anxiety is common during the first year after you have been diagnosed with stroke, with one in three experiencing it. Today anxiety after stroke gets significantly less attention compared to other psychological problems after stroke and one has reported dissatisfaction with the provision of psychological services after stroke. Since anxiety significantly influences quality of life, it is prevalent, and could be a predictor for depression. In this review, we have looked at the prevalence of anxiety at different times after stroke. We found that 29.3% of the patients had some form of anxiety disorders during the first year after stroke. The highest frequency, 36.7%, was 0–2 weeks after stroke onset. We suggest that clinicians should be more aware of anxiety that further routine screening post stroke may be worth considering providing appropriate interventions.
Stroke caused by cerebral infarction or cerebral haemorrhage is the leading cause of permanent disability in adults, and is the second largest cause of death after heart attack and cancer (1). More than 25 million people worldwide are diagnosed with stroke, and 6.5 million people die from stroke every year (2), with approximately equal representation between the sexes.
As well as physical disability, persons with stroke can experience a variety of physiological consequences, such as various mood disorders, which can compromise the rehabilitation process and influence long-term recovery (3). It is estimated that every fourth individual at some point in life will experience an anxiety disorder (4), which can be a natural, and sometimes a vital, reaction to coping with stress and life-threatening events. The word anxiety is taken to mean something that feels uncomfortable, with feelings such as frustration, boredom, worry, despair, and guilt all fitting within this concept. From a psychological perspective, anxiety is a type of fear or worry. The physical aspect of anxiety is stress, an internal pressure or restlessness, a body sensation which creates discomfort (5). A low level of anxiety is often described as worry or trouble, while a higher level often seems like fear or panic (6).
After stroke onset, anxiety is a common symptom both in the acute phase, after months, and after years (7–9). A systematic review from 2012 reported that approximately 20% of people with stroke sometimes experience anxiety to varying degrees (10), but later studies have shown that more than one-third of subjects reported worry and anxiety post-stroke (11, 12). Individuals recovering from stroke worry about recurrence of stroke, their ability to return to work, occurrence of fall accidents, etc. (11, 12). Anxiety and worry are also shown to be associated with a decreased quality of life (13). Studies have shown that the Hospital Anxiety and Depression Scale (HADS) subscale for anxiety correlate significantly with the Stroke Specific Quality of Life (SSQOL) a total score, score for energy, mood, personality, social roles, family role, thinking, and work/productivity. The severity of the anxiety syndrome after stroke is independent of sex or depressive symptoms and is associated with a general low post-stroke quality of life (14). It is known that post-stroke depression is common and has a negative impact on the risk of accidents and rehabilitation (15). A review from 2012 concluded that anxiety after stroke gets significantly less attention compared with other psychological problems after stroke (10) and a large-scale survey has reported dissatisfaction with the provision of psychological services after stroke (16).
The HADS is a 14-item self-assessment mood scale specifically designed for use in non-psychiatric hospital departments and is presented as a reliable and valid instrument for screening for clinically significant anxiety and depression after stroke (17, 18). The scale is frequently used for the assessment of depression and anxiety in stroke patients (19–22). HADS can be divided into 2 equal parts, HADS-A, anxiety, and HADS-D, depression. A systematic review of a large number of studies identified a cut-off point of 8/2 for both subscales (18). However, studies in stroke patients indicate that lower cut-offs (Anxiety: 5–7; Depression: 4–8) would be more appropriate for this population (18, 21–23).
While a systematic review that covered up until March 2011 investigated the frequence of anxiety after stroke, and coincides well with our aims and interests, it has been 6 years since it was completed (10). In the years since, there has been a lot of change within the healthcare system in Sweden, with shortened care times (24), fewer follow-ups, etc., which may have impacted on the incidence of anxiety, as well as potential for a change in the incidene of anxiety generally regardless of changes to the healthcare system. We feel, therefore, that it is important to perform a new systematic review. The main aim of this review is to update evidence about the presence of anxiety during the first year after stroke. The second aim is to perform meta-analyses on those studies that have used HADS as assessment of anxiety after stroke during the first year after stroke.
An electronic search in EMBASE, MEDLINE, PsycINFO, Cochrane Library, AMED and CINAHL was conducted in May 2015 and repeated in April 2017, and reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (25). A combination of MeSH terms and key words were used: “stroke” or “cerebrovascular disorders” or “cerebrovascular accident” or “post stroke” combined with “anxiet” or “anxiousness” or “emotions” or “stress” or “anxiety disorders” or “posttraumatic stress” or “distress” or “mental health” or “neurotic disorders” or neurotic” or “worry” or “fear”. To narrow the search, the following search limitations were used: systematic review, review, available abstract, publication date from 1 Jan 2011 to 13 May 2015, humans, in Swedish, English, Danish, or Norwegian (see Appendix S11 for detailed search strategy). A librarian, independent of the study, performed the electronic search. One reviewer (LR) screened and identified studies against the inclusion criteria. A second reviewer (AD) conducted a random check of approximately 10% of titles and abstracts to check the reliability of the initial screening. When the decision on inclusion was not clear based on the title or abstract, studies were selected for further full-text screening. The final inclusions were made by reviewing the full-text articles to determine if studies met the inclusion criteria and were performed independently by 2 reviewers. Disagreements between the 2 reviewers were resolved through discussion and, if required, a third experienced colleague was consulted as reviewer. As a second stage, a hand search of the reference lists from the included studies was conducted. Study authors were contacted for additional data, where necessary. Data extraction from the included studies was made by the 2 independent reviewers (LR and AD) through a standardized extraction sheet.
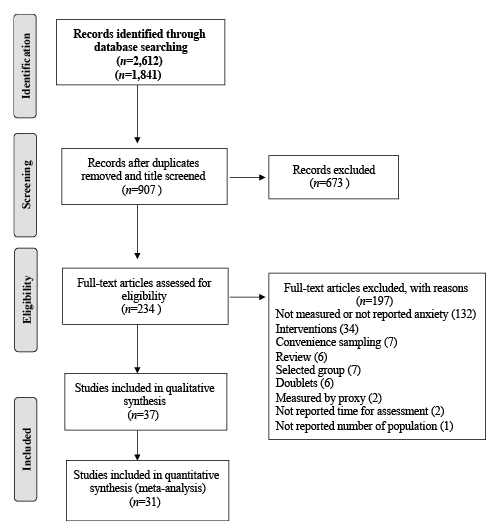
This review includes studies with groups with a clinical diagnosis of haemorrhagic or ischaemic stroke or transient ischaemic attack (TIA), diagnosed with anxiety or assessed for anxiety symptoms on a rating scale, such as the HADS, during the first year after stroke onset. A flow chart of the inclusion process is shown in Fig. 1.
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow chart of search process and reasons for exclusion of full-text articles.
Studies were excluded if they:
reported anxiety as a continuous outcome and we were unable to obtain a categorical assessment from the author;
measured anxiety by proxy.
Information about study design, setting, and patient characteristics was extracted using a standardized extraction sheet. Study quality and the potential risk for bias was assessed by 2 review authors using the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU) checklist for assessment of study quality – observational studies, which uses the following scale: Low, Medium, High. The score evaluated possible selection bias, such as bias in the method of recruitment, assessment bias such as the validation of the assessment instrument used to measure anxiety, failure bias such as proportion lost to follow-up. At a minimum, it was also expected that age and sex would be reported.
Studies were grouped into 4 categories, depending on where the patients were recruited (hospital, rehabilitation, community, population). Percent and meta-analyses were calculated using the random effects model with a forest plot to take into account the heterogeneity within and between studies. A χ2 test was used to test for subgroups differences. Heterogeneity among studies was assessed by means of the Q-test, and I² was used to estimate the magnitude of heterogeneity among studies. It was interpreted as low (0–25%), moderate (25–50%), substantial (50–75%) and high (75–100%) heterogeneity. Eggers regression asymmetry test was used to confirm any heterogeneity. A confidence interval excluding zero was considered significant. If the summary results present signs of heterogeneity we made new analyses, where studies of poorer quality or ones that are borderline were excluded. In studies that measured anxiety at multiple time-points, the earliest measurement from each study was used in the meta-analysis to measure the overall prevalence. To estimate the effect in different subgroups, such as cut-off value for HADS-A, study population source (hospital, rehabilitation, community, and population) and time post-stroke, several meta-analyses were performed on those studies using HADS as assessment for anxiety. The analyses were made using Review Manager 5:3.
The search from April 2011 to May 2015 produced 2,612 references, of which 19 publications met the inclusion criteria of this review (Table I). An updated search run in April 2017 found 1,841 studies, of which 18 publications met the inclusion criteria, giving a total of 37 studies and 13,756 unique stroke patients included in this review. The search process and reasons for exclusion of the full-text articles are provided in a PRISMA flowchart (Fig. 1).
Anxiety was assessed 2 days to 1 year post-stroke. Mean age of participation ranged from 52 to 79 years, and 36–73% of the participants were men (Table I).
The included studies came from all over the world, 60% were from Europe. Of the 37 included analyses, 27 took place in an acute hospital setting (14, 26–52) including 10,697 participants, 3 in rehabilitation settings (7, 53, 54) including 330 participants, 6 in the community (33, 48, 55–58) including 2,729 participants, and one in the population setting (29) including 3,373 participants (Table I). The eligible participation rate in these 3 study types ranged from 2% to 100%, and 6 studies (30, 37–40, 45) failed to provide information about the number of eligible stroke patients. Twenty-three of the included studies were of prospective designs, 13 studies of cross-sectional design, and the remaining study was a case-control study.
Twelve studies assessed anxiety within the first 2 weeks post-stroke (26–28, 35, 39–41, 46, 47, 52, 53, 59), 17 studies between 2 weeks and 3 months post-stroke (7, 14, 29–32, 36, 37, 42, 44, 45, 49–51, 54, 55, 60) and 8 studies assessed between 3 months and 1 year post-stroke (33, 34, 38, 43, 48, 56–58).
Clinical diagnoses of anxiety disorders were made according to HADS-A in 31 studies (7, 14, 27–42, 44, 46, 48–52, 54–59). The Hamilton Anxiety Rating Scale (HAM-A) was used in 3 studies (26, 43, 45) and State-Trait Anxiety Inventory (STAI), Generalized Anxiety Disorder test (GAD-7) and Hamilton Depression Rating Scale (HDRS-17) in 1 study, respectively (47, 53, 60). The cut-offs used in the studies using HADS-A ranged from > 6 to ≥ 11. In the studies using HAM-A the cut-offs ranged from > 5 to ≥ 8. The study using STAI did not report any cut-off and, in the studies using GAD-7 and HDRS-17, they used ≥ 10 and ≥ 1, respectively. Due to HADS-A being the most common used rating scale and the scale we used in a study of ours, we decided to include only the studies that used this in our meta-analysis. One study did not report any cut-off, and the authors did not answer our attempts to contact them, and therefore the study is not included in subgroup analyses regarding cut-off in the meta-analysis.
Seven studies reported that they only included patients with first ever stroke (7, 29–31, 40, 49, 53), and 18 studies reported that the stroke diagnoses were confirmed with magnetic resonance imaging (MRI) or computed tomography (CT) brain imaging (14, 26, 27, 30, 31, 34, 35, 37, 38, 40, 42, 45, 50, 52, 55, 56, 58, 59). Two studies asked the patients if they had any previous history of mood disorders and one of them excluded patients if they had any related medication (27). Fifteen studies excluded patients with cognitive impairment (14, 26, 30–32, 34, 37, 41, 45, 49, 52, 54–56, 59) and 17 excluded those with aphasia (14, 30, 31, 34, 35, 37–41, 43, 45, 50, 53–56). Four studies excluded those with subarachnoid haemorrhage (SAH) (14, 28, 41, 55) and 5 those with TIA (14, 26, 31, 40, 41).
Quality assessment of the included studies is summarized in Table I. Most of the studies (65%) were of medium quality. The most common reason for not being categorized as having high quality was not using consecutive samples, not reported if the assessments were validated, and having a high loss to follow-up rate. Those of high quality made a consecutive selection, used standardized assessment, which was reliable and validated, had no reporting bias or reported no bias of interest.
The overall pooled prevalence of anxiety disorders in this review showed that anxiety was present in 29.3% ((95% CI 25.1–33. 5%), (I2 = 97%, p < 0.00001)) of stroke survivors at any time during the first year after stroke. Pooling only those studies using HADS-A showed that anxiety is present in 27.4% ((95% CI 22.5–32.3%) (I2 = 97%, p < 0.00001)) (Fig. 2) at any time during the first year after stroke. There was a statistically high heterogeneity in this estimate (I2 = 97%, p < 0.00001). The Eggers regression asymmetry test confirms the heterogeneity (b1=1.4), but it was not significant (p = 0.2). One study was judged to be of low quality (38) and if excluded from the analysis the pooling of HADS-A showed that anxiety was present in 28.1% ((95% CI 23.9–32.3%) (I2 = 98%, p < 0.00001)). The pooled anxiety in hospital settings was 29.5% ((95% CI 19.7–20.8%) (I2 = 90%), p < 0.00001)). In rehabilitation-based and community-based settings anxiety incidence was 18.4% ((95% CI 13.9–22.8%) (I2 = 79%, p = 0.03)) and 18.9% ((95% CI 17.5–20.5%) (I2 = 87%, p < 0.00001)), respectively, and in population-based settings 37% (95% CI 21–53%). The majority of the studies using HADS-A used a cut-off ≥8 to define possible anxiety (7, 14, 27–30, 32, 34, 36, 38, 40–42, 46, 48–52, 55–59). Those studies reported a higher prevalence rate (29%) relative to those using a lower, ≥ 6 (23%), or higher, ≥ 11 (19.4%) (I2 = 88%, p < 0.00001), cut-off. Subgroups analyses of the prevalence over different time showed a non-significance decrease between the acute phase and the phase 2 weeks to 3 months post-stroke (Fig. 3). The frequency 0–2 weeks post-stroke was 32.3% ((95% CI 22–42.5%) (I2 = 90%, p < 0.00001)), 2 weeks to 3 months post-stroke 24.1% ((95% CI 16.7–31.4%) (I2 = 98%, p < 0.00001)) and 3–12 months post-stroke 23.8% ((95% CI 12.9–34.7) (I2 = 96%, p < 0.00001)). Excluding the study with low quality (38) from the subgroup analysis showed no difference in the analyses regarding cut-off or settings, but in the analyses of time post-stroke it showed that the frequency in the group assessed 3–12 months post-stroke was decreased to 20.9% (11.1–20.9), and that there was still a significant high heterogeneity, but not so high (I2 = 79%, p < 0.00001).
Fig. 2. Prevalence of anxiety disorders and symptoms after stroke.
Fig. 3. Prevalence of anxiety depending on when assessed post-stroke. SE: standard error.
A total of 37 studies were found, involving 13,756 patients, that examined anxiety prevalence across all settings and found that anxiety disorders were present in 29.3% of stroke patients during the first year after stroke. Anxiety was particularly high in the hospital settings, 29.5% and when assessed up to 2 weeks post-stroke, 36.7%. Our overall estimate is that at least 1 in 3 have any anxiety disorder. This shows an increased prevalence compared with earlier review (10). Our study shows a small increased prevalence of anxiety over time, but the increase is not statistically significant.
There was insufficient information regarding whether the anxiety reported was a consequence of stroke or if there was any presence of anxiety history pre-stroke, since only 3 studies reported asking about any history of anxiety disorders (27, 45, 48). Neither have we taken into account whether the studies included patients only with the first stroke or also included patients with recurrent stroke. This may have influenced our results, giving an impression that the anxiety was a result of the current stroke disorder.
There was a significant heterogeneity in the pooled data, thus we stratified the analysis in different subgroups analyses by settings, time post-stroke and the cut-off value of HADS-A. The regression analyses confirmed this heterogeneity. This is probably a result of articles with a very small sample size also having a high prevalence of anxiety.
The main purpose of the majority of the studies was to measure depression, but since HADS is a combined assessment measuring both depression and anxiety, those studies also reported anxiety. This confirms that depressive disorders receive most clinical attention. This is not so strange given that anxiety as a syndrome in the medical literature one of the newest subjects (61). Studies have found that anxiety is highly related and comorbid with depression (46, 62–64). Anxiety could be one of the predictors of depression (65). Considering this, and that anxiety after stroke is as prevalent in 1 in 3 in this study, management of anxiety could be helpful into preventing depression after stroke. Anxiety also significantly influences the quality of daily life (48, 66). These are 2 strong contributing reasons patients should be screened for anxiety disorders post-stroke.
The majority of the studies assessing anxiety with HADS-A used a cut-off of ≥ 8 to define possible anxiety and those reported a prevalence of 29%. Only one study used a cut-off ≥ 6 and they reported a lower prevalence (23%) (39). It has been suggested that a score of 4 or 5 should be an optimal cut-off when screening for anxiety (67). In that case, the studies in our review have probably underestimated the prevalence of anxiety disorders, which means that anxiety is probably more common than we currently believe.
The limitations of the quality of the studies in this review of course affect the results. Many studies are small, n < 50, and the studies are very different in the types of settings of stroke survivors. Besides using different scale for discovering anxiety, those using the same scale used different ways of assessment. Some had a blinded research assistant who administrated and guided in the assessment process, while some studies just sent the assessment home to the patient, without any guidance. Some studies did not state in what way they administered the assessment scale.
The included studies came from countries all over the world and not all of them have reported if HADS-A were validity tested for the language in which it was administered. Despite the above limitations, the pooled frequency of anxiety during the first year after stroke reported in the present review conforms to several major earlier reviews (10). The included patients in the studies came from different settings, which of course can affect the experience of anxiety. We found that those from acute settings in hospital and those ≤ 2 weeks post-stroke estimated more anxiety compared with those from rehabilitation settings more in a post-acute stage. The anxiety decreased assessed 2 weeks to 3 months post-stroke, but compared with 3 months to 1 year post-stroke there were no differences. According to the Swedish Stroke Register (68) approximately 40% of the Swedish stroke patients experienced inadequate help and support from healthcare 3 months after the onset, and, if we apply that to the participants in this review, which can be an explanation for our results. People who experience anxiety up to 3 months post-stroke and receive inadequate help may have a continued experience of anxiety 1 year post-stroke. Patients from population-based settings reported nearly twice as high levels of anxiety compared with those from hospital, rehabilitation and community-based settings. In addition, here one may suspect that the help and support from healthcare has decreased or ended, and that the patients therefore feel more alone and experience more anxiety.
Anxiety is common during the first year post-stroke, with 1 in 3 subjects experiencing it. Since anxiety significantly influences quality of life, is prevalent, and could be a predictor for depression (65), clinicians should be more aware of the condition. It may be worth considering further routine screening post-stroke, in order to provide appropriate interventions.
The authors would like to thank Ann Liljegren (ann.liljegren@vgregion.se) for providing original data. Thanks also go to Dr Kate Bramley-Moore for editing assistance.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize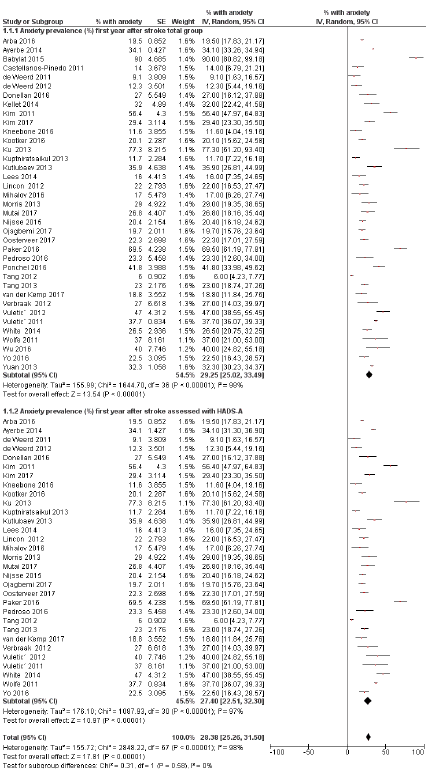 Click to show fullsize
Click to show fullsize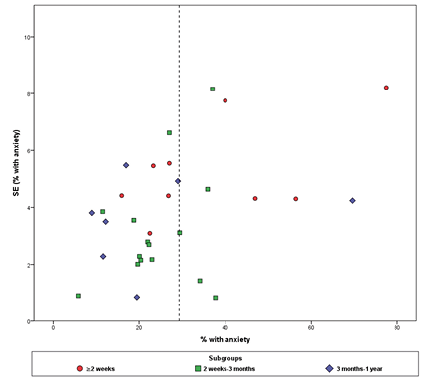 Click to show fullsize
Click to show fullsize