
From the 1Department of Physical Medicine and Rehabilitation, Daejeon St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, 2Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital, Seoul, 3Department of Ortgopedic surgery, Regional Rheumatoid and Degenerative Arthritis Center, Jeju National University Hospital, Jeju National University College of Medicine, Jeju, and 4Department of Rehabilitation Medicine, Regional Rheumatoid and Degenerative Arthritis Center, Jeju National University Hospital, Jeju National University College of Medicine, Jeju, Republic of Korea
Objective: To identify preoperative physical performance factors that predict stair-climbing ability at one month after total knee arthroplasty.
Design: Prospective cohort study.
Setting: University-based rehabilitation centre.
Subjects: Eighty-four patients who underwent a primary unilateral total knee arthroplasty.
Methods: Before and one month post-operation, the patients completed physical performance tests, including a stair-climbing test, a 6-minute walk test, a Timed Up-and-Go test, tests of the isometric flexor and extensor strength of the operated and non-operated knees, and instrumental gait analysis. Disease-specific physical function was measured by the Western Ontario McMaster Universities Osteoarthritis Index.
Results: Correlation analysis showed that postoperative stair-climbing test scores were significantly correlated with preoperative physical performance and function. Linear regression analysis showed that postoperative stair-ascent scores were correlated with preoperative Timed Up-and-Go test scores and peak torque of the extensor of the operated knee. Postoperative stair-descent scores were positively correlated with preoperative stair-descent scores and age.
Conclusion: The results show that preoperative balance ability and quadriceps strength in the operated knee could influence postoperative stair-climbing ability at one month after total knee arthroplasty. These findings will be useful for developing pre- and post-operative rehabilitation strategies for improving stair-climbing ability in the early stages after total knee arthroplasty.
Key words: knee osteoarthritis; total knee arthroplasty; rehabilitation, stair-climbing ability; prediction.
Accepted Apr 27, 2020; Epub ahead of print May 13, 2020
J Rehabil Med 2020; 52: jrm00064
Correspondence address: Bo Ryun Kim,Department of Physical Medicine and Rehabilitation, Korea University Anam Hospital, 73, Goryeodae-ro, Seongbuk-gu, Seoul, Korea. E-mail: brkim08@gmail.com
The aim of this study was to find out which physical performance factors in patients before a knee replacement operation (total knee arthroscopy) can be used to predict what the patient’s stair-climbing ability might be at one month after the operation. Patients having a primary total knee arthroplasty in one knee were enrolled in a prospective cohort study (a study that follows a group of similar patients over time, who differ in terms of a number of factors). The results show that scores on the following tests before the operation were the best independent predictors of the time taken to climb the stairs after the operation. These were: Timed Up-and-Go test scores and extensor torque of the operated knee. The time taken to descend the stairs after the operation were strongly predicted by the time taken to descend stairs before the operation and the patient’s age. These findings will be useful in developing pre- and post-operative rehabilitation strategies for improving stair-climbing ability in the early stages after total knee arthroplasty.
Knee osteoarthritis (OA) is a very common disease and a leading cause of joint pain, stiffness, oedema, disability and functional limitation in older adults (1). Total knee arthroplasty (TKA) is one of the most effective surgical interventions for patients with end-stage knee OA (2). Previous studies have revealed that TKA significantly improves knee pain, self-reported physical function, and quality of life (3). Even in cases of successful TKA, several patient physical performance indexes, including gait and stair-climbing ability, improve slowly in the months after surgery. Walsh et al. (4) reported that, compared with age-matched healthy individuals, patients consistently had difficulty ascending and descending stairs at 1 year after TKA.
Stair ascent and descent place great demand on lower extremity muscles and joints (5), and both knee OA and TKA patients potentially encounter stairs on a daily basis. Thus, clinicians and patients have identified stair-climbing as a critical functional activity before and after TKA (6, 7). A recent study investigating the expectations of patients undergoing total knee replacement reported that stair-climbing was the second most expected outcome and that 30.5% of patients were dissatisfied with the improvements in their ability to go up and down stairs minimum 6 months after the operation (8).
There is evidence that some physical, demographic and psychosocial factors are related to stair-climbing ability in patients with knee OA (9). However, evidence showing that similar factors affect stair-climbing ability in the TKA population is scarce; thus, more extensive research is required (9).
Identifying the preoperative predictors that affect stair performance in the first month following TKA is of great importance. This is the critical period during which patients generally return home after TKA surgery. Therefore, performance predictors will be helpful for determining patients’ expected level of stair-climbing ability. Such predictors can also determine the expected level of independence in community ambulation and the need for postoperative locomotor rehabilitation (10).
Therefore, the aim of this study was to identify the preoperative physical performance factors that predict stair-climbing ability at one month following TKA.
Participants
The study was designed as a prospective cohort study. All patients who were diagnosed with end-stage primary OA of the knee, who were scheduled to undergo unilateral primary TKA between 2014 and 2016 at the Department of Orthopedic Surgery at OO Jeju National University Hospital, Jeju, Republic of Korea and who consented to participate in the study were recruited.
Patients were included in this study if they could walk independently with or without an ambulatory aid before surgery. Patients who had previous neurological or orthopaedic disease causing ambulatory deficits, such as orthopaedic injury or previous joint surgery in the lower extremities, unstable cardio-respiratory diseases; or who had undergone bilateral TKA were also excluded.
The study protocol was approved by the institutional review board of OO Jeju National University Hospital, and all participants provided written informed consent.
Rehabilitation protocol
Two weeks after surgery all patients were transferred to the rehabilitation department of the hospital and completed a rehabilitation programme that included passive knee range-of-motion (ROM) exercises, progressive resistance-based strengthening exercises of the affected leg, gait training, ergometer-monitored aerobic exercises, functional training for transfers and stair-climbing, and physical modalities, such as cryotherapy and transcutaneous electrical nerve stimulation, to relieve knee pain and swelling. Progressive resistance-based strengthening exercises consisted of concentric knee extension and flexion exercises and hip abduction and adduction exercises that were performed on air resistance machines (HUR® machines, HUR Led, Kokkola, Finland) at 30% of the 1-repetition maximum (1RM) for 3 sets of 15 repetitions in a 30-min session. The 1RM was reassessed every week, and the training prescription was advanced to a new resistance level until the patients performed at 60% of the 1RM for 3 sets of 10 repetitions (11). Gait training was performed using a lower-body positive-pressure (LBPP) treadmill (AlterG® M320 Anti-Gravity Treadmill®, Alter G, Inc., Fremont, CA, USA). All patients started at a workload of 50% of their bodyweight (BW) and walked at a speed of 2.0 km/h. When the patients could perform more repetitions than initially set for a specific % BW and gait speed, the training was increased until a workload of 90% of BW and a speed of 3.5 km/h were reached (12). All rehabilitation programmes were performed 5 times per week for a 2-week period and were supervised by physical therapists. Postoperative knee pain was controlled by oral medication, and only the dosage of medication was changed during the 2-week rehabilitation period. Two weeks after the end of the inpatient rehabilitation programme, all patients were discharged to home and participated in a home exercise programme.
Outcome measures
Before and one month after TKA, all patients completed a series of physical performance tests, including a stair-climbing test (SCT), a 6-min walk test (6MWT), a timed up-and-go test (TUG), tests of the isometric knee flexor and extensor strength of the operated and non-operated knee, and instrumental gait analysis to measure spatiotemporal parameters. Self-reported disease-specific physical function was measured using the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC), and self-reported quality of life was measured by using the Euro QOL Five Dimensions (EQ-5D) questionnaire. Knee pain was assessed using a visual analogue scale (VAS).
Assessment of physical function
Stair-climbing test. The SCT was measured as the time required to ascend and descend a flight of stairs (12 steps total, each step 17 cm high and 25 cm wide). The patients were asked to ascend or descend the stairs as quickly as possible on the word “go”. Each trial was performed with a 5-min rest interval, and the best score was recorded (13). All patients completed 3 trials, and the fastest time was recorded. There was a handrail on the stairs used for the SCT set, and patients were allowed to use it during the test
Six-min walk test. The 6MWT is a performance-based measure of exercise tolerance and functional walking capacity in adults. The patients were instructed to walk as far as possible for 6 min, through a 50-m hallway indicated with lines. The 6MWT has high reliability in patients who have undergone primary TKA (14).
Timed up-and-go test. The TUG test is an evaluation of dynamic balance performance. Each patient sat on a chair with his or her back against the back of the chair (seat height, 44 cm; depth, 45 cm; width, 49 cm; arm rest height, 64 cm) placed at the end of a marked 3-m distance. The patients were instructed to stand up on the word “go”, walk at a comfortable speed past the 3-m mark, turn around, walk back, and sit down again in the chair without physical assistance, while being timed. The TUG tool has acceptable concurrent validity for measuring dynamic balance (15, 16).
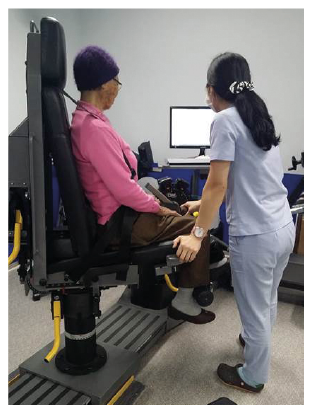
Measurement of the isometric strength of the knee extensors and flexors. The maximal isometric strength of the bilateral knee extensors and flexors was measured using an isokinetic dynamometer (HUMAC®/NormTM, CSMI, Stoughton, MA, USA; Fig. 1). All patients relaxed their muscles with light stretching before the test. The participants were seated on a specially designed chair with a hip angle of approximately 85° (17). The distal shin pad of the dynamometer was attached 2–3 cm proximal to the lateral malleolus using a strap. Additional straps were applied across the chest, pelvis, and mid-thigh to minimize inappropriate trunk movements during thigh muscle contraction. The alignment of the dynamometer rotational axis with the knee joint rotational axis (lateral femoral epicondyle) was adjusted at the beginning of each trial. The gravity effect torque was recorded for each subject and was used to correct the torque measurements during all tests. The patients were asked to grasp the sidebars during the testing procedure. The length of the moment arm as measured from the lateral femoral epicondyle to the centre of the force transducer at the shin was kept constant. Data were obtained from digitized signals. After a structured warm-up with the knee joint fixed at 60°of flexion for maximal isometric force generation (18) the patients were asked to perform maximal voluntary contractions until the torque did not increase by more than 5% during 3 successive attempts. Knee flexion and extension were performed as discrete movements in a single direction (i.e. non-reciprocal). Each contraction lasted 4–5 s, and the contractions were separated by 2 min of rest. After a 5-min rest, the same procedure was performed with the contralateral lower limb. The variables analysed included the peak torque (PT) of the operated and non-operated knee extensor and flexor.
Fig. 1. Isometric test. Permission has been given to publish this photo from the therapist and the patient.
Gait analysis. The spatiotemporal variables of gait were measured using a validated 24-point wireless inertial sensing device (G-Walk®, BTS Bioengineering S.p.A., Milan, Italy). The patients were instructed to walk 8 m at a comfortable speed as naturally as possible. The gait data were collected and transmitted via Bluetooth to a personal computer, where they were processed using the BTS G-Walk® system, a dedicated software program that measures gait variables, such as gait speed, cadence, stride length, duration of gait cycle, stance phase, swing phase, and double support.
Western Ontario McMaster Universities Osteoarthritis Index. The multidimensional WOMAC questionnaire asks questions about pain, stiffness, and physical function, and has been used previously to measure self-reported disability in patients with knee OA. The questionnaire includes 5 pain variables, 2 stiffness variables, and 17 physical function variables, each of which is scored using a Likert scale (0, none; 1, slight; 2, moderate; 3, very; and 4, extremely), as recommended by the Outcome Measures in Rheumatology Clinical Trials. The Likert scale is used to determine the degrees of pain, stiffness and difficulty the patient experienced while performing each of 17 activities in the preceding 48 h. Higher scores indicate greater levels of pain, stiffness, and difficulty (19).
EuroQoL 5-dimensions questionnaire. The EQ-5D questionnaire is used to evaluate self-reported quality of life, and the EQ-5D index is widely used to measure general health status. The instrument consists of a questionnaire with 5 dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is represented by 1 question with 3 severity levels (no problems, some or moderate problems, and extreme problems). Scores were transformed using utility weights derived from the general Korean population and ranged from −1 to 1. Higher scores indicate better overall health status. The formula for the EQ-5D index has been presented by Lee et al. (20).
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). All variables were subjected to descriptive statistics. A paired t-test was used to compare the pre- and postoperative physical performance parameters, which were measured before and one month after TKA, respectively. Bivariate Pearson correlation analysis was used to assess the correlation between preoperative physical performance and postoperative stair-climbing ability. In the multivariate linear regression analysis, variables that had a p-value < 0.05 in the bivariate analysis were entered into the model selection procedure using a backward stepwise process. The multivariate regression analysis was used to determine which objective performance-based physical function variables best explained the postoperative stair-climbing test results at one month after TKA. A p-value < 0.05 was considered statistically significant.
Of the 213 patients who underwent TKA during the 2-year study, 84 patients who underwent a primary unilateral TKA, met our inclusion criteria, and completed a one-month evaluation after TKA were recruited into the study. Of the excluded patients, 48 had a history of previous orthopaedic injury, and 27 had undergone bilateral TKA. The remaining excluded patients comprised 23 patients with a history of neurological disease, such as stroke and myelopathy, and 31 patients who did not complete the 1-month evaluation after TKA. The baseline demographic and disease-related characteristics of the subjects are presented in Table I.
The mean (standard deviation, SD) age and body mass index (BMI) were 72.0 years (SD 6.0) and 27.1 kg/m2 (SD 3.6), respectively. Of the 84 patients, 42 (50%) had osteoporosis, and 63 (75%) had Kellgren-Lawrence (K-L) grade IV OA. The K-L grade is a common method for classifying the severity of knee OA, and grade IV indicates marked joint space narrowing, severe sclerosis and definite bony deformity (21). No patients experienced infections, wound problems, nerve injuries, or any other postoperative complications.
Preoperative and postoperative evaluation of performance-based physical function, self-reported physical function, and quality of life
Table II shows the preoperative and postoperative evaluations of the patients’ physical performance, physical function, and quality of life. The postoperative SCT-ascent and SCT-descent scores did not differ significantly from the corresponding preoperative scores, and the patients displayed significant improvements in 6MWT performance, TUG test scores, knee extension ROM, PT of the non-operated knee flexor, gait speed, cadence, function according to the WOMAC, EQ5D scores, and VAS scores.
Table I. Demographic and disease-related characteristics of the subjects (n = 84)
Table II. Preoperative and postoperative evaluation of physical performance, physical function, and quality of life
Correlation between preoperative factors and postoperative stair-climbing ability
Table III shows the correlations between preoperative function and postoperative SCT scores. The preoperative scores of both SCT-ascent and SCT-descent were significantly positively correlated with preoperative stair-climbing ability, TUG scores, and age. The WOMAC-function was significantly positively correlated with only the postoperative SCT-descent score.
Furthermore, the postoperative SCT-ascent and SCT-descent scores were significantly negatively correlated with preoperative 6MWT performance and both the flexor and extensor torque of the operated and non-operated knee.
Table III. Correlation between the preoperative physical performance and postoperative stair-climbing ability
Preoperative factors predicting postoperative stair-climbing ability according to the multivariate linear regression analysis
Linear regression analysis identified preoperative TUG scores (β = 0.28, p < 0.01) and PT of the operated knee extensor (β = –0.23, p = 0.03) as predictors of post-operative SCT-ascent scores; moreover, the analysis identified preoperative SCT-descent scores (r = 0.28, p = 0.01) and age (β = 0.20, p = 0.04) as predictors of postoperative SCT-descent scores (Table IV).
Table IV. Preoperative factors predicting the postoperative stair-climbing ability by multivariate linear regression analysis
This study aimed to identify the preoperative physical performance factors that predict stair-climbing ability at one month following TKA. The results revealed that preoperative TUG test scores and the extensor torque of the operated knee were significant independent predictors of postoperative stair ascent time and that preoperative stair descent time and age could predict postoperative stair descent time. In addition, several preoperative physical performance indexes, including 6MWT results, the extensor and flexor torque of the operated and non-operated knees and stair-climbing ability, were significantly correlated with postoperative stair-climbing ability at one month after TKA.
Stair-climbing is one of the important functional activities of daily living for maintaining mobility and independence (6), and most osteoarthritic patients select functional stair-walking as one of their criteria for successful rehabilitation in terms of returning to previous activity levels (22). Furthermore, following TKA, the ability to safely ascend and descend stairs is an exceptionally important concern. The majority of falls occur on stairs in a domestic setting (23). These falls may result in major injuries or even death; an estimated 10% of fall-related deaths occur on stairs (24). As mentioned in the introduction, given that the first month after TKA is the critical period during which patients return home after surgery, providing an adequate appraisal of a person’s ability to safely negotiate stairs soon after TKA is essential to preventing serious injury in the home. If we can predict the physical performance factors that affect stair-climbing ability at one month after TKA, rehabilitation strategies will be able to focus on improving these factors. In addition, early rehabilitation and proper management after TKA are important for successful negotiation of stairs during activities in the community.
The TUG test has acceptable concurrent validity with the Berg Balance Scale and with gait speed for measuring dynamic balance and shows high repeatability in patients awaiting TKA (15, 16). TUG test performance depends on a combination of neuromuscular factors (walking ability, lower limb strength, and balance) that also play important roles in stair-climbing activity. Thus, preoperative balance ability is important for good stair-climbing ability after TKA.
The correlation between stair ascent time and extensor strength in the operated knee has already been shown in several studies (7, 22). Valtonen et al. (25) revealed that knee extensor and flexor muscle strength and pain in the knee with OA were independently associated with stair ascent times. Furthermore, Mizner et al. (7) reported that preoperative quadriceps strength strongly predicts functional variables at 1 year after TKA. Interestingly, we found that muscle torque on both the operated and non-operated sides was significantly correlated with the time required to ascend stairs. The associations between stair ascension time and the muscle torque of both legs might be attributable to the fact that walking upstairs is a very challenging functional task. Moreover, knee extensor and flexor torque on the non-operated side was associated with stair ascent time. The results of the current study confirm that the muscle strength of both sides is associated with stair ascent time in TKA patents.
Secondly, this study found that preoperative stair descent time and age predicted postoperative stair descent time, and that TUG test scores, 6MWT performance, and the extensor and flexor torque of the operated and non-operated knees were also significantly associated with postoperative stair descent time. In terms of stair descending activity, patients who completed self-reported assessments indicated a greater fear of falling during stair descent than during stair ascent (26), and Whitehouse et al. indicated that descending stairs was one of the most difficult tasks to complete (27). Another study reported that 6 months after TKA, up to 60% of respondents had moderate-to-extreme difficulty in descending stairs (26, 28). Thus, balance ability and the thigh muscle strength of both the operated and non-operated sides, which have a significant effect on the ability to ascend stairs, can also be expected to have a significant impact on the ability to descend stairs. In addition, Cooper et al. (29) showed that age is the strongest predictor of multidimensional functional outcomes after TKA. This result can be explained by the fact that older patients have worse perceived function and physical performance during activities after TKA. As age is a non-adjustable factor, elderly OA patients with poor stair descent ability are encouraged to use an elevator or undertake lifestyle modifications rather than descending stairs.
The 6MWT has been favoured as a performance measure of exercise tolerance and functional walking capacity due to its strong responsiveness to change over time in patients with TKA (30). Stair activities place the greatest demands on lower extremity muscles (5) and are challenging; thus, the exercise tolerance and endurance of the lower extremities are important in stair-climbing ability after TKA. The results of the current study revealed that preoperative 6MWT performance and gait performance were related to postoperative stair-climbing ability.
In this study, range of knee flexion was not associated with stair-climbing ability. A previous study consistently showed that during stair ascent, TKA patients showed reductions in the knee flexion angle at contact, maximum knee flexion, total knee flexion ROM and ascent velocity compared with healthy controls (31). It is apparent that, for more demanding tasks, such as stair ascent, knee kinematics and ascent velocity are not restored to functional levels.
Although our results showed that the maximal knee flexion ROM at resting state was significantly decreased after TKA, it was within the normal ROM needed for stair-climbing reported in a previous study (32). The stair-climbing ability did not change after TKA in this study. This seems to be because the effect of the rehabilitation programme after TKA included ROM exercise of the knee. Thus, we suggest that rehabilitation programmes focus specifically on increasing knee ROM to achieve good stair-climbing ability.
Previous studies have shown that the preoperative conditions of TKA patients are a strong indicator of postsurgical recovery (30). Pre- and postoperative comparisons of the operated knee may be more valuable for understanding stair gait following TKA. However, only a few studies have compared the post-operative results of TKA patients to their preoperative results (30, 33).
The results of the current study showed that function, pain, and quality of life were significantly improved at one month after TKA compared with before TKA. However, SCT scores did not show significant changes. This finding is consistent with those of a previous study showing that stair-climbing activity was affected by high levels of disability, which persisted until 4 weeks after TKA (26). Ouellet et al. (33) showed that large locomotor deficits are still present in patients after TKA; this finding explains why patients displayed slower walking and stair-ascent speeds and reduced performance on the TUG test and 6MWT. Mizner et al. (30) also demonstrated that, from between the preoperative test and the 1-month postoperative test, several performance-based measures of activities, such as the SCT, the 6MWT, and the TUG test, worsened. However, the rehabilitation therapy in that study was less intense than the protocol used in our study. Mizner et al. (30) provided rehabilitation therapy for 3 days, according to an inpatient hospital care protocol; the patients then underwent home physical therapy for 2–3 weeks. In contrast, our study provided 2 weeks (10 days) of intensive inpatient rehabilitation therapy. Our results are consistent with those of previous studies showing that intensive rehabilitation programmes that include resistance-based strength exercises, balance, gait and stair-climbing training are essential in the first months following TKA (27, 30, 33).
Study limitations
This study has several limitations. First, the study results may not be generalizable to all patients undergoing TKA because this study included only people with OA who underwent a unilateral primary TKA. In addition, because we did not analyse the postoperative variables at time points other than one-month post-TKA, we cannot guarantee that the predictors of gait function in our study will also be significant predictors of performance several years post-TKA. Therefore, long-term follow-up studies that address these issues are warranted. Secondly, we did not compare our patients with those who did not undergo postoperative rehabilitation. The TUG test was performed at a comfortable speed and not as quickly as possible; thus, our results are not considered to reflect a risk of falling or a dynamic balance problem. Additional studies of the causal relationships between postoperative gait variables and the effects of our intensive rehabilitation programme are needed. Finally, almost all the participants in our study were female. Previous studies have demonstrated that female patients have significantly worse preoperative pain and function than males. It has been shown that men and women differ in terms of surgery preferences and that, compared with men, women are more likely to wait until their functional status worsens before being willing to undergo surgery (2).
Conclusion
This study clarified that balance ability and the extensor torque of the surgical knee influence postoperative stair ascending ability. In addition, preoperative stair descending ability and age influence postoperative stair descending ability. This study suggests that variable preoperative rehabilitation strategies that focus on improving balance and strength will improve stair-climbing ability in the early stages after TKA. Furthermore, we recommend that patients who have a poor prognosis in terms of stair-climbing ability after TKA undergo intensive postoperative rehabilitation to improve this ability.
Conflicts of interest. No commercial party with any direct financial interest in the results of the research supporting this article has conferred or will confer a benefit to the authors or to any organization with which the authors are associated.


 Click to show fullsize
Click to show fullsize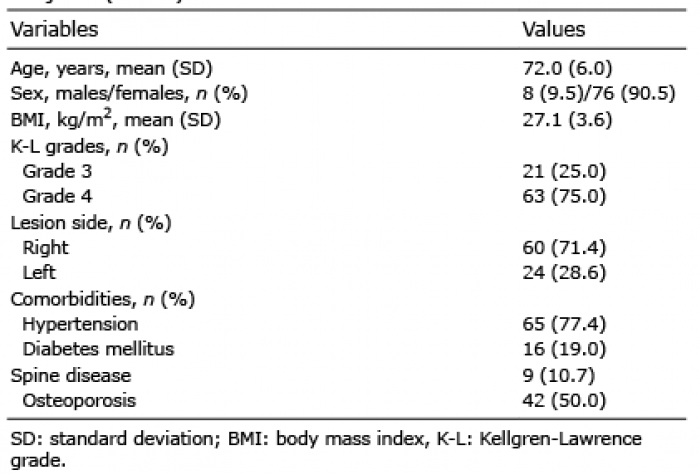 Click to show fullsize
Click to show fullsize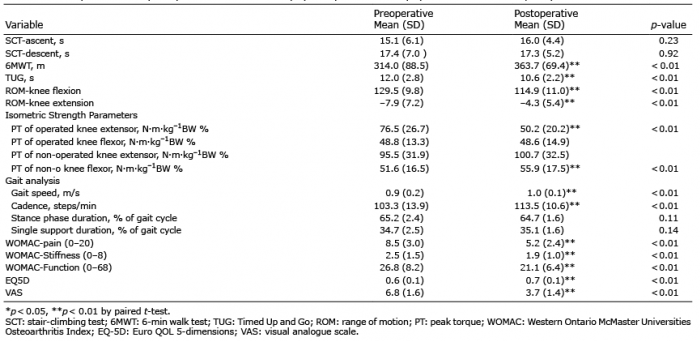 Click to show fullsize
Click to show fullsize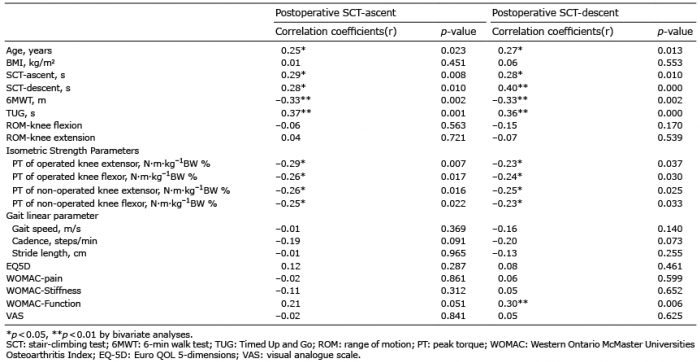 Click to show fullsize
Click to show fullsize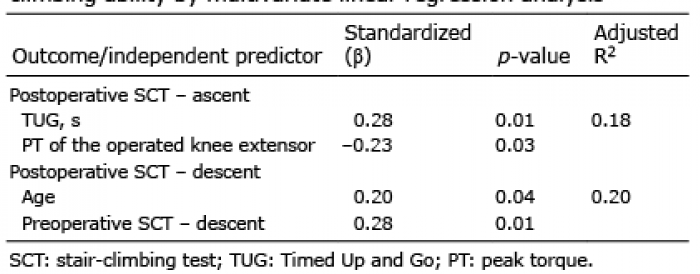 Click to show fullsize
Click to show fullsize