
From the Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
#These authors contributed equally to this work.
Objectives: To investigate the effectiveness of contra-laterally controlled functional
electrical stimulation (CCFES) on the recovery of active wrist dorsiflexion and upper limb function in patients with early-phase stroke (<15 days post-stroke).
Methods: Patients in the CCFES group were treated with routine rehabilitation combined with CCFES, while those in the conventional neuromuscular electrical stimulation (NMES) group were treated with routine rehabilitation combined with NMES. Time intervals from stroke onset to appearance of wrist dorsiflexion, and from onset of treatment to appearance of wrist dorsiflexion were recorded (in days). Functional assessments were also performed at baseline and endpoint.
Results: Nineteen out of 21 patients in the CCFES group and 12 out of 20 patients in the NMES group regained active wrist dorsiflexion during the treatment and follow-up period (90.5% vs 60%, p = 0.025). The mean time interval from onset of treatment to appearance of active wrist dorsiflexion was signifcantly shorter in the CCFES group than in the NMES
group (p < 0.001). The CCFES group had signifcantly higher scores for upper extremity
function (p = 0.001), strength of extensor carpi (p = 0.002), active ROM for wrist dorsiflexion (p = 0.003), activities of daily living score (p = 0.023) and ICF score (p < 0.001) than the NMES group at the endpoint.
Conclusion: CCFES signifcantly shortened the time for regaining wrist dorsiflexion, and improved the upper extremity function and general health of patients with early-phase stroke. CCFES therefore has potential as a clinical intervention.
Key words: stroke; contralaterally controlled functional electrical stimulation; neuromuscular electrical stimulation; wrist dorsiflexion; early-phase rehabilitation.
Accepted Nov 16, 2018; Epub ahead of print Jan 22, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Xiao Lu, Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. E-mail: luxiao1972@163.com
After a stroke, it is essential that recovery of function of the upper limb is maximized in order to enable activities of daily living. The hand plays an important role in the function of the upper limb. This study examined the effectiveness of contralaterally controlled functional electrical stimulation (CCFES) on recovery of active dorsiflexion of the wrist and upper limb functioning in patients in the early-phase after stroke (<15 days post-stroke). CCFES significantly shortened the time for regaining wrist dorsiflexion, and improved the upper extremity function and general health of patients with early-phase stroke, compared with conventional neuro-muscular electrical stimulation. CCFES therefore has potential as a clinical intervention.
Stroke is a leading cause of disability with high morbidity and mortality. Approximately 75% of patients with stroke have upper extremity dysfunction (1). Impaired motor function of the upper extremity is a major factor in preventing patients returning to their usual activities. In addition to routine medical treatment, early-phase rehabilitation helps improve motor function and activities of daily living (ADL) (2). Moreover, well-prescribed rehabilitation may shorten the course of recovery from stroke, help patients return to the community earlier, improve their quality of life, and reduce the cost of medication (3).
Recovery of upper extremity functioning is essential for improving ADL ability in patients with stroke (4). The hands play an important role in functioning of the upper extremities. Hand function and, in particular, extensor function, is difficult to recover once impaired, Therefore, specific rehabilitation interventions, which are considered the first step in re-gaining full extension of the hand, are essential in the recovery of wrist dorsiflexion (WD). Early recovery of active WD contributes not only to a better outcome for upper extremity functioning, but also to improved outcome for ADL.
Over the past decades, neuromuscular electrical stimulation (NMES), an electrical stimulation that provides passive training for the wrist dorsi-extensor, has been integrated into certain specific rehabilitation prescriptions (5–7). NMES triggers the movement using electrical stimulation. The frequency and amplitude of biphasic rectangular current pulses are pre-set and fixed during the whole training course.
In contrast, controlled functional electrical stimulation (CCFES) is an intervention technique developed recently to improve the function of the paretic upper extremity after stroke. One of the characteristics of CCFES is that it requires active participation from patients, and not merely electrical stimulation of the paretic muscle or extremity. As described by Knutson et al., “CCFES uses a control signal from the non-paretic side of the body to regulate the intensity of electrical stimulation delivered to the paretic muscles of the homologous limb on the opposite side of the body” (8). In separate studies, Knutson et al. (9) and Shen et al. (10) compared the effectiveness of CCFES and NMES in patients with sub-acute stoke, and found greater improvements with CCFES. Nonetheless, its effectiveness in the early-phase (i.e. within 15 days) after stroke is unclear. The aim of this study was therefore to investigate the effectiveness of CCFES compared with NMES on upper extremity function, particularly WD, in patients with early-phase stroke.
Patients admitted to the Department of Neurology, Jiangsu Province People’s Hospital, Nanjing, China, between March and September 2015 were recruited to this study. All subjects provided written informed consent prior to the study, and the ethics committee of the First Affiliated Hospital of Nanjing Medical University approved the study protocol.
Inclusion criteria were: (i) diagnosed with stroke using computed tomography (CT) or magnetic resonance imaging (MRI); (ii) stable vital signs 48 h post-stroke; (iii) single-side injury; (iv) age 20–80 years; (v) within 15 days post-stroke; (vi) Brunnstrom recovery stage of III or less; (vii) score of Fugl-Meyer assessment (FMA) for upper extremity ≤ 22; and (viii) no active WD detected.
Exclusion criteria were: (i) progressive stroke with non-stable condition; (ii) stroke-like symptoms due to subdural haematoma, tumour, encephalitis or trauma; (iii) unable to follow treatment instructions due to severe cognitive and communication deficiency; (iv) implanted with a pacemaker; and (v) no informed consent (11).
Patients were assigned to either the NMES or the CCFES group based on a computer-generated randomization list and allocation (1:1) concealed by consecutively numbered, sealed opaque envelopes. An envelope was opened once a patient had consented to participate in the trial, the administrator then informed the doctor about the allocated intervention regimen via phone calls.
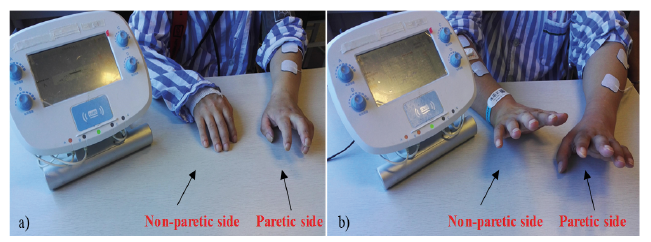
In the NMES group, 2 stimulating electrodes (4 × 4 cm) were placed at the motor points of the forearm extensor muscles (specifically the ulnar margin of the extensor aspect of the forearm) to produce WD (Fig. 1a). The stimulators (Weisi Corporation, Nanjing, China) used in this study delivered biphasic rectangular current pulses; the pulse frequency was set at 35 Hz, and the pulse amplitude was set at 40 mA. The electrical stimulation intensity was set at a sustainable level with full balanced WD with tetanic contraction.
In the CCFES group, 3 recording electrodes (4 × 4 cm) were placed on the motor points of the forearm extensor muscles (the ulnar margin of the extensor aspect of the forearm) on the non-paretic side, while 2 stimulating electrodes (4 × 4 cm) were attached on the paretic side (Fig 1b). For each patient, the intensity of the electrical stimulation to WD of the paretic side was determined by the strength of contralateral forearm extensor muscles contraction. Subjects were asked to voluntarily extend their unaffected wrist to 10% of ROM or less and maintain that position without moving. The electromyography value of the movement was then recorded. Meanwhile, the therapist adjusted the electric intensity until the same degree of movement appeared on the paretic side. The intensity value was then recorded. The same practice and recording process was also applied, with the patients extending their unaffected wrist to 50% and 100% of ROM. The electrical stimulation intensity that produced balanced WD was determined empirically for each patient and programmed into the stimulator.
Fig. 1. Patients treated with different strategies. (a) The patient underwent neuromuscular electrical stimulation (NMES) with the stimulator in Model I; (b) the patient underwent contralaterally controlled functional electrical stimulation (CCFES) with the stimulator in Model II.
The design and application of the stimulator was consistent with the protocol reported by Knutson et al. (9). The stimulator issued sound and light cues to inform the CCFES participants when and for how long to attempt to perform WD. For the NMES group, the stimulator was programmed to automatically and repetitively ramp the pulse durations from minimum to maximum in 1 s, maintain the stimulation at maximum for several seconds, and then ramp down the stimulation in 1 s, repeating this cycle at a rate that matched the sound and light cue timing in the NMES group.
Eligible patients were randomly assigned to either the NMES group or the CCFES group. Both groups received routine rehabilitation (mainly proprioceptive neuromuscular facilitation for 30 min/day) for the upper and lower extremities for 5 days over a period of 2 weeks.
In addition to routine rehabilitation, patients in the NMES group received neuromuscular electrical stimulation (2 20-min sessions each day). Each session consisted of 48 15-s sets, separated by 10 s of rest. The forearm extensor muscles were stimulated by the NMES instrument to complete WD without the patients’ active participation.
Patients in the CCFES group were treated with contralaterally controlled functional electrical stimulation (two 20-min sessions every day) combined with routine rehabilitation. Each session consisted of 48 15-s sets, separated by 10 s of rest. Patients were prompted by sound cues from the stimulator to actively extend both wrists, then the paretic wrist was stimulated to complete WD, assisted by the bioelectrical signal transmitted from the non-paretic side, held still for 15 s when full WD was achieved, then relaxed for 10 s.
A therapist was responsible for follow-up of the appearance of WD and recorded the time intervals from the onset of stroke to the appearance of WD (in days) and from the onset of treatment to the appearance of WD (in days). All patients were followed up for 1 month after inpatient treatment. The appearance of WD (a minimal range of motion of 5°) indicated the first time of volitional WD, which was checked and reported by the therapists every morning, afternoon and evening during the inpatient treatment period. When the patients were discharged from the hospital, the appearance of WD was reported by patients during everyday training and activities (checked every morning, afternoon and evening) and confirmed by the corresponding therapists via phone, and videos recorded by family members.
The functional assessments were performed both at baseline (before 2 weeks of training) and at endpoint (after 2 weeks of training), including active ROM for WD measured with a goniometer (range 0–45°), strength of the extensor carpi measured with Manual Muscle Testing (range 0–5), upper extremity impairment measured with Fugl-Meyer assessment (FMA) (range 0–66, presented as absolute scores: 0, cannot perform; 1, perform partially; and 2, perform fully, with higher score indicating better upper extremity function) (9, 12, 13); hand function measured with Jebsen Hand Function Test (JHFT) (ranged 0–7 and presented as number of missions completed: with more completed items indicating better function) (14), and ADL measured with Modified Barthel Index (mBI) (range 0–100 and presented as absolute score: 0 and 100, with higher scores indicating greater independence) (15). In addition, the ICF Generic Set was used to evaluate patients’ general health (range 0–10 and presented with absolute scores: 0 and 10, with lower scores indicating better general health) (16).
Demographic data for the patients, including age, sex, stroke classification and course of disease, in both groups were compared using Student’s t-test and χ2 test. Data on active ROM for WD, strength of extensor carpi and JHFT were not normally distributed; therefore non-parametric methods (Wilcoxon-rank sum test) were applied to test for inter-group differences. Student’s t-test was applied for testing the normally distributed data including time intervals (from the onset of stroke to the appearance of WD and from the onset of treatment to the appearance of WD), FMA for upper extremity, mBI and ICF Generic Set. All statistical analyses were performed using SPSS 20.0 (IBM Corp, USA). p < 0.05 was considered statistically significant.
The study was powered based on data from Knutson et al. (9) to detect differences in upper extremity FMA mean scores of 46.2 (standard deviation (SD) 2.1) in the CCFES group vs 41.1 (SD 2.2) in the NMES group at a significance level of 0.05 (10). A minimum of 4 participants per group was required in order to detect differences between groups with a power of 90%. In order to power the current study, the sample size was increased to 20 in each group, with a total of 40 participants.
Based on the inclusion and exclusion criteria, 50 patients with early-stage stroke were eligible to join the study, and were randomly assigned to the CCFES group (n = 25) and the NMES group (n = 25). Nine out of the total of 50 dropped out due to secondary cerebral haemorrhage (1 in the CCFES group and 2 in the NMES group), compressive lumbar vertebrae bone fracture after falling off a bed (1 in the CCFES group), secondary cerebral infarction (1 in the CCFES group and 2 in the NMES group), serious pulmonary infection (1 in the CCFES group and 1 in the NMES group). At the endpoint, 41 patients completed the study (21 in the CCFES group and 20 in the NMES group) (Fig. 2). No statistical difference was detected between experimental groups in terms of the demographic data (Table I).
Fig. 2. Study flow diagram. CCFES: contralaterally controlled functional electrical stimulation; NMES: neuromuscular electrical stimulation.
Table I. Demographic data of study sample
At the endpoint, 19 patients in the CCFES group and 12 in the NMES group had re-gained active WD. The mean time interval from onset of stroke to appearance of WD was 18.33 days (SD 7.01) for patients in the CCFES group, which was approximately 23 days earlier than for NMES group (Table II). In addition, a statistical difference was detected between groups in terms of mean time interval from onset of treatment to appearance of WD (10.48 (SD 5.46) days in the CCFES group vs 31.90 (SD 22.44) days in the NMES group, p < 0.001).
Table II. Summary of the appearance of wrist dorsiflexion (WD) between groups
Statistical differences were observed in terms of the FMA score of upper extremity (mean 29.6 (SD 26.34) in the CCFES group vs 22.65 (SD 5.67) in the NMES group, p = 0.001), strength of the extensor carpi (mean 2.29 (SD 0.78) in the CCFES group vs 1.20 (SD 1.06) in the NMES group, p = 0.002), active ROM of WD (mean 14.76 (SD 13.81) in the CCFES group vs 6.15 (SD 8.23) in the NMES group, p = 0.003), ADL score (mean 66.67 (SD 10.99) in the CCFES group vs 58.25 (SD 11.73) in the NMES group, p = 0.023), and ICF score (mean 13.05 (SD 3.06) in the CCFES group vs 17.10 (SD 1.12) in the NMES group, p < 0.001) between the 2 experimental groups after 2 weeks of intervention. Moreover, changes between baseline and endpoint for each parameter were significantly greater in the CCFES group compared with the NMES group (Table III).
Table III. Inter-group comparisons at baseline and endpoint
This randomized controlled trial (RCT) compared the effectiveness of CCFES and NMES in patients with early-phase stroke. Patients in the CCFES group regained WD earlier than those in the NMES group, and experienced better improvement in function of the upper extremity, better ADL and general health.
Over the past decades, early-phase rehabilitation for stroke has been developed around the world. Rehabilitation is prescribed once the patient’s vital signs are stable, and can significantly improve outcomes for patients. Several studies have reported that early-phase stroke rehabilitation may help to reduce the mortality and incidence of disability, improve the function of the body and quality of life and reduce medical costs (9, 17, 18).
Previously, rehabilitation for patients with stroke has focused mainly on training the proximal extremity. However, this can lead to disuse of the hand and forearm, and complications may also occur (e.g. shoulder-hand syndrome and dysmyotonia). Recovery of WD and finger extension are the most difficult aspects of hemiplegia treatment. Moreover, WD plays an important role in grip func-tion and it has been reported that WD deficiency is positively related to dysfunction of the hand (19, 20). Therefore, it is essential to involve the patients in the rehabilitation programme.
As a conventional physical therapy, NMES has been applied in stroke rehabilitation for a long time. It involves low- to moderate-frequency electrical stimulation of the paretic muscles and targets recovery of the function of nerve conduction, and is helpful in re-gaining motor function. Koyama et al. reported that NMES can improve the function of the upper extremity in patients with stroke (21).
Recently, CCFES has been developed as an active training, involving repetitive stimulation of peripheral neural activity, with bilateral symmetrical movement on the non-paretic side, to produce symmetrical and near-simultaneous movement of the paretic side. The patients control the timing and degree of WD in a way that does not interfere with the fluidity of task practice, making it more conducive to complete task-oriented functional hand activities (9, 10, 17). The effectiveness of CCFES was investigated in a RCT study conducted by Knutson et al. in 2016 (17). They randomized 80 patients with chronic stroke (> 6 months) into a CCFES group or an NMES group and found the 12 weeks of CCFES therapy improved manual dexterity more than an equivalent dose of NMES (17). Furthermore, Shen et al. compared the effectiveness of CCFES and NMES on patients and found that CCFES was better than NMES in the improvement of upper extremity function (9); however, it was only tested in patients with sub-acute stroke, not early-phase stroke.
The current study investigated the effectiveness of CCFES compared with NMES in patients with early-phase stroke. Although patients in both groups experienced improvement in each individual measurement, the CCFES group showed better outcome. Within the treatment and follow-up period, 19 patients in the CCFES group re-gained WD compared with 12 patients in the NMES group. In addition, the time intervals from the onset of stroke and the onset of treatment to the appearance of WD were significantly shorter in the CCFES group than in the NMES group. Therefore, CCFES may be more effective and efficient in the improvement of hand function than NMES. For the FMA scores, the level of motor dysfunction was reduced from very severe to severe in the NMES group (22). Although the same situation was observed in the CCFES group, it scored a mean of 7 higher, indicating that better upper limb function was obtained compared with the NMES group. This is not surprising, because this assessment captures the most fundamental level of upper extremity function and is therefore expected to be impacted largely by the timing of WD appearance. Muscle strength was improved from 0 to 1.20 ± 1.06 in the NMES group and from 0 to 2.29 ± 0.78 in the CCFES group; the improvement with NMES was limited for task-oriented movement, while CCFES allows partial actions of the hand when the effect of gravity is eliminated (23). At the endpoint, active ROM of the WD (mean 14.76 (SD 13.81)) in the CCFES group was approximately 15°, which is considered the lower threshold for basic hand movements, while the improvement in the NMES group was limited (24). The outcome of JHFT also indicated better hand activity in the CCFES group than in the NMES group, which indicated better hand function with CCFES. For ADL measurement, patients in the CCFES group (mean 66.67 (SD 10.99)) could be classified as “Moderate Dependence” after 2 weeks treatment according to the criteria of mBI, while those in the NMES group (mean 58.25 (SD 11.73)) were classified as “Severe Dependence” (15). This also demonstrated better ADL ability in the CCFES group and could be considered clinically important by patients and clinicians. Patients’ general health was measured with the ICF Generic Set (25) and greater improvement was observed in the CCFES group. Although the mechanism of the improved upper-limb function in the CCFES group remains unclear, the possible explanation may be that linking movement of the paretic side to the less-affected side increased the corticospinal excitability of the stimulated muscles by interhemispheric disinhibition, intracortical facilitation. In addition, the short length of inpatient rehabilitation in China requires patients to perform more self-administered training at home with less assistance from a therapist. This indicates that CCFES may be a promising intervention with superior effectiveness compared with NMES, since it further addresses the current clinical needs of patients with early-phase stroke in China.
The major limitation of the current study was the relatively small sample size, which may cause bias when the findings are applied to specific patients with impaired upper extremity. This limitation could be overcome by enrollment of more patients. Moreover, the study focused only on the observation of the outcome reflected by different scales after 2 specific interventions (CCFES vs NMES), the real recovery mechanism might be better understood using functional magnetic resonance imaging (fMRI) examinations of the brain at the baseline and endpoint. A further limitation was that there was no control group (without NMES and CCFES) in the current study, therefore it was difficult to identify whether the improvement was due to the specific interventions or the natural history of the disease. In addition, the appearance of WD was reported by the patients and their family members after the patients were discharged from hospital, which may lead to vulnerable and over- or under-estimated results, since the patients and their family members were not expected to be as precise as the medical staff. The current study was not powered to detect changes in the time to regain WD within the 2-week treatment; however, this study provided estimates of the effect, which can be used to power future studies.
In conclusion treating patients with early-phase stroke at different levels. After 2 weeks of intervention, improvements at the structural and functional level, activity level and participation level were observed in terms of the active ROM, strength of extensor carpi, upper extremity function, hand function, ADL and general health. In addition, CCFES was superior to NMES in either shortening the course of regaining WD or the recovery of upper extremity function in patients with early-phase stroke.
The authors would like to thank several people who participated in this study or supported them. We acknowledge Ying Shen for her invaluable technical support. Zhifei Yin, Qiumin Zhou and Hong Hou are also acknowledged for their professional insights on the electrophysiological treatment of stroke.


 Click to show fullsize
Click to show fullsize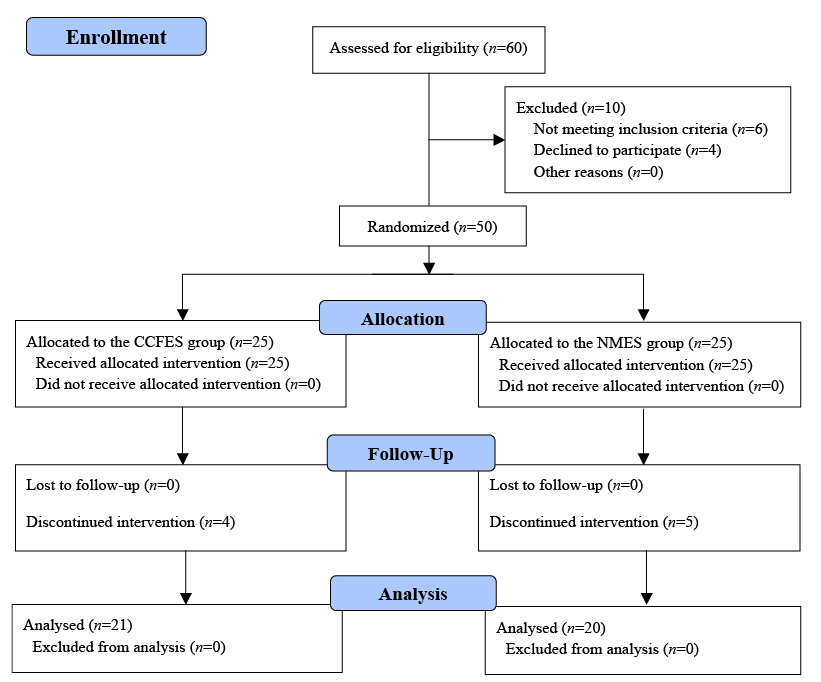 Click to show fullsize
Click to show fullsize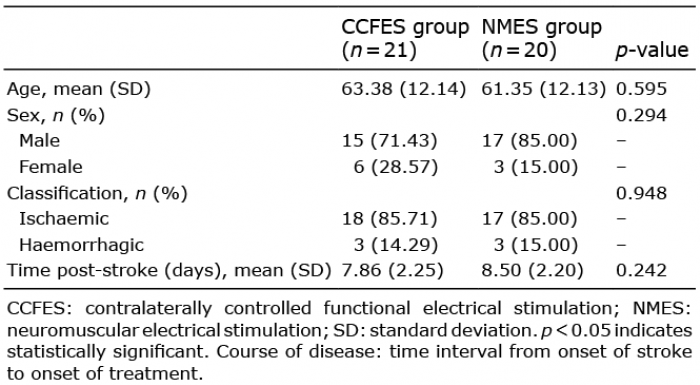 Click to show fullsize
Click to show fullsize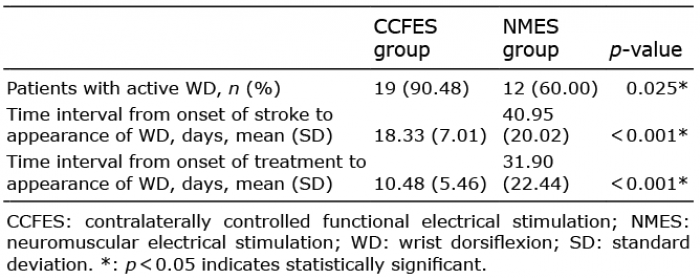 Click to show fullsize
Click to show fullsize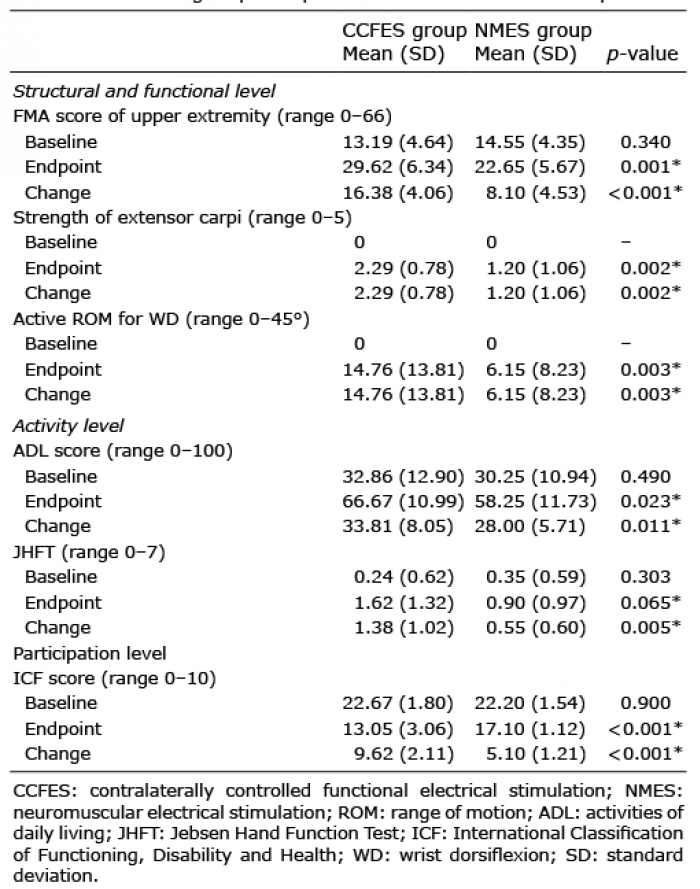 Click to show fullsize
Click to show fullsize