
From the 1Vivantes Hospital Spandau, Berlin, Germany, 2Raymond-Poincaré Hospital, University of Versailles, Saint Quentin, Garches, France, 3Merz Pharmaceuticals GmbH and 4Formerly of Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany and 5Icahn School of Medicine at Mount Sinai, New York, New York, USA
Objective: The Titration study in lOWer and uppER-limb spasticity (TOWER) study (NCT01603459), evaluated incobotulinumtoxinA for upper- and lower-limb spasticity. This post hoc analysis assessed shoulder spasticity in patients who received injections into the shoulder.
Methods: Subjects received 3 injection cycles with escalating incobotulinumtoxinA doses on the same side (400, 600, 600–800 U; ≤ 600 U per limb including optional shoulder dose, planned range 100–250 U).
Joint function was assessed with the Ashworth
Scale shoulder sumscore (AS-SSS) in subjects treated
in the shoulder vs those who were not. Safety was assessed in subjects treated in the shoulder, and in those who had upper-limb treatment without
shoulder treatment.
Results: The proportion of subjects receiving shoulder treatment increased with escalating dose at each cycle (n = 84/140 (60.0%) by cycle 3; mean (standard deviation (SD)) shoulder dose 118.4 U (SD 60.2)). From baseline to 4-weeks post-injection, mean AS-SSS improved by –1.1 (SD 1.9), –1.7
(SD 1.8) and –1.7 (1.8) in cycles 1, 2 and 3,
respectively, in subjects treated in the shoulder, and –0.5 (SD 1.3), –0.8 (SD 1.6) and –0.9 (SD 1.4) in subjects who were not. A significant dose effect on AS-SSS was observed in cycle 3 (p = 0.0081). No
unexpected safety concerns were reported.
Conclusion: The results demonstrate an improvement in shoulder spasticity and safety following
incobotulinumtoxinA treatment.
Key words: incobotulinumtoxinA; botulinum neurotoxin type A; shoulder spasticity; upper-limb, lower-limb; stroke.
Accept Jan 20, 2020; Epub ahead of print Feb 26, 2020
J Rehabil Med 2020; 52: jrm00028
Correspondence address: Jörg Wissel, Department of Neurorehabilitation and Physical Therapy, Department of Neurology, Vivantes Hospital Spandau, Neue Bergstraße, 13585 Berlin, Germany. E-mail: Joerg.wissel@vivantes.de
After a stroke, many patients experience disabling spasticity of the limbs, characterized by stiffness and an inability to control the muscles. Spasticity in the shoulder muscles can lead to a limited range of motion and severe pain. The TOWER study looked at the use of incobotulinumtoxinA for upper- and lower-limb spasticity. The subsequent analysis of data from the TOWER study determined the effect of incobotulinumtoxinA for the treatment of spasticity in the shoulder muscles. The results showed that muscle tone in the shoulder muscles improved from baseline after treatment with incobotulinumtoxinA. No unexpected safety concerns were reported. Thus, incobotulinumtoxinA has potential as a treatment for patients who experience shoulder spasticity after a stroke.
Disabling spasticity of the limbs affects ~30% of individuals following a stroke (1). The shoulder joint is involved in all 5 typical combinations of patterns of
upper-limb post-stroke spasticity (2), which frequently affect internal rotation, extension and adduction of the shoulder (1, 2). Shoulder spasticity is associated with restriction of the range of motion in the joint, as well as spontaneous and stretch-related pain (1, 3).
Intramuscular injection of botulinum neurotoxin type A (BoNT-A) is recommended in European and North American guidelines for the treatment of focal and multifocal spasticity of the upper and lower limbs (4–7). The efficacy and safety of incobotulinumtoxinA (Xeomin®, Merz Pharmaceuticals GmbH) in subjects with upper-limb spasticity are well established (8–11). IncobotulinumtoxinA is approved for the treatment of upper-limb spasticity at total doses of up to 400 U in the USA (12), and up to 500 U in the European Union (EU) (13).
For the treatment of spasticity-related shoulder pain, a number of studies have confirmed the efficacy of BoNT-A (14–16). An exploratory analysis of subjects with post-stroke spasticity found greater, but not significant, reductions in shoulder pain 12 and 24 weeks post-injection vs placebo (both p > 0.05) (17). In another study, significant improvements in reported shoulder pain (p = 0.004), as well as range of motion, were documented 4 weeks post-injection for subjects with post-stroke spasticity (16).
However, there is limited evidence of the efficacy of BoNT-A specifically for the shoulder muscles in the management of upper-limb spasticity, as previous studies have included only small numbers of subjects (15, 18–22). In subjects with spastic hemiplegic shoulder following stroke or brain injury, BoNT-A treatment was associated with significant reductions in spasticity (p < 0.0001), and improvements in passive function (p = 0.002) and non-significant reductions in pain (p = 0.052) (18). Disability scores have also been shown to improve with BoNT-A compared with placebo (19).
The Titration study in lOWer and uppER-limb spasticity (TOWER) study (NCT01603459) assessed the safety and efficacy of escalating doses of incobotulinumtoxinA in adults with limb spasticity due to cerebral causes (11). This post hoc analysis was conducted to assess the safety and efficacy of inco-botulinumtoxinA for the relief of shoulder spasticity in sub-populations of subjects from the TOWER study.
Study design and participants
The TOWER study (NCT01603459) was a prospective, open-label, single-arm, multicenter, dose-titration study investigating the safety and efficacy of incobotulinumtoxinA. The methodology and pre-specified endpoints have been described previously (11). In brief, at the screening visit, investigators selected a target clinical pattern of spasticity to be treated in each cycle. For the selected target pattern, subjects had to have an Ashworth Scale (AS) (23) ≥ 2 and a Disability Assessment Scale (DAS) (24) score ≥ 2. Treatment comprised 3 injection cycles, in which escalating total body doses of incobotulinumtoxinA (400, 600 and 600−800 U) were administered via intramuscular injection in the same body side in accordance with the selected target clinical pattern of spasticity. The maximum dose per limb was 400 U in cycle 1, and up to 600 U in cycles 2 and 3. The intended dose range for treatment of the clinical pattern ‘internally rotated/extended/adducted shoulder’ was 100–250 U. An observation period of 12–16 weeks followed each treatment and included a follow-up 4-week post-injection visit in each injection cycle, and an end-of-study visit.
Subjects eligible to participate in the TOWER study were aged 18–80 years, with chronic upper- and lower-limb spasticity (defined as ≥ 12 weeks since the last event leading to spasticity) on the side of the body with the selected target clinical pattern, who were deemed by the investigator to require total body doses of up to 800 U incobotulinumtoxinA. Subjects were excluded if they had: spinal lesions of any origin in their medical history; neurological conditions associated with neuromuscular dysfunction, fixed contracture or muscle hypertonia other than spasticity in the joint associated with the target clinical pattern; previous or planned surgical treatment for spasticity in the target muscle(s); or severe atrophy of the muscles associated with the selected target clinical pattern.
This study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Good Clinical Practice Guidelines, and was approved by the Institutional Review Boards (IRBs) and/or Independent Ethics Committees at each investigational centre participating in the study.
Post hoc efficacy analysis
In this post hoc analysis, muscle tone increase on the treated body side was assessed using the AS shoulder sumscores (AS-SSS), following the principles of the summary rating scale for resistance to passive movement (REPAS) (25). AS assessments were performed for shoulder external rotation/flexion/abduction from the individual shoulder position of the subject (rather than from a neutral/null position). AS-SSS were then calculated from the sum of the AS scores for the 3 axes of movement, and expressed as a reduction in the respective dominant clinical pattern in the shoulder that are usually affected by shoulder spasticity (internal rotation, extension and adduction of the shoulder joint) (3) at the baseline and
4-week post-injection visit of each injection cycle. A reduction in score indicated a reduction in velocity-dependent muscle tone.
Post hoc safety analysis
Functional outcomes. Functional outcomes were analyzed to detect any improvement in upper-limb passive or active function post-treatment. Muscle function was also tested to detect any treatment-related weakness. The DAS was used to assess passive function at the baseline and 4-week post-injection visit of each injection cycle. Each subject and/or caregiver selected one of the 4 DAS domains (hygiene, dressing, limb position or pain) as their principal therapeutic target, and rated their level of functional impairment for each of the 4 domains on a 4-point scale ranging from 0 (no disability) to 3 (severe disability).
In addition, at each injection visit, subjects (supported by the healthcare teams) identified 2 personal, realistic goals per limb involved in spastic paresis. The extent to which a subject’s individual goals were achieved during the course of treatment was assessed using the Goal Attainment Scale (GAS) (26). The investigators rated the GAS score for each cycle at the next injection or the end-of-study visit, using a 5-point scale, ranging from −2 (a lot less than expected) to +2 (a lot better than expected).
Adverse events. The primary endpoint of the TOWER study was safety and has been reported previously (11). In this post hoc analysis, the incidences of adverse events (AEs) and serious AEs (SAEs) were assessed. In addition, the incidence of AEs in cycle 3 was assessed according to total incobotulinumtoxinA dose < 500 and ≥ 500 U administered in the upper limb. AEs of special interest that may indicate distant toxin spread were also evaluated.
Statistical analysis
Efficacy variables and functional outcomes were assessed in the full analysis set, defined as all subjects who received ≥ 1 injection of incobotulinumtoxinA. All efficacy variables were analyzed using descriptive summary statistics comparing subjects who were treated in the shoulder with those who were not treated in the shoulder. The change in AS-SSS was assessed using multiple regression analysis on shoulder dose and AS-SSS baseline value.
Safety was assessed in the safety analysis set, defined as all subjects who received ≥ 1 injection of incobotulinumtoxinA. AEs were summarized descriptively for each injection cycle, comparing subjects who were treated in the shoulder with those who had upper-limb treatment without shoulder treatment.
Subjects
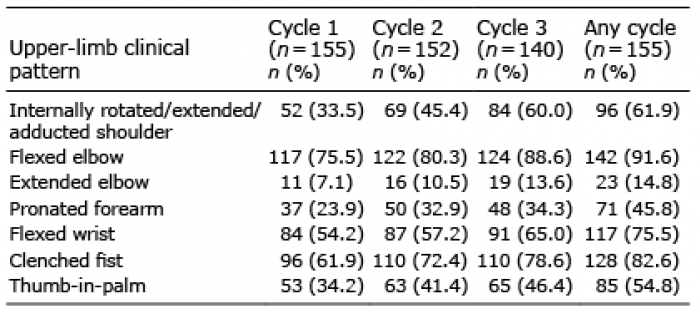
A total of 155 subjects (mean age, 53.7 years; 67.1% male) participated in the TOWER study (11). Of these, 52 were treated in the shoulder in cycle 1, while the remaining 103 subjects had upper-limb spasticity, but were not treated in shoulder muscles. The proportion of subjects who were treated in shoulder muscles increased at each injection cycle (with the option of increased dose per session) from 33.5% (52/155) in cycle 1, to 45.4% (69/152) in cycle 2, and to 60.0% (84/140) in cycle 3 (Table I). The most frequently treated shoulder muscle was the pectoralis major (Table II). The mean (standard deviation (SD)) doses of incobotulinumtoxinA used to treat shoulder muscles generally increased at each injection cycle (Table II). Doses of ≥ 500 U
were administered in 18 and 51 subjects treated in shoulder muscles in cycles 2 and 3, respectively, and in 4 and 20 subjects not treated in shoulder muscles in cycles 2 and 3, respectively (total body doses in cycles 2 and 3 were 600 and 600−800 U, respectively).
Table I. Proportion of subjects treated with incobotulinumtoxinA per upper-limb clinical pattern
Table II. IncobotulinumtoxinA dosing of the clinical pattern ‘internally rotated/extended/adducted shoulder’ and individual muscles: mean total doses and permitted dose ranges at each injection cycle
Post hoc efficacy analysis
Mean AS-SSS improved from baseline to the 4-week post-injection visit in each injection cycle for those subjects treated in shoulder muscles (cycle 1: 6.3 (SD 1.9) to 5.3 (SD 2.2); cycle 2: 6.2 (SD 2.3) to 4.4 (SD 2.3); cycle 3: 5.8 (SD 2.2) to 4.2 (SD 2.3)). The mean change from baseline to the 4-week post-injection visit of each injection cycle was: cycle 1: –1.1 (SD 1.9);
cycle 2: –1.7 (SD 1.8); and cycle 3: –1.7 (SD 1.8)
(Fig. 1 and Table III).
Fig. 1. Mean Ashworth Scale shoulder sum score (AS-SSS) change from baseline to the 4-week post-injection visit of each injection cycle according to whether subjects were, or were not, treated with incobotulinumtoxinA in the shoulder. n: number of subjects assessed; SD: standard deviation.
Table III. Mean changes from baseline to the 4-week post-injection visit for each injection cycle in AS-SSS and AS for subjects treated in the shoulder and those not treated in the shoulder with incobotulinumtoxinA
Mean AS-SSS at baseline and the 4-week post-injection visit in each injection cycle for those subjects not treated in spastic shoulder muscles was: cycle 1: 4.5 (SD 2.5) to 4.0 (SD 2.3); cycle 2: 4.5 (SD 2.4) to 3.7 (SD 2.6); and cycle 3: 3.7 (SD 2.4) to 2.8 (SD 2.2). The mean AS-SSS for these non-treated subjects was lower at each baseline visit compared with the scores for treated subjects. The mean change from baseline to the 4-week post-injection visit of each injection cycle was: cycle 1: –0.5 (SD 1.3); cycle 2: –0.8 (SD 1.6);
and cycle 3: –0.9 (SD 1.4) (Fig. 1 and Table III).
Changes in AS score across all 3 axes of movement involved in shoulder spasticity (internal rotation, extension and adduction) contributed to the improvement in AS-SSS (Table III). Changes were smaller in subjects not treated in the shoulder compared with subjects treated in shoulder muscles (Table III).
In cycle 3, a multiple regression analysis revealed a significant effect of incobotulinumtoxinA shoulder dose on AS-SSS (p = 0.0081), consistent with the greater improvement in AS-SSS with the higher incobotulinumtoxinA shoulder dose during this cycle.
Post hoc safety analysis
Functional outcomes. No weakness in shoulder muscles resulting in functional impairment was reported in subjects who received incobotulinumtoxinA treatment in shoulder muscles. Subjects who were treated in the shoulder muscles showed a similar functional improvement to those who were not treated in the shoulder. Specifically, subjects who were treated in the shoulder experienced a mean change in the DAS score of their principal therapeutic target domain of –0.5 (SD 0.6), –0.7 (SD 0.6) and –0.6 (SD 0.6) points in cycles 1, 2 and 3, respectively; the corresponding changes in subjects not treated in the shoulder were –0.6 (SD 0.7), –0.7 (SD 0.7) and –0.8 (SD 0.9), respectively.
At baseline, as would be expected, subjects who were treated in the shoulder reported a higher mean score in the DAS pain domain than those not treated in the shoulder (1.4 (SD 1.1) vs 1.1 (SD 1.0)). From baseline to the 4-week post-injection visit in each injection cycle, subjects who were treated in the shoulder
also experienced a greater mean improvement in DAS pain score than those not treated in the shoulder:
cycle 1: –0.5 (SD 0.8) vs –0.3 (SD 0.7); cycle 2: –0.5
(SD 1.1) vs –0.2 (SD 0.7); and cycle 3: –0.4 (SD 0.7) vs –0.2 (SD 0.9), respectively.
Mean GAS scores for upper-limb goals improved from baseline to the 4-week post-injection visit in each injection cycle for those subjects treated in the shoulder (cycle 1: 6.7 (SD 9.2); cycle 2: 12.5 (SD 8.5); cycle 3: 12.7 (SD 8.9)) and for those subjects not treated in the shoulder (cycle 1: 7.4 (SD 9.3); cycle 2: 9.0 (SD 9.5);
cycle 3: 13.4 (SD 8.5)).
Adverse events. In this post hoc analysis, no differences were observed in AE patterns according to treatment of the shoulder. The incidences of AEs per injection cycle for subjects treated in the shoulder vs those treated in the upper limb without shoulder treatment were: cycle 1: 40.4% and 36.3%; cycle 2: 40.6% and 32.9%; cycle 3: 26.2% and 25.0%, respectively. No SAEs related to treatment were reported.
The incidence of AEs of special interest that may indicate distant toxin spread was not generally higher in subjects treated in the upper limb without shoulder treatment
(2.2% (2/91), 6.1% (5/82) and 1.8% (1/56) in cycles 1, 2 and 3, respectively) than in those treated in the shoulder (7.7% (4/52), 2.9% (2/69) and 7.1% (6/84), respectively).
Over the course of the study, dysphagia was reported in only 5 subjects (3.2%). Two subjects treated in the shoulder reported dysphagia in cycle 1: one case of mild severity, deemed unrelated to treatment, and one case of worsening of pre-existing dysphagia. In cycle 2, one subject treated in the upper limb without shoulder treatment reported dysphagia of mild severity, unrelated to treatment. The remaining 2 subjects treated in the shoulder reported dysphagia in cycle 3; both cases were of mild severity, and only 1 was deemed related to treatment.
Local muscular weakness was reported at a low incidence among subjects treated in the shoulder and those treated in the upper limb without shoulder treatment (cycle 1: no cases; cycle 2: 0/69 (0.0%) and 1/82 (1.2%); cycle 3: 1/84 (1.2%) and 1/56 (1.8%), respectively). This had no effect on upper-limb function for either subject group.
In cycles 1 and 2, most subjects (272/294 (92.5%)) received doses <500 U. In cycle 3, incobotulinum-toxinA doses < 500 or ≥ 500 U were received by 33 and 51 subjects treated in the shoulder, and 36 and 20 who were not, respectively. The incidence of AEs and SAEs in cycle 3 did not appear to relevantly increase with the higher incobotulinumtoxinA dose within these groups. Among subjects who received incobotulinumtoxinA doses < 500 or ≥ 500 U in cycle 3, the incidence of AEs was 21.2% (7/33) and 29.4% (15/51) in subjects treated in the shoulder, vs 30.6% (11/36) and 15.0% (3/20) in those who were not. The incidence of SAEs in those who received incobotulinumtoxinA doses < 500 or ≥ 500 U was 0.0% and 2.0% (1/51 subjects), respectively, in subjects who were treated in the shoulder vs 2.8% (1/36) and 5.0% (1/20), respectively, in those who were not.
The incidence of dysphagia did not appear to be related to incobotulinumtoxinA dose: among the 4 subjects with dysphagia who were treated in the shoulder, 2 received < 500 U and 2 received ≥500 U. The one subject with dysphagia who was treated in the upper limb without shoulder treatment received < 500 U.
The TOWER study demonstrated the safety and efficacy of escalating total body doses of incobotulinumtoxinA (up to 800 U) for combined treatment of the upper and lower limbs in adults with spasticity due to cerebral causes (11). This post hoc analysis of data from the TOWER study assessed the effect of incobotulinumtoxinA for the treatment of shoulder muscles as part of a total upper-limb dose of 400 to 600 U. The TOWER study allowed for the treatment of the typical spastic shoulder muscle pattern, internally rotated/extended/adducted shoulder (3). The pectoralis major, latissimus dorsi, deltoideus pars clavicularis, teres major and subscapularis muscles are most commonly involved in the internal rotation, extension and adduction of the shoulder, and were treated with incobotulinumtoxinA in this study.
Efficacy, according to the level of impairment or reduction in AS scores as a measure of improvement in shoulder spasticity, was assessed using the AS-SSS. Following the concept of the REPAS score (25), this novel sum score takes into account the special features of frequent patterns of shoulder joint spasticity by summing the AS scores for internal rotation, extension and adduction of the shoulder, reflecting the shoulder as a functional unit. Results of this post hoc analysis showed that subjects treated with incobotulinumtoxinA in the shoulder muscles experienced improvement from baseline in muscle tone, as assessed by AS-SSS. Furthermore, multiple regression analysis confirmed a significant effect of incobotulinumtoxinA dose on reduction of spastic muscle tone with the higher dose of incobotulinumtoxinA in cycle 3.
In spasticity treatment trials, for the wrist and elbow, it is common to provide efficacy data for muscles acting on 1 axis, or a maximum of 2 axes, of movement only (usually the extension/flexion and pro-/supination axes) (9, 10, 22); however, this is different in the shoulder joint, because it is biomechanically the most mobile joint in the upper limb and involves 3 axes (27). Changes in the AS scores for all 3 axes of movement contributed to the improvement in the AS-SSS. All changes were higher in subjects treated in the shoulder than in those not treated in spastic shoulder muscles. This post hoc analysis showed a clinically relevant reduction in shoulder muscle spasticity with incobotulinumtoxinA, of the same order of magnitude as that reported previously for abobotulinumtoxinA, where mean changes from baseline to Week 4 on the 6-point derived modified AS for shoulder extension were –0.6 and –0.7 with 500 U and 1,000 U doses, respectively (22). In the current study, the mean improvement from baseline to the 4-week post-injection visit on the 5-point derived AS score for shoulder extension was –0.3 for cycle 1, –0.5 for cycle 2 and –0.4 for cycle 3.
Analyses of the upper-limb passive and active func-tional parameters following incobotulinumtoxinA treatment did not indicate any negative effects from paresis induced by treatment of shoulder muscles with incobotulinumtoxinA in terms of functional impairment; indeed, the changes in DAS indicated a clinically meaningful improvement of passive upper-limb function when shoulder muscles were treated. No differences in goal attainment in passive and active functional goals were reported in subjects who were treated in the shoulder compared with those who were not.
The state of shoulder spasticity is a substantial cause of pain leading to disability in subjects who have experienced stroke or any other lesion of the brain, and can impair quality of life (QoL) (3). Indeed, in the TOWER study, subjects treated in shoulder muscles reported higher DAS pain scores at baseline than those not treated in the shoulder, indicating a correlation between shoulder spasticity and pain. A beneficial effect of BoNT-A on shoulder pain in subjects with shoulder spasticity has been reported previously (15, 18–20, 22). However, while studies have reported statistically significant improvements in pain scores from baseline with BoNT-A (16, 17), not all studies have reported statistically significantly greater improvements compared with placebo or triamcinolone acetonide (15, 18, 19). In the current post hoc analysis, the changes in DAS indicated a clinically meaningful reduction in pain when shoulder muscles were treated, as subjects regained better passive upper-limb function.
QoL assessments were not included in the current post hoc analysis and will be reported separately, but QoL data from the main TOWER study were consistent with the efficacy findings, and indicated improvements in QoL across all 3 incobotulinumtoxinA injection cycles.
Finally, with regard to safety analyses, there was no difference in the reported AE pattern for subjects treated in shoulder muscles compared with those who were treated in the upper limb without shoulder treatment. Importantly, treatment of shoulder muscles with incobotulinumtoxinA did not induce additional local muscular weakness in shoulder muscles with reduced function. Physicians may have to prioritize the clinical patterns for treatment based on the maximum approved BoNT-A dose and subjects’ treatment goals, but, in the TOWER study, dose escalation in cycles 2 and 3 enabled more muscle groups and clinical patterns to be treated, including additional treatment of the shoulder, without compromising safety or tolerability (11).
In terms of potential limitations, it should be noted that this was a post hoc analysis and that the main study was non-randomized and lacked a placebo control (11). Here, subjects treated in spastic shoulder muscles were compared with those who were not. Furthermore, improvement in range of motion in the treated shoulder joint was not measured as an efficacy outcome in this analysis. A strength of this post hoc analysis of the TOWER study was the relatively large proportion of subjects who received treatment in spastic shoulder muscles in comparison with previous studies (15, 18–20, 22).
In summary, treatment of spastic shoulder muscles with incobotulinumtoxinA was well tolerated with no new safety concerns, and improved spasticity without causing excessive local weakness of the shoulder muscles that could have led to a net negative effect on
upper-limb function. IncobotulinumtoxinA doses of up to 250 U are now approved in the EU for treatment of shoulder spasticity as part of a total dose of 500 U for treatment of the upper limb (13), underlining the need for a multi-level, multi-pattern approach to optimize the outcome of botulinum neurotoxin treatments.
The authors would like to thank Doris Rosenwald from Merz Global Product Safety for her contribution to the study. This study was supported by Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany. Medical writing support, under the direction of the authors, was provided by Claire Cairney, PhD, CMC Connect, McCann Health Medical Communications, and Tracey Lonergan, PhD, on behalf of CMC Connect, funded by Merz Pharmaceuticals GmbH, in accordance with Good Publication Practice (GPP3) guidelines.
Conflicts of interest. JW received research grant support from, and served as a consultant for, Allergan, Ipsen, Medtronic and Merz; DB served as a consultant for Allergan, Almirall, Ipsen, Medtronic and Merz; AS is an employee of Merz Pharmaceuticals; BF-B is an employee of Merz Pharmaceuticals; OS is a former employee of Merz Pharmaceuticals; MA is an employee of Merz Pharmaceuticals; DMS received research grant support from, and served as a consultant for, Allergan, Ipsen and Merz.


 Click to show fullsize
Click to show fullsize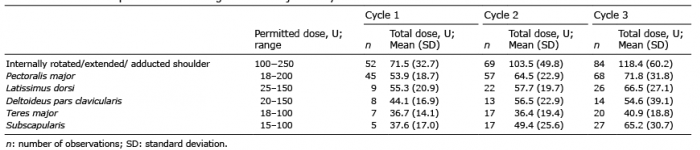 Click to show fullsize
Click to show fullsize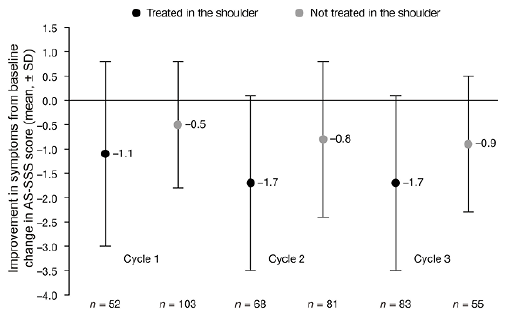 Click to show fullsize
Click to show fullsize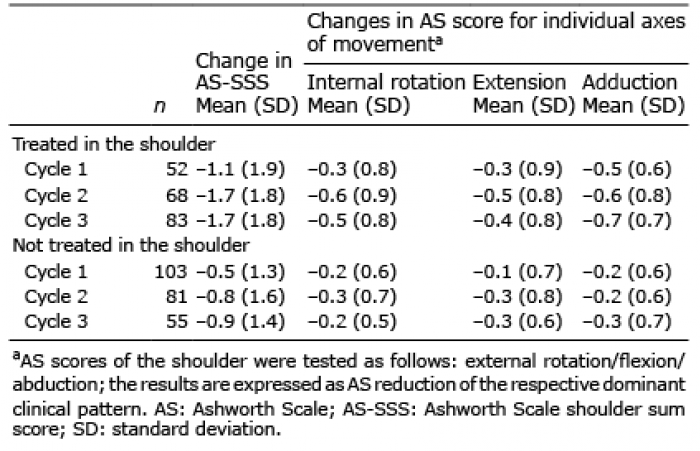 Click to show fullsize
Click to show fullsize