
From the 1Department of Rehabilitation and 2Department of Neurology, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, Nijmegen, The Netherlands
Objective: To investigate the functional effects of bilateral botulinum toxin A treatment and subsequent stretching of spastic hip adductors on gait and reactive lateral stepping responses in patients with pure hereditary spastic paraplegia.
Design: Explorative pre-post intervention study.
Patients: Twenty-five patients with pure hereditary spastic paraplegia.
Methods: Patients were treated with bilateral botulinum toxin A injections in the hip adductors and performed daily self-administered stretching exercises for 16 weeks. Before the intervention (T0), and 6 (T1) and 16 (T2) weeks thereafter, gait width, gait speed, and leg angles at first stepping-foot contact after lateral balance perturbations were assessed, as well as the corresponding success rates of reactive lateral steps.
Results: Compared with baseline, gait width increased by 12.6% and 9.7% and comfortable gait speed by 8.3% and 11.5% at T1 and T2, respectively. In known perturbation directions, leg angles increased by 5.9% at T1 and 8.0% at T2, while success rates increased from 70% at baseline to 90% at T1 and T2. No effects were found for maximal gait speed or lateral stepping responses in unknown perturbation directions.
Conclusion: Bilateral botulinum toxin A treatment and subsequent stretching of the hip adductors may improve gait and reactive lateral stepping in patients with pure hereditary spastic paraplegia.
Key words: hereditary spastic paraplegia; botulinum toxin; balance control; gait.
Accepted Mar 29, 2019; Epub ahead of print Apr 10, 2019
J Rehabil Med 2019; 00: 00–00
Correspondence address: Bas van Lith, Department of Rehabilitation, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, PO Box 9101, 6500 HB Nijmegen, The Netherlands. E-mail: Bas.vanLith@Radboudumc.nl
Patients with pure hereditary spastic paraplegia often have hip adductor spasticity, causing reduced gait width and a narrow base of support. In addition, they experience difficulties stepping sideways to recover from sideward balance perturbations. A small base of support and the presumed side-stepping difficulties probably increase their risk of falling. Botulinum toxin type A injections are commonly used to reduce spasticity in patients with hereditary spastic paraplegia, but no studies have systematically investigated the effects of botulinum toxin type A in (with subsequent stretching of) the hip adductors on gait and balance. The results of this study indicate that, after botulinum toxin type A administration, there is an increase in comfortable gait speed and gait width. Furthermore, patients show improved reactive stepping responses when the perturbation direction is known. It is concluded that botulinum toxin type A treatment and subsequent stretching of the hip adductors may improve gait and reactive lateral stepping in patients with pure hereditary spastic paraplegia.
Patients with pure hereditary spastic paraplegia (HSP) show a slow, retrograde axonal degeneration of the corticospinal tract, which leads to bilateral progressive lower extremity spasticity. Although muscle strength and somatosensation are often also affected, the degree of paresis and sensory loss is usually milder than in other conditions with spastic paraparesis (e.g. spinal cord injury or multiple sclerosis) (1, 2). Hip adductor spasticity is often prominently present in patients with pure HSP. Besides loss of gait propulsion and deterioration of balance in the plane of progression (1, 3), patients are usually also affected by frontal-plane imbalance, to which hip adductor spasticity is suggested to be an important contributing factor (4). This may be explained by spasticity of the hip adductors leading to forced, spontaneous narrowing of the base of support while standing and walking (“scissoring”). In addition, patients with HSP may experience difficulties stepping sideways to recover from lateral balance perturbations, as the hip abductors have to overcome the involuntary activity of the spastic hip adductors. The small base of support in combination with the presumed difficulties in side-stepping probably increase the risk of falling in patients with HSP.
Botulinum toxin type A (BTX-A) injections are commonly used for reducing spasticity in patients with HSP (2, 5–8), although BTX-A is still on off-label prescription in HSP for all commercially available toxins. BTX-A treatment of the hip adductors, calf muscles and hamstrings has been suggested to lead to functional improvements in balance and gait capacities (4, 5). However, despite the high prevalence of hip adductor spasticity in patients with HSP, there are no studies that have systematically investigated the effects of BTX-A injections in these muscles, either on clinical indicators of spasticity, or with respect to balance and gait capacity. In a few previous studies with limited numbers of patients with HSP, the hip adductors were injected in some of the participants (n = 5–12), yet often in combination with other muscle groups (i.e. calves, tibialis posterior, iliopsoas and rectus femoris) (6, 8, 9). Furthermore, these studies did not include stretching exercises following BTX-A treatment, as recommended by international consensus (10). Hence, the specific effects of BTX-A injections in the hip adductors with subsequent stretching exercises remain to be established.
This exploratory study focused on the effects of BTX-A injections in spastic hip adductors and subsequent stretching exercises in patients with pure HSP, using 2 primary outcomes: (i) gait width; and (ii) the quality of sideways reactive stepping responses following lateral balance perturbations. In addition, comfortable and fast gait speed, success rates of the lateral stepping responses, and various clinical (physical and functional) tests served as secondary outcome measures. The physiological effect of BTX-A usually reaches its maximum 6 weeks after the injections (11) and diminishes progressively until approximately 16 weeks after the injections. Therefore, we hypothesized that reduced hip adductor tone would translate into improvements in both gait width and lateral stepping at 6 weeks post-treatment, whereas a reduction in these effects was expected at 16 weeks after treatment.
Participants were recruited from all patients with HSP and hip adductor spasticity known at the expert centre for genetic movement disorders of the Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Center, Nijmegen, The Netherlands. In addition, active recruitment took place through the national patient organization “Spierziekten Nederland”. Inclusion criteria were: (i) a “pure” form of autosomal dominant HSP (either genetically proven, or based on family history); (ii) 18 years of age or older; (iii) bilateral hip adductor spasticity (Modified Ashworth Scale (MAS) score 1–4); (iv) balance- and/or gait-related activity limitations in daily life; (v) able to walk > 50 m independently with (adapted) shoes and/or orthoses (but without walking aids, such as crutches or a walker); and (vi) comfortable gait velocity > 0.4 m/s. Participants were excluded if they had any cognitive impairment, or they had any comorbidity affecting their gait capacity. In addition, the final BTX-A treatment of the hip adductors should have been administered longer than 6 months before the first measurement. Regular BTX-A treatments of other muscle groups should have been performed either within 3–4 weeks or longer than 4 months before the first measurement in order to have either an optimal or, otherwise, an absent effect of these prior injections during the study period.
For participants recruited at the outpatient departments, all inclusion criteria were checked by the attending physician. Participants who responded to the recruitment letters via the patient organization were interviewed by telephone by the primary investigator to check inclusion criteria i, ii and iv, whereas inclusion criteria ii, v and vi were checked by a physiotherapist at the first visit for the study. Out of 75 patients, 25 fulfilled the inclusion criteria and were included. Their demographic and clinical characteristics are listed in Table I.
Table I. Patient characteristics before the intervantion (T0)
All subjects gave their written informed consent prior to participation. The study was approved by the regional medical-ethics committee and conducted in accordance with the Declaration of Helsinki. Due to lack of prior research on gait width and quality of reactive sidesteps in patients with HSP, no formal power calculation could be performed. Given the exploratory nature of the current study, a required number of 25 patients seemed optimal, feasible and justified, and was agreed upon by the medical ethics committee.
Each participant was treated with bilateral BTX-A injections in the hip adductors by 1 of 3 rehabilitation physicians of our university hospital. A solution of 100 U Xeomin® (Botulinum toxin type A, Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany) per 5 ml saline 0.9% was used. A dose of 150 or 200 U per leg was injected, depending on the degree of hypertonia (Modified Ashworth Scale (MAS) 1: 150 U; MAS ≥ 2: 200 U). The BTX-A was distributed over the gracilis, adductor magnus and adductor longus muscles according to Table II. Muscle selection was based on muscle volume and its moment arm with respect to the hip joint. Thigh length was measured from the pubic bone to the medial femoral condyle and thigh length percentages were calculated from the pubic bone (see Fig. 1). All BTX-A injections were placed under ultrasound guidance.
Table II. Distribution of botulinum toxin per leg
Fig. 1. Schematic view of injection locations in percentages thigh length from the pubic bone to the medial femoral condyle. At the indicated thigh lengths, botulinum toxin (BTX) was injected into the adductor longus (L), adductor magnus (M) and gracilis (G).
During the 16-week study period, participants were instructed to perform stretching exercises of the hip adductors (with the hips both flexed and extended) for approximately 10 min, 3 times per day, and to log their exercises in a diary. The exercises were individually demonstrated and instructed by a physio-therapist at the day of the BTX-A injections until each participant was able to correctly perform the exercises independently.
Instrumented gait assessments. For instrumented gait assessment, the GAITRite system was used (CIR Systems, Inc., Sparta, NJ, USA), which is a 4.88-m long carpeted walkway that contains pressure sensors that detect the position of each footfall (12). Participants started at one end of the GAITRite and were instructed to walk 3 times across the walkway with (adapted) shoes and/or orthoses at their preferred speed. Subsequently, they walked 3 times across the walkway at their maximal speed without risking a fall. For each step, gait width was determined by the GAITRite system (and stored as “stride width”) and exported to Microsoft Excel. For each participant, the median gait width of all steps was calculated to avoid a disproportional influence of a single outlying step. Gait width was determined for both the preferred (primary outcome) and maximal gait speed. In addition, the mean preferred and mean maximal gait speed of the 3 trials was calculated.
Instrumented dynamic balance assessments. For instrumented dynamic balance assessments, the Radboud Falls Simulator was used (RFS). The RFS is a moveable platform (240 × 174 cm; BAAT, Enschede, The Netherlands (13)) that can translate in multiple directions. In this way, perturbations can be imposed that mimic natural situations. In this study, only sideways perturbations were used, where a leftward platform translation resulted in a rightward balance perturbation and vice versa. In the remainder of this text, we consistently refer to the direction of the balance perturbations.
At the start of each measurement, participants were instructed to sustain all perturbations by making a single lateral step without grabbing the handrails, while the perturbation direction was known to the participants. All participants wore a safety harness attached to the ceiling that prevented them from falling. In addition, a railing system was present at both sides that participants could grab in the case of a fall. At the first measurement (T0), participants were exposed to increasing perturbation intensities that started at 0.125 m/s2 and were increased by at least 0.125 m/s2 between trials. The maximum perturbation intensity that each participant could successfully sustain with a single step at least once out of 3 trials (without falling or grabbing the railing system) defined the individual limit of stability. To familiarize them with the test situation, during the subsequent measurements (T1 and T2), participants were again exposed to at least 15 incremental perturbation intensities until their individual limits of stability were reached.
During all measurements each participant was twice (randomly) exposed to 5 leftward and 5 rightward perturbations at their individual limits of stability. During the first 10 perturbations, the perturbation direction was known to the participant, whereas during the last 10 trials the perturbation direction was unknown. These 20 trials were used for statistical analysis.
During all balance assessments, kinematic data were recorded by an 8-camera 3D motion analysis system (Vicon Motion Systems, Oxford, UK) at a sample rate of 100 Hz. Reflective markers were placed at anatomical landmarks according to the full-body PlugInGait configuration (14). For all trials in which the participant succeeded to make a sidestep following the perturbation, the leg angle (primary outcome) was calculated at the instant of stepping-foot contact, as the body configuration at step contact appears to critically determine the successfulness of balance recovery responses (15). The leg angle was defined as the angle between the absolute vertical and a line connecting the mid-pelvis and the ankle marker of the stepping foot. The medians of the 5 right and 5 left leg angles were calculated to avoid a disproportional influence of a single outlying value. These medians were averaged for each person into a single leg angle score for the perturbations with known and unknown directions separately. Furthermore, the success rates of the lateral stepping responses were calculated for the perturbations with known and unknown directions separately. A trial was scored as successful if the participant maintained balance with a single sidestep.
Physical tests. Muscle strength of the hip adductors and hip abductors was assessed with the Medical Research Council (MRC) scale (0–5), with lower scores indicating more muscle weakness (16). Muscle tone of the hip adductors was assessed using the MAS (0–5), with higher scores indicating more hypertonia (17). Furthermore, passive range of motion (ROM) on hip abduction was measured using a goniometer. All outcomes were averaged for both sides into a single score.
Functional tests. Functional balance was assessed barefooted with the Berg Balance Scale (BBS, range 0–56) (18). The Timed Up and Go (TUG test) (19) was performed with (adapted) shoes and/or orthoses, but without other walking aids. Endurance was assessed with the 6-min Walk Test (6MWT) (20) during which all walking aids were allowed. Lastly, the Activities-specific Balance Confidence (ABC) scale (21) was obtained as a subjective measure of mobility and balance.
All outcome measurements were performed on the day of treatment prior to the injections (baseline; T0), 6 (± 1) weeks after treatment (T1), and 16 (± 1) weeks after treatment (T2). T1 was set at 6 weeks after treatment, because at this time-point the physiological effects of BTX-A on spasticity were expected to have reached a maximum (11). The effects of BTX-A were expected to diminish progressively until approximately 16 weeks after the injections. Hence, T2 was set at 16 weeks post-treatment to test the possible presence of a long-term effect of the combined treatment. The instrumented assessments were taken by the primary investigator. All other tests were assessed by an independent physiotherapist.
All instrumented (parametric) outcome measures were tested using repeated-measures analysis of variance (ANOVA). The primary outcomes gait width and sidestep leg angle were tested using time (T0 – T1 – T2) as within-subjects factor. For gait width and gait speed, also gait condition (preferred – maximal) was introduced as a within-subjects factor. Bonferroni corrected post-hoc tests were applied in the case of a significant main effect of time. All other (non-parametric) outcome measures (physical and functional tests) were analysed with a Friedman’s test using time (T0 – T1 – T2) as a within-subject factor. Wilcoxon’s tests were used for post-hoc comparisons in the case of a significant time effect. All statistical analyses were performed using IMB SPSS Statistics Version 22 for Windows. The α-level was set at 0.05 for all analyses, with no adjustment for multiple outcomes.
From the total of 25 patients included in the study, 3 patients were lost between the first (T0) and second measurements (T1): 1 patient experienced increasing shoulder complaints that were already present before the first visit. One patient was lost due to spontaneous severe back pain, which had also repeatedly occurred in the past. A third patient left the study due to personal circumstances. No other adverse events occurred during the study.
Table III summarizes the group results for all measurements. There was a significant time effect on gait width (F(2,42) = 6.143, p = 0.005). Gait width increased by 12.6% from baseline to T1 (p = 0.021), and this improvement persisted at T2 (9.7%; p = 0.022) (see Fig. 2a). There was no effect of gait condition on gait width (F(1,21) = 1.229, p = 0.280), nor was there a significant time × gait condition interaction (F(2,42) = 1.081, p = 0.349).
Table III. Outcomes measures
There was also a significant time effect on gait speed (F(2,42) = 5.458, p = 0.008) as well as a significant time × gait condition interaction (F(2,42) = 5.399, p = 0.008). Compared with baseline, the preferred gait speed had increased by 8.3% at T1 (p = 0.001) and by 11.5% at T2 (p < 0.001). In contrast, no significant changes from baseline were observed in the maximal gait speed (Fig. 2b).
Fig. 2. (a) Gait width and (b) gait speed at 3 measurements (T0, T1, T2) for preferred and maximal gait speed (gait condition). *Indicates significant post-hoc effects of time for gait width. #Indicates significant post-hoc effects of time on preferred gait speed.
Changes in leg angles across time could only be statistically tested if side steps were made at all measurements (T0–T2). As some participants failed to make any side steps (i.e. only made cross steps) or grabbed the railing system before stepping, a total of 19 participants could be included in the analysis of trials with known perturbation direction and 13 in the analysis of trials with unknown directions. The mean limit of stability was 2.135 m/s2 (range 0.375–4.375 m/s2).
For the known direction perturbations, the leg angle showed a main effect of time (F(2,36) = 12.053, p < 0.001). There was an increase of 5.9% in leg angle from baseline to T1 (p = 0.003), which persisted at T2 (8.0%; p = 0.001). In contrast, leg angle for the unknown direction perturbations did not show a significant effect of time (F(2,24) = 0.107, p = 0.899) (see Fig. 3a).
For the known direction perturbations, there was a significant effect of time on success rate (χ2(2) = 12.559, p = 0.002). Compared with the 70% success rate at baseline, participants were more successful at T1 (90%; p = 0.007), which result tended to persist at T2 (90%; p = 0.075). For the unknown direction perturbations, no significant effects of time were found (χ2(2) = 4.388, p = 0.111) (see Fig. 3b).
Fig. 3. (a) Leg angle and (b) success rate at 3 measurements (T0, T1, T2) for known and unknown perturbation directions. #Indicates significant post-hoc effects of time in known perturbation directions. *Indicates significant effect of time.
Hip adductor muscle tone showed a significant time effect (χ2(2) = 33.890, p < 0.001). The MAS scores decreased from baseline to T1 (p < 0.001), and subsequently increased from T1 to T2 (p = 0.001), although they did not reach the baseline values (T0 vs T2, p = 0.001). Hip adductor muscle strength also showed a significant effect of time (χ2) = 15.800, p < 0.001), as the MRC scores decreased from baseline to T1 (p = 0.005), and increased from T1 to T2 (p = 0.003) to baseline values (T0 vs T2, p = 0.480). Hip abductor muscle strength did not significantly differ between the 3 measurements (χ2(2) = 4.957, p = 0.084). Furthermore, there was a significant time effect on hip abduction ROM (F(2,42) = 31.613, p < 0.001), which increased from baseline to T1 (p < 0.001) and decreased from T1 to T2 (p = 0.001), although it was still above baseline values at T2 (T0 vs T2, p < 0.001).
Because the 6MWT was too demanding for 5 participants, the analysis was performed on the remaining 17 participants. This analysis showed no significant effect of time on the 6MWT (F(2,32) = 2.498, p = 0.098). Likewise, the BBS (χ2(2) = 4.031, p = 0.133), TUG (F(2,42) = 0.198, p = 0.821), and ABC scale (F(2,42) = 2.048, p = 0.142) also did not show significant time effects.
The aim of this study was to evaluate the effects of BTX-A treatment and subsequent stretching of the hip adductors on gait and balance capacities in patients with pure HSP. The results support our hypothesis that bilateral BTX-A injections in, and subsequent stretching of, the hip adductors improve both gait width and lateral stepping responses in known perturbation directions coinciding with reduced hip adductor tone 6 weeks after treatment compared with baseline. These functional effects were retained, although some recurrence of hip adductor muscle tone was found 10 weeks later. In addition, comfortable gait speed increased 6 weeks post-injections, which effect was even a little stronger after 16 weeks. In contrast, maximal gait speed and lateral stepping responses in unknown perturbation directions did not respond to the treatment, nor did other functional tests (BBS, TUG, 6MWT, ABC scale).
Besides a prolonged reduction in hip adductor muscle tone lasting up to 16 weeks after treatment, we observed a similar and substantial improvement in hip abduction ROM (on average 13.3°) and a temporary reduction of hip muscle strength (on average 1 point on the MRC scale, 6 weeks after treatment). These findings are in line with several previous studies (2, 3, 5, 6, 8, 9, 11). The mean improvement of muscle tone at 6 weeks post-injections was 1.5 point on the MAS, which can be considered substantial and clinically relevant (22). Interestingly, the observed temporary loss of muscle strength did not seem to have a detrimental effect on balance and gait capacities, since functional tasks improved (or remained stable) 6 weeks after treatment. This result is in agreement with a previous study from our group (2) and suggests that loss of muscle strength after BTX-A injections in spastic muscles is probably of relatively short duration and without noticeable functional disadvantage.
The observed improvement in gait width was, on average, 1.1 and 1.5 cm for comfortable and maximal walking speed, respectively, and was probably the direct result of reduced hip adductor tone and improved hip abduction ROM. Remarkably, this effect was found even though comfortable gait speed improved in parallel. It is conceivable that a higher gait speed might coincide with faster leg swing and, thus, aggravate velocity-dependent hip adductor spasticity, but this effect apparently did not occur. Instead, the reason why comfortable gait speed improved may be that reduced hip adductor tone allowed patients to make larger and/or faster steps. In a prior study of patients with spastic paraparesis of various origins, BTX-A injections in the hip adductors also led to increased gait velocity (23). In addition, previous studies of patients with HSP in which hip adductors were injected with BTX-A in combination with other muscle groups also showed increased gait speed (6, 8, 9). These findings have important clinical implications as reduced spontaneous gait speed is one of the most frequent problems reported by patients with HSP (24). Notably, maximal gait speed did not improve after treatment, which is in agreement with the notion that the hip adductors are not the key muscles for gait propulsion (25). Nevertheless, gait width during walking at maximal gait speed improved even more strongly than during comfortable walking, indicating the robustness of the treatment effects on widening the base of support while walking. The observed effect size for gait width in this study may seem small, but it constitutes a 10–15% increase compared with baseline. Hence, the observed increase in gait width of 1.1–1.5 cm may be clinically relevant in terms of improved frontal-plane balance, but this conclusion needs to be supported by future studies.
To our knowledge, the effects of bilateral BTX-A injections on reactive lateral stepping responses have not been investigated previously. In the present study, we only observed beneficial effects on stepping responses to perturbations in known directions. Interestingly, no improvements in stepping leg angle or success rate were observed upon perturbations in unknown directions. As hip adductor spasticity decreases, less muscle activity of the hip abductors is supposedly needed to make a lateral step. One explanation for the observed discrepancy between known and unknown perturbation direction may be that the individual maximal perturbation intensity at baseline was based on tests with a known perturbation direction. As a consequence, the perturbation intensities might have been too high for the participants following perturbations in unknown directions. This may also (partly) explain the much lower number of participants able to sustain perturbations with unknown compared with known directions. Another reason might be that reactive steps following unexpected perturbations are relatively strongly influenced by delayed postural responses that occur in patients with HSP (4, 26), because patients cannot compensate by an anticipatory “central set” if the direction is unknown. Nevertheless, the improved balance capacity following perturbations in known directions suggests that hip adductor spasticity indeed impairs the quality of lateral stepping responses and, thus, is a relevant treatment target from a frontal-plane balance perspective.
The fact that the beneficial effects on muscle tone, gait width, comfortable gait velocity, lateral balance persisted until 16 weeks after treatment seems to challenge the common opinion that the biological effects of BTX-A have worn off after this time interval. It may, therefore, be that the stretching component of the treatment protocol was responsible for the observed long-term effects.
A limitation of the present exploratory study in patients with HSP is the relatively small sample size and the lack of a control condition, while the rather stringent inclusion and exclusion criteria limit the generalizability of our findings. Nevertheless, this study provides indications for the beneficial effects of bilateral BTX-A injections in the adductor longus, adductor magnus and gracilis muscles and subsequent stretching of these muscles on gait width, comfortable gait speed, and reactive lateral stepping in known perturbation directions, whereas maximal gait speed, gait endurance, and clinical balance scores appear to be less responsive in these patients. Future research should preferably be multi-centred to increase the number of participants and use a randomized controlled design. Gait width and gait speed would be valuable and responsive outcome measures in such trials. The instrumented balance assessments used in the present study are, however, less suitable for multi-centre studies as they require further development of clinically affordable systems. Clinically applicable assessments to validly test the quality of (lateral) reactive stepping responses are therefore urgently needed. As HSP is a chronic and progressive condition, it would also be relevant to conduct longitudinal, comparative cohort studies to investigate whether repetitive cycles of BTX-A treatment of spastic hip adductors improve lifetime functional ambulation prognosis in these patients.
This investigation was supported by an unrestricted grant from Merz Pharmaceuticals.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize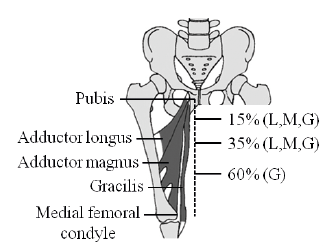 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize