
From the 1Department of Rehabilitation and Brain Trauma, Division of Clinical Neurosciences, Turku University Hospital and University of Turku, 2Department of Expert Services, Turku University Hospital and 3Department of Biostatistics, University of Turku, Turku, Finland
Objective: To compare to what extent the presence of contralateral spatial neglect affects functional recovery and outcome among patients with right or left stroke after subacute inpatient rehabilitation. Methods: Observational cohort study comparing functional improvement and outcome. The same admission data-set was used as in part 1 of this study.
Results: Right and left stroke rehabilitants with equally mild neglect and those without neglect (a total of 4 subgroups) all improved proportionally as much, but those with neglect, irrespective of stroke side needed a longer stay in inpatient rehabilitation. At discharge, total disability did not differ significantly between the 2 neglect subgroups, but those with left stroke had significantly lower Functional Independence Measure cognitive sub-score and score in communication. Rehabilitants with neglect, irrespective of stroke side had higher motor, cognitive and total disability and were more often institutionalized than those without neglect.
Conclusion: Mild neglect did not impair recovery after right or left stroke, but rehabilitants with neglect were more disabled and needed a longer rehabilitation inpatient stay than those without neglect.
Key words: functioning; inpatient; outcome; recovery; subacute rehabilitation; spatial neglect; stroke laterality.
Accepted May 18, 2020; Epub ahead of print May 29, 2020
J Rehabil Med 2020; 52: jrm00071
Correspondence address: Sinikka Tarvonen-Schröder, Division of Clinical Neurosciences, Turku University Hospital, PO Box 52, FI-20521 Turku, Finland. E-mail: sinikka.tarvonen-schroder@tyks.fi
Mild contralateral spatial neglect (inattention) did not impair recovery of patients after right or left stroke, but rehabilitants with neglect were more disabled and needed longer rehabilitation than those without neglect. At discharge from rehabilitation, overall disability did not differ significantly between right and left stroke rehabilitants with neglect, but those with left stroke had more problems in cognitive-communicative ability. Rehabilitants with neglect, irrespective of stroke side, had higher motor, cognitive and overall disability and were more often institutionalized than those without neglect.
Hemi-spatial neglect is considered a disabling cognitive syndrome, defined as a failure to attend to the contralateral personal, peri- or extra-personal space (1). Despite substantial research it is still poorly defined as a condition per se (2). Hemi-spatial neglect has been linked with long hospitalization and slower, more attenuated rehabilitation (3–8), poor motor recovery (9, 10) and falls (3), poor rehabilitation outcome (3, 6, 8, 10–15) and reduced likelihood of being discharged home (3, 8). More severe neglect has been associated with more suppression on the pattern of recovery (9) and poor recovery in many domains of activities of daily living (ADL) (16). However, on closer scrutiny (2) combining previous data, only a paucity of evidence has been found to support the presence of hemi-neglect as a key predictor of functional recovery after stroke. In a recent study, hemi-spatial neglect without other cognitive impairments was not found to be a significant predictor for regaining independent gait (17).
Future studies should take the many confounding factors (14, 18) and measurement limitations (2) into account. As there are wide-ranging differences in the amount and rate of functional recovery among stroke survivors with and without neglect during the initial months after stroke onset (19), the relationship between neglect and functional recovery post-stroke warrants further investigation (2). In addition, research using standardized (20), quantitative, validated and sensitive measures (1), and especially studies on patients with left hemisphere stroke and neglect are needed (20).
The aims of this study were to extend previous research on the consequences of spatial neglect on rehabilitation outcomes and, especially, to examine the possible effect of stroke laterality. The objective of this study was to investigate to what extent the presence of contralateral spatial neglect is associated with functional recovery in right compared with left stroke.
This is an observational cohort study. Patients and methods, including the division of the participants into 4 subgroups, their background information, demographic and admission clinical variables, including the presence and severity of neglect, have been described in part 1 of this study (21).
Functional outcome variables during the rehabilitation and at discharge: Functional Independence Measure
The Functional Independence Measure (FIM) was routinely performed at admission and discharge (discharge scores in Table I) by a rehabilitation nurse qualified to use this outcomes management tool. The admission FIM scores (total score, motor and cognitive sub-scores, domain and item scores) have been described in part 1 of this study (21). A range of outcome scores were calculated (Table II), as follows.
FIM efficiency is the mean change in FIM score per day. This statistic is calculated as the mean change in FIM score during the rehabilitation, divided by the mean length of stay. FIM effectiveness is FIM at discharge minus FIM on admission × 100%. Corrected FIM effectiveness is calculated as FIM effectiveness/(A – FIM on admission), where A is generally taken to be 126 points for total FIM score and 91 points for motor FIM score. This corrected version of FIM effectiveness corrects the ceiling effect present in FIM gain. FIM motor effectiveness with advanced correction corrects for both floor and ceiling effects and is calculated so that motor FIM effectiveness is approximately 0.65, whereupon A varies, being 42, 64, 79, 83, 87, 89, or 91 points when the admission FIM motor sub-score is 13–18, 19–24, 25–30, 31–36, 37–42, 43–48, or 49–90 points, respectively (22, 23).
In addition, the number of falls and near-fall incidents during the stay were calculated. Prior to onset of this study in 2015, a fall prevention programme, including comprehensive electronic reporting of all fall and near-fall events, was implemented. A fall was defined as an event that resulted in a person coming to rest inadvertently on the ground or another level and other than a consequence of sustaining a violent blow, loss of consciousness, sudden onset of paralysis, such as stroke or an epileptic seizure (24). A near fall was defined as a major stumble event or loss of balance reported by a staff member, that would have resulted in a fall if sufficient recovery mechanisms were not activated (25) or assistance given by another person.
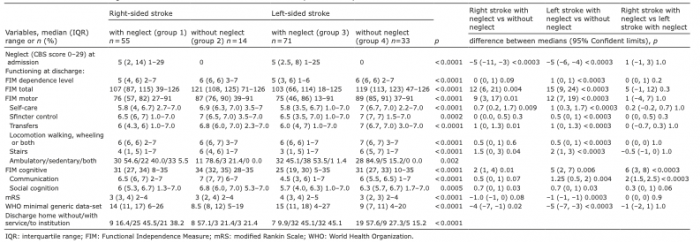
Table I. Functional outcome at discharge of the four rehabilitant subgroups (including their admission Catherine Bergego Scale (CBS) scores) with between-group differences using Kruskal-Wallis test. Difference on Hodges-Lehmann estimate for median difference. All pairwise comparisons are Bonferroni corrected
Table II. Functional improvement and outcome during the stay in rehabilitation of the four subgroups with between-group differences using Kruskal-Wallis test. Difference on Hodges-Lehmann estimate for median difference. All pairwise comparisons are Bonferroni corrected
Other scales besides FIM at discharge:
A neurologist assessed the modified Rankin Scale (mRS) score and the World Health Organization (WHO) minimal generic data-set covering functioning and health, aiming at assessing functioning in a simple validated way.
The mRS (Table I) is a simple tool used for measuring disability or dependence of neurological and stroke patients, encompassing levels from 0 to 5: “independent patients with no residual symptoms” to “dependent patients who require continuous care” (level 6 denoting death) (26).
The WHO minimal generic data-set (Table I) consists of 7 domains: energy and drive functions, emotional functions, sensation of pain, carrying out daily routine, walking, moving around, and remunerative employment. Each item is scored 0–4 (no, mild, moderate, severe or total/extreme difficulty), the sum score ranging from 0 to 28 (27).
The participants signed a written informed consent. The same data-set was used in part 1 of this study (21). Some of the participants were also included in a previous study (31).
The ethics committee of the University of Turku and Turku University Hospital approved the study (19.5.2015, 73/2015). The ethical standards of the World Medical Association Helsinki Declaration of 1975, revised in 1983, were followed.
Statistical analysis
Categorical variables were described using frequencies and percentages and, for continuous variables, medians with range of values and 25th and 75th percentiles (interquartile range; IQR) were used. The comparisons between the 4 subgroups for continuous variables were carried out using the non-parametric Kruskal–Wallis test and for pairwise comparisons Mann–Whitney U test with Bonferroni correction was used. Difference on Hodges-Lehmann estimate for median difference was used. With categorical variables between-group comparisons were assessed with χ2 test, or, in the case of small cell frequencies, Fisher’s exact test. Spearman’s correlation coefficient was used to test the correlation between Catherine Bergego Scale (CBS) score (varying from 0 to 29) and measures of functioning at discharge. Correlations of 0–0.29 were considered weak, 0.30–0.49 moderate, 0.50–0.69 strong, and 0.70–1.00 very strong. p-values below 0.05 (2-tailed) were considered statistically significant. Statistical analyses were performed using SAS 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Demographic data, clinical characteristics and functioning of the 4 subgroups at admission to rehabilitation are described in part 1 of this study (21). Outcome measures at discharge from rehabilitation with significant between-group differences are shown in Table I.
At discharge, FIM cognitive sub-score and score in communication were lower in left than in right stroke with neglect, but otherwise no significant differences were found in FIM, mRS or the WHO minimal generic data-set scores or institutionalization between the 2 subgroups with neglect. Rehabilitants with neglect, irrespective of stroke side had lower FIM total score, motor and cognitive sub-score and higher disability assessed with the other instruments (mRS and the WHO minimal generic data-set), and they were more often institutionalized than those without neglect (Table I).
FIM efficiency and corrected motor effectiveness were higher in left stroke rehabilitants with neglect compared with those without neglect. Effectiveness was higher and length of stay longer in the subgroups with neglect than in those without, but total corrected effectiveness and motor effectiveness with advanced correction did not differ significantly between the 4 subgroups. Most falls and near-falls were found in those with neglect (Table II).
When comparing functional improvement of all rehabilitants with neglect (n = 126) with those without neglect (n = 47), FIM efficiency (median, IQR; range) was 0.354 (0.111, 0.600; –1.0 to 1.590) vs 0.167 (0.0, 0.348; –0.286 to 1.313), p = 0.0047, FIM effectiveness% 14.946 (3.077, 36.471; –25.0 to 150.0) vs 2.609 (0.0, 7.576; –4.082 to 28.571), p < 0.0001, and corrected FIM total effectiveness 0.273 (0.083, 0.591; –0.390 to 0.929) vs 0.282 (0.0, 0.450; –0.167 to 1.0), p = 0.2185, respectively.
Spearman correlations between neglect severity at admission (CBS score range 0–29, median 3, n = 173) and level of functioning and dependence at discharge of rehabilitation (FIM total, motor and cognitive, mRS, and the WHO minimal generic data-set) in those with right (n = 69) and left (n = 104) stroke are shown in Table III. Moderate to strong correlations were found.
Table III. Spearman’s correlation coefficients between admission neglect severity and measures of functioning at discharge
Research aiming at comparing functional recovery and outcome between right and left stroke patients with neglect has been lacking. In this study, no significant differences were found in daily gain or motor or overall improvement during the entire rehabilitation in-stay between right and left stroke subgroups with equally mild neglect. These 2 subgroups were comparable, since time from stroke onset to admission and length of stay in rehabilitation were similar. At discharge, rehabilitants with left stroke had higher cognitive-communicative disability, but no significant differences were found in motor or overall disability between the 2 neglect subgroups.
In the only previous study primarily aiming at comparing functioning between populations with unilateral left or right hemi-neglect, left neglect was found to be more frequent and severe than right, while motor and cognitive functioning (cognitive ability, communication, motor strength, mobility, and self-care) were largely equal in these 2 groups at admission and discharge. Physical independence at admission was similar in rehabilitants with left, right and no neglect; however, at discharge equal in the 2 neglect groups, but lower than in the no neglect group. The equal improvement in the 2 neglect groups is in accordance with our results. In our population, however, the rehabilitants with mild neglect, whether in connection with right or left stroke, reached proportionally the same level of recovery as those without neglect, but they needed a longer rehabilitation in-stay to accomplish the result. Our results cannot be directly compared with this past retrospective research because of several differences in the populations studied; in the previous study, 29% of the 31 rehabilitants with right and 53 with left hemi-neglect had ipsilateral or bilateral neglect compared with our population with only contralateral lesions, the left-sided neglect was more severe than in our population, length of stay was not reported, and patients with problems in understanding were excluded (10).
Previous studies on neglect have concentrated on comparing patients with and without neglect, especially in association with right stroke. In our population, those with neglect, especially the most disabled left stroke subgroup, had a higher improvement rate (FIM efficiency) and overall recovery (effectiveness) than those without neglect. However, when considering the significant differences in admission functional level between the 4 subgroups, the overall improvement (corrected FIM effectiveness) was largely similar in all subgroups, but those with neglect needed a more lengthy hospitalization to reach the goal. The mean time from stroke onset was equal in all 4 subgroups allowing comparisons. At discharge, despite the lengthy rehabilitation the rehabilitants with neglect were still more disabled, had more restrictions in several motor and cognitive domains and in ADL, more falls, and were more often institutionalized or needed assistance at home.
Interestingly, in a recent retrospective study including 27 rehabilitants with unilateral neglect and 33 with no neglect, those with right or left stroke and neglect had similar FIM effectiveness scores, but lower than rehabilitants without neglect. The mean length of stay was significantly longer than in our study, but a higher initial CBS score predicted a shorter length of stay (for those institutionalized), which reduces effectiveness in the neglect groups. In addition, the admission neglect severity was higher in both right and left stroke groups than in our population. Comparisons are also difficult because their results were not corrected for functional level (in the current study corrected effectiveness was calculated), and in multiple regression analysis the rehabilitants with right and left stroke were combined (28). It is noteworthy that most of our patients (54.3%) had mild neglect at admission, significantly fewer moderate (11.6%), severe (6.9%) or no neglect (27.2%). Irrespective of stroke side, the correspondence of neglect severity with other measures of functioning (activities and body functions) at discharge was moderate to strong. This is in agreement with previous findings of a correlation between neglect severity and NIHSS or FIM (13, 14, 29).
Our findings of more severe disability, attenuated rehabilitation stay, falls and greater need for service after discharge are largely in agreement with previous findings among patients with neglect compared with those without, based on studies in populations with right stroke (4, 5, 11, 13, 30, 31) or in mixed populations with stroke on either side (3, 16). In subacute rehabilitation, functional gain and rate of improvement has been reported to be lower in those with neglect (30), and even lower in those with more severe neglect (3, 13). With worse (3, 4) or comparable (5, 10) admission functional capacity those with neglect have been found to progress more slowly. Specific neglect treatment has been shown to enhance recovery, but the functional gain was still lower and prognosis worse compared with those without neglect (30). On the contrary, a similar gain and rate of improvement has been found in patients with right stroke and neglect compared with those without neglect, in spite of the lower admission functional status (31) as in the current study in the right stroke subgroups. Even a higher total gain has been reported in rehabilitants with neglect compared with those without in a population with right stroke (6) or in a mixed population with either right or left stroke (32), but the patients with neglect needed a longer stay in rehabilitation. This might have been the case also in our population if the in-stay of rehabilitants with neglect would have been even longer.
Limitations
There are some limitations to this study. The number of participants was limited, even if adequate for the purpose of the study. The study was conducted in only 1 facility; thus, the results may not be representative of all in-patient stroke rehabilitants or stroke survivors in general. A long-term follow-up was not performed, so the current study cannot predict the prognostic role of neglect after the subacute rehabilitation phase. Because of limited rehabilitation ward capacity, some patients were transferred to a general ward with rehabilitation recommendations, with the aim of a possible community discharge some weeks later, and were not followed in this study. When comparing the results of the current study with those of studies using conventional paper and pencil tests to assess neglect, the current population probably includes more rehabilitants with mild neglect, as the functional assessment used in the current study is more sensitive to detect neglect. FIM may not capture all consequences of neglect, but it has been widely used and accepted as a tool that evaluates functional ability throughout the rehabilitation process. In addition, we did use other validated instruments and no data were missing despite the large number of variables in this prospective study.
Conclusion
Mild neglect did not impair recovery in patients with right or left stroke, but rehabilitants with neglect were more disabled and they needed a longer rehabilitation in-stay to reach the same functional improvement as those without neglect.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize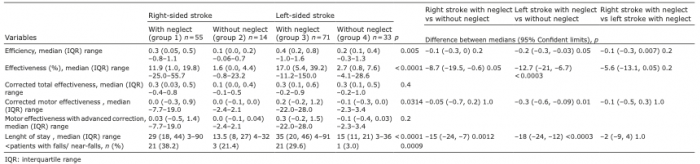 Click to show fullsize
Click to show fullsize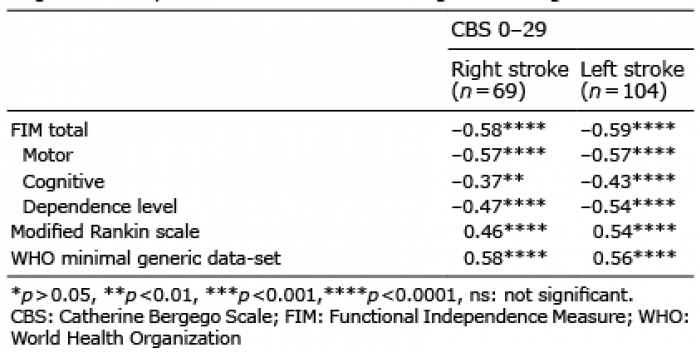 Click to show fullsize
Click to show fullsize