
From the 1Department of Rehabilitation and Brain Trauma, Division of Clinical Neurosciences, Turku University Hospital and University of Turku, 2Department of Expert Services, Turku University Hospital, and 3Department of Biostatistics, University of Turku, Turku, Finland
Objective: To examine the clinical and functional characteristics associated with contralateral spatial neglect in right compared with left subacute stroke, and to investigate the correlations between neglect severity and stroke severity, functional ability and outcome.
Methods: Cross-sectional study comparing neurological impairment and disability. The same data-set was used in part 2 of this study.
Results: Contralateral neglect was present in 79.7% of right stroke and 68.3% of left stroke rehabilitants, and was, on average, equally mild. Left stroke rehabilitants with neglect had higher stroke severity, cognitive and total disability and dependence level and more impaired sphincter control than right stroke rehabilitants with neglect, while the occurrence of depression, motor and sensory impairment was similar. Rehabilitants with neglect, irrespective of stroke side, had higher stroke severity, cognitive, motor and total disability and dependence level than rehabilitants without neglect.
Conclusion: In left and right stroke rehabilitants with equally mild neglect, those with left stroke had higher stroke severity, cognitive and total disability and dependence level. Neglect severity correlated with right or left stroke severity and functional ability, moderate to severe neglect correlated significantly more with functioning. Neglect severity was independently associated with functional outcome in right stroke.
Key words: clinical characteristics; functioning; inpatient; outcome; subacute rehabilitation; severity; spatial neglect; stroke laterality.
Accepted May 18, 2020; Epub ahead of print June 2, 2020
J Rehabil Med 2020; 52: jrm00072
Correspondence address: Sinikka Tarvonen-Schröder, Division of Clinical Neurosciences, Turku University Hospital, PO Box 52, FI-20521 Turku, Finland. E-mail: sinikka.tarvonen-schroder@tyks.fi
Contralateral spatial neglect (inattention) occurred in 79.9% of rehabilitants with right and 68.3% of those with left stroke at admission to rehabilitation, and was, on average, equally mild. Rehabilitants with left stroke and neglect had higher stroke severity and higher cognitive-communicative and overall disability and dependence level and more impaired sphincter control than those with right stroke and neglect, while the occurrence of depression, and motor and sensory impairment was largely similar. Rehabilitants with neglect, irrespective of stroke side, had higher stroke severity and higher cognitive, motor and overall disability than those without neglect. Neglect severity was related to right or left stroke severity and functional ability, moderate to severe neglect was significantly more related to functioning. Neglect severity was independently related to functional outcome in rehabilitants with right stroke.
Stroke is a leading cause of functional impairment worldwide. Annually, approximately 16.9 million people have their first stroke (1, 2). Approximately one-third of stroke patients present lifelong disability (2, 3). Hemi-spatial neglect is a complex and puzzling syndrome, defined as a failure to attend to the contralateral side of personal, peri- or extra-personal space (4). In a recent national registry study neglect was found in 30% of all stroke patients admitted to hospital (5). Among stroke rehabilitants the occurrence has been found to increase to 80% (6, 7), being most common in the immediate post-stroke and subacute phase (7, 8) and usually more common and severe after right compared with left brain damage (4, 7, 9–11), although in different studies the occurrence varies widely, depending on the methods used to assess neglect, the criteria applied in patient selection including age, and the time after stroke onset (4, 10, 12). Even if up to 77% of left brain-damaged stroke rehabilitants have been found to show at least some behavioural neglect (4), most studies on neglect have concentrated mainly on right-sided brain lesions (6, 13), or some studies have been conducted in mixed populations with lesions on either side (7, 8, 14–16). In these studies hemi-spatial neglect has been linked with higher stroke severity and high motor, sensory and cognitive impairment and disability in activities of daily living (ADL) (5, 7, 8, 17–21). However, little is known about left stroke with neglect (14), and studies aiming at comparing clinical and functional differences between right and left stroke patients with neglect are lacking. In addition, the correlations between severity of neglect and both neurological impairment and disability level require clarification (22).
In order to extend previous stroke research on the correlation of spatial neglect with various clinical and functional factors and their connection with stroke laterality, the aim of this study was to investigate the clinical characteristics and functional ability in ADL associated with right and left subacute stroke with and without neglect, and, secondly, to investigate the correlation between contralateral neglect severity and stroke severity, functional ability and outcome in right and left stroke.
A total of 173 consecutive, previously independent, patients, aged over 16 years, with first-ever, radiologically confirmed, unilateral, either right or left hemispheric stroke, were included in this cross-sectional study between August 2015 and February 2019. The patients were mostly referred to the neurological rehabilitation unit from the acute stroke unit of the same university hospital. Sometimes the patient had to wait after the acute stroke unit care on a general ward for stabilization of the medical condition before intensive rehabilitation, or due to lack of capacity of the rehabilitation unit. Because of the intensive programme and high costs of multidisciplinary rehabilitation it is necessary to assess which patients are most suited for admittance to inpatient rehabilitation ward and which patients would be better taken care of at home with possible outpatient therapies or in a skilled nursing facility (23, 24). For admission to our rehabilitation ward, patients had to be able to sit in a wheelchair for a minimum of 30 min.
A multidisciplinary team evaluation included assessments made by a neurologist, a physiotherapist, an occupational therapist, a speech and language therapist, a neuropsychologist, a social worker, a rehabilitation planner, rehabilitation nurses and, when necessary, also other consultants. Intensive comprehensive inpatient rehabilitation programme consisted of combined coordinated meetings with these rehabilitation specialists 5 days a week according to patients’ individual needs, in addition to constant daily rehabilitative nursing.
Exclusion criteria were: current major medical, neurological or psychotic condition, in addition to stroke (n = 1), patients with infra-tentorial or bilateral lesions or with a radiological finding of a previous stroke or other brain damage or with brain injury without radiological findings (n = 55), those with ipsilateral (1 patient with right hemisphere infarct) or bilateral (n = 3) neglect, delay in admission to rehabilitation from stroke onset over 1 year (n = 2), and medical reasons for interrupted rehabilitation (n = 5).
Demographic variables
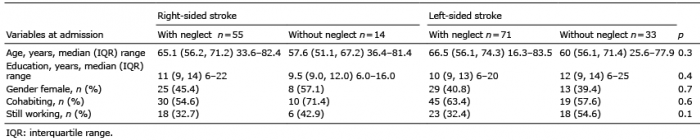
Demographic data, including age, sex, marital status, educational level and working status, were collected (Table I).
Table I. Demographic data of the four rehabilitant subgroups.
Independent variables
The independent admission variables included, firstly, neglect (presence and severity) as the main variable and, secondly, other independent variables that can affect functioning: type of lesion (infarction vs haemorrhage), stroke severity, severity of paresis and aphasia, presence of sensory impairment, apraxia and depression, time since stroke onset, number of comorbidities, Charlson Comorbidity Index (Table II). Clinical data (e.g. 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) diagnosis, date of diagnosis, date of admission and discharge, 24 h National Institutes of Health Stroke Scale (NIHSS) score after possible thrombolysis and/or thrombectomy, comorbidities) were collected from the hospital patient charts. The total number of comorbidities was counted, a procedure previously used to categorize comorbidities (25), and the Charlson Comorbidity Index was calculated (26). The presence of depression and apraxia were based on the clinical judgement of the team.
Scales
An occupational therapist assessed the level of possible spatial neglect of each rehabilitant at admission, using the Catherine Bergego Scale (CBS). The CBS is a measure of functional neglect in spontaneous behaviour in personal, peri- and extra-personal space. It is based on direct observation of 10 real-life situations, i.e. grooming, dressing, eating, mouth cleaning, gaze orientation, knowledge of limbs, auditory attention, moving (collisions), spatial orientation, and finding personal belongings. It captures mild neglect better than traditional paper-and-pencil tests. A total score of 1–10 is classed as mild, 11–20 moderate, and 21–30 severe neglect (4, 27, 28).
A neurologist assessed the neurological status of subjects, including the NIHSS score at admission. The NIHSS is a scale of key components of a standard neurological examination used to assess stroke severity from 0 to 42 (“normal functioning” – “coma”). Total scores 1–4 mean mild, 5–15 moderate, 16–20 severe, and 21–42 very severe stroke (29).
Functional variables
Functional variables included admission FIM total score and motor and cognitive sub-score, dependence level, domain scores, and FIM item scores main locomotion and stairs separately (Table III). The discharge FIM total score was chosen as the main outcome variable because it covers a large number of items and measures outcome in stroke (Tables III, V and VI).
FIM instrument
As part of our formal rehabilitation programme, a rehabilitation nurse, trained and accredited in accordance with Uniform Data System standards as a Functional Independence Measure (FIM®) rater, assessed the level of functioning of each rehabilitant at admission and discharge using an electronic FIM tool (FIM® version 5.2, Amherst, NY, USA). The FIM is a measure of physical and cognitive disability and dependence in 18 items, including 4 motor (self-care, sphincter control, transfer and locomotion) and 2 cognitive (communication and social cognition) domains. The domain locomotion consists of the items main locomotion and stairs. Each item is measured on a 7-point scale, ranging from 1 (total assistance) to 7 (complete independence). The total score ranges from 18 to 126, motor sub-score from 13 to 91, and cognitive sub-score from 5 to 35 (http://udsmr.org).
Participants signed a written informed consent. The same data-set was used in part 2 of this study (30). A proportion of the participants were also included in a previous study (31).
The ethics committee of the University of Turku and Turku University Hospital approved the study (19.5.2015, 73/2015). The ethical standards of the World Medical Association Helsinki Declaration of 1975, as revised in 1983, were followed.
Statistical analysis
Categorical variables were described using frequencies and percentages and, for continuous variables, medians with range of values and interquartile range (IQR) percentiles were used. Comparisons between the 4 rehabilitant subgroups for continuous variables were carried out using the non-parametric Kruskal–Wallis test, and, for pairwise comparisons, the Mann–Whitney U test with Bonferroni correction was used. Difference on Hodges-Lehmann estimate for median difference was used. With categorical variables comparisons between subgroups were assessed with χ2 test, or, in the case of small cell frequencies, Fisher’s exact test. Spearman’s correlation coefficient was used to test the correlation between CBS score, varying from 0 to 29 in the present study, and, firstly, NIHSS score and, secondly, FIM total score, motor and cognitive sub-score and dependence level at admission. When examining the significance of the mild vs moderate to severe neglect on neurological and functional status, we chose to selectively include only the rehabilitants with neglect (CBS ≥ 1). Correlations of 0–0.29 were considered weak, 0.30–0.49 moderate, 0.50–0.69 strong, and 0.70–1.00 very strong. Among rehabilitants with neglect (CBS ≥ 1), linear associations between discharge FIM total score and variables potentially having an impact on outcome were investigated. The factors found to have a significant bivariate association with discharge FIM score were included as independent variables in a linear multiple regression model with discharge FIM score as a dependent variable. Residuals were checked to justify the analysis. Possible multicollinearity was checked; correlation coefficient ≥ 0.8 and/or tolerance value
Of the 173 consecutive stroke rehabilitants who fulfilled the inclusion criteria, 126 (72.8%) were affected by contralateral neglect, 79.7% of those with right and 68.3% of those with left stroke. Of those with neglect, neglect was mild in 65.4% of those with right, and 81.7% of those with left stroke, moderate in 20.0% and 12.7%, and severe in 14.5% and 5.6%, respectively. Four subgroups were formed, those with right-sided stroke with (n = 55) and without (n = 14) neglect and those with left-sided stroke with (n = 71) and without (n = 33) neglect. No statistically significant differences were found in demographic data between the 4 subgroups (Table I).
Clinical characteristics and functioning of the 4 subgroups with significant between-group differences are shown in Tables II and III. Rehabilitants with right and left stroke had, on average, equally mild neglect (CBS median 5 in both subgroups), but those with left stroke had a more severe stroke and lower FIM total score and cognitive sub-score including lower score in the FIM domains sphincter control, communication and social cognition and higher overall dependence level. No differences were found between the 2 neglect subgroups in FIM motor sub-score or motor domain or item scores. The occurrence of depression, sensory impairment, presence and severity of paresis and ambulatory ability were largely similar in the 2 neglect sub-groups, but aphasia and apraxia were more common in those with left stroke. Compared with those without neglect, rehabilitants with neglect, irrespective of stroke side, had a more severe stroke, more often sensory impairment, paresis and more severe paresis, less often ambulatory ability, and higher overall, motor and cognitive disability.
Table II. Clinical characteristics of the four rehabilitant subgroups with between-group differences using Kruskal-Wallis test. Difference on Hodges-Lehmann estimate for median difference. All pairwise comparisons are Bonferroni corrected.
Table III. Functioning assessed with FIM of the four rehabilitant subgroups with between–group differences using Kruskal-Wallis test. Difference on Hodges-Lehmann estimate for median difference. All pairwise comparisons are Bonferroni corrected.
Spearman correlations between neglect severity (CBS score at admission, range 0–29, median 3, n = 173) and stroke severity (admission NIHSS) and level of functioning and dependence (admission FIM) in those with right (n = 69) or left (n = 104) stroke are shown in Table IV. Moderate to very strong correlations were found.
Table IV. Spearman’s correlation coefficients between neglect severity (CBS 0–29) and measures of stroke severity (NIHSS) and functioning (FIM) at admission
In further analysis, mild neglect (left and right CBS range 1–10, median 3, n = 94) correlated slightly more strongly with admission NIHSS (Spearman r 0.35, p = 0.0005) than with FIM total score (r –0.28, p = 0.007), but moderate to severe neglect (left and right CBS range 11–29, median 16, n = 32) correlated significantly more strongly with FIM (r –0.46, p = 0.009) than with NIHSS (r 0.23, p = 0.2). When analysing the 2 sides separately, the corresponding correlations of mild neglect with FIM and NIHSS in right stroke (median CBS 3, n = 36) were r –0.22, p = 0.20 and r 0.38, p = 0.02, and in left stroke (median CBS 4, n = 58) r –0.27, p = 0.04 and r 0.31, p = 0.02, respectively, and of moderate to severe neglect in right stroke (median CBS 16, n = 19) r –0.64, p = 0.003 and r 0.16, p = 0.52 and in left stroke (median CBS 16, n = 13) r –0.49, p = 0.09 and r 0.42, p = 0.15, respectively.
Results of bivariate linear regression analysis between discharge FIM total score and neglect severity (admission CBS score range 1–29) and potential confounding factors in right and left stroke separately are shown in Table V. Age, stroke severity, functioning (FIM), severity of neglect and paresis, presence of apraxia and depression, time since stroke and Charlson Comorbidity Index were found to be associated with discharge FIM total score. CBS score was found to explain 41.9% of the variance of the discharge FIM total score in those with right and 17.3% in those with left stroke; the corresponding figures for admission FIM total score were 64.1% and 69.0%, respectively.
Table V. Results of bivariate regression analysis between admission neglect severity and other potential factors affecting outcome (discharge FIM total score)
Multiple linear regression analysis was applied to test the association between discharge FIM total score and variables significantly associated with FIM in bivariate analysis (Table VI). Admission functional ability, age and time since stroke onset were found to be independently associated with outcome in both neglect subgroups, severity of neglect in those with right stroke and presence of depression in those with left stroke and neglect. No significant multicollinearity was found. The factors significantly associated with FIM in multivariate analysis explained 79.8% of the variance of discharge FIM score in rehabilitants with right and 81.2% in those with left stroke.
In addition, associations between length of stay as a dependent variable and the above-mentioned variables potentially affecting outcome (Table V) were investigated: of the variables associated with length of stay in bivariate analyses (severity of neglect, admission FIM motor or total score, education, 24 h and admission NIHSS and severity of paresis), education, admission FIM motor or total, and admission NIHSS score were independently associated with length of stay in both right and left stroke, but not neglect severity (CBS≥1). Spearman correlations coefficients between CBS≥1 and length of stay analysed separately in the 3 discharge categories (home without or with service or institutionalized) and in the entire population (n = 173) were 0.09, 0.14, 0.15 and 0.24, respectively.
Table VI. Results of multiple linear regression analysis with the variables significant in bivariate analysis for FIM total score at discharge
The occurrence of neglect in the rehabilitant population in this study was high in both right and left stroke (79.7% vs 68.3%), almost as high as in a previous study using a battery of tests to detect neglect (85% vs 77.3%) (4). This is not surprising, as CBS has been found to be a more sensitive method to assess neglect than any single paper-and-pencil test (4). Even if the mean level of neglect in the current study population was equally mild in both right and left stroke, more moderate and severe cases of neglect were found among those with right stroke. The finding of higher occurrence and more severe cases in association with right compared with left stroke is in agreement with previous studies (4, 7, 9–11).
When comparing the clinical and functional differences between the 2 subgroups with neglect, rehabilitants with left stroke had a more severe stroke and higher cognitive and total disability and dependence level, but no significant difference was found in motor or sensory functions or the presence of depression. Aphasia and apraxia were significantly more common in those with left brain damage; it is noteworthy that difficulties in communication explain a large part of the FIM cognitive sub-score besides social cognition. In the only previous study primarily aiming at comparing functioning between populations with unilateral left or right hemi-neglect, left neglect was found to be more frequent and severe than right neglect, while motor and cognitive functioning (cognitive ability, communication, motor strength, mobility, and self-care) was largely equal in these 2 groups. Physical independence at admission was similar in rehabilitants with left, right and no neglect. The results of the current study cannot be directly compared with this retrospective study, because of several differences in the populations studies; in the previous study, 29% of 84 rehabilitants, 31 with right and 53 with left hemineglect had ipsilateral or bilateral neglect compared with the current study population with only contralateral lesions, the left-sided neglect was, on average, more severe than in our population, physical independence was similar in rehabilitants with left, right or no neglect at admission to rehabilitation, and patients with problems in understanding were excluded (11). Nevertheless, the previous finding of physical sequelae in functioning and independence being largely comparable in rehabilitants with mild left- and right-sided hemi-neglect is in agreement with our results.
Past studies on neglect have concentrated on comparing patients with neglect to those without neglect, especially in connection with right stroke. Hemi-spatial neglect has been linked with higher severity of stroke and more severe motor, sensory and cognitive impairment and disability in ADL (5, 7, 8, 17–21). The findings of the current study show that this applies to both right and left stroke: those with neglect had a more severe stroke, more often sensory impairment, paresis and more severe paresis, less often ambulatory ability, and higher overall, motor and cognitive disability and dependence level in daily activities than those without neglect.
Neglect appeared to be mild in most of our rehabilitants (74.6% of those with neglect), significantly less often moderate (15.9%) or severe (9.5%). Irrespective of stroke side, the correspondence of neglect severity with stroke severity (NIHSS) was strong to very strong, and with functioning (FIM) moderate to strong. On closer analysis, in both right and left stroke moderate to severe neglect (CBS >10) correlated significantly more strongly with FIM than with NIHSS; mild neglect (CBS 1–10), on the other hand, correlated slightly more strongly with NIHSS. Moderate to strong correlations have also been found previously between neglect and both FIM and NIHSS (20, 22, 31). In a previous study, neglect correlated slightly more strongly with FIM than with NIHSS during the first year post-stroke (22), which is in agreement with our finding concerning moderate to strong neglect (CBS >10). As CBS is a more sensitive method to detect neglect than conventional assessments used in the previous study, milder cases of neglect were most probably included in our population than in the previous study; this is also supported by the fact that the mean severity of stroke was lower in our population. Nevertheless, the stronger correlation of more severe neglect with FIM than with NIHSS can be seen as an indication that clinically significant neglect influences functional outcome. In accordance with this assumption is the fact that attentional training for disabling neglect has been found to improve functional independence (behaviour), but not neurological status (33).
In agreement with the wider literature (34, 35), the current study found that admission functional status, age and time (delay) from stroke onset to rehabilitation were independent predictors of discharge functional ability, and this applied to both neglect subgroups. Previous research has shown that admission FIM score is the single most significant predictor of outcome (36) and FIM variance at discharge (32). In a previous study among patients with right stroke, neglect severity was shown to be an independent predictor affecting functional recovery (31). Recently, unilateral neglect has been included in a predictive outcome tool for rehabilitants with severe stroke (34). In the current population, especially in those with right stroke, neglect severity predicted independently discharge functional status, but not length of stay, which may be a more biased outcome variable by dependency on, for example, domestic situation and organization of rehabilitation services. Of the neglect subgroups, those with right stroke had milder degree of stroke severity and disability than those with left stroke, but the mean neglect severity was equal in the 2 subgroups; thus, the impact of other factors than functional ability, such as neglect severity, may potentially explain a greater proportion of the outcome in those with right stroke. In addition, the right stroke subgroup had more cases with clinically significant moderate to severe neglect (34.5% vs 18.3%) although the mean severity of neglect did not differ between the 2 subgroups. Advanced age has also previously been found to be a risk factor for poor functional outcome after stroke (36–38), but also for the presence and severity of neglect (12). In accordance with the results of depression being a predictor of outcome in the subgroup with left stroke and neglect, previous research has shown that depression was associated with outcome and was more common in those with left stroke (39).
Study limitations
This study has some limitations. Although the number of participants was limited, it was adequate for the purpose of this research. In addition, no data were missing in this prospective study. Although a wide range of consecutive patients, with severity levels varying from NIHSS 0–22 and FIM 18–126, were included in the study, the most and the least disabled patients were not admitted to intensive inpatient rehabilitation, which narrows the generalizability of the results to the entire stroke population. In addition, rehabilitants with first-ever unilateral hemispheric lesions in one facility only were included; thus, the results may not be representative to all stroke rehabilitants. The application of cross-sectional study design does not allow confirmation of causal relationships of disability, i.e. whether they are based on the disease itself or its secondary consequences. When comparing the current results with studies using conventional paper-and-pencil tests to assess neglect, the current population probably includes more rehabilitants with mild neglect, as the functional assessment used in the current study is more sensitive to detect neglect. The FIM may not capture all consequences of neglect, but it covers the most important ADL and is widely accepted as a functional tool in stroke rehabilitation.
Conclusion
When comparing right and left stroke rehabilitants with equally mild neglect those with left stroke had higher stroke severity and higher cognitive and total disability and dependence level. Rehabilitants with neglect, irrespective of stroke side had not only higher stroke severity and higher cognitive and total disability and dependence level, but also higher motor disability than those without neglect. Severity of neglect correlated with right or left stroke severity and functional ability, moderate to severe neglect significantly more with functioning. Severity of neglect was independently associated with functional outcome in rehabilitants with right stroke.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize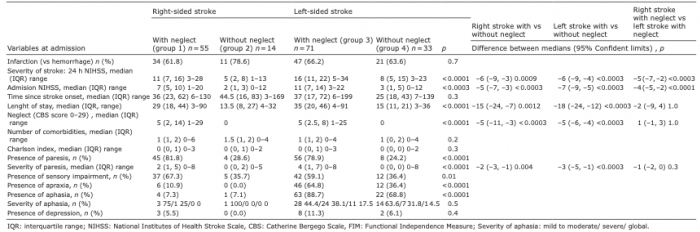 Click to show fullsize
Click to show fullsize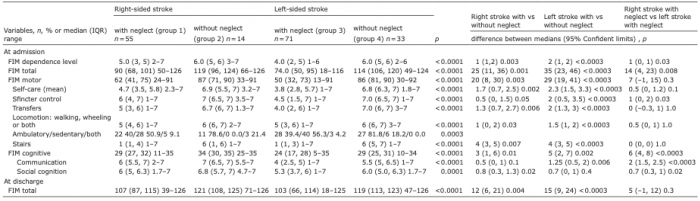 Click to show fullsize
Click to show fullsize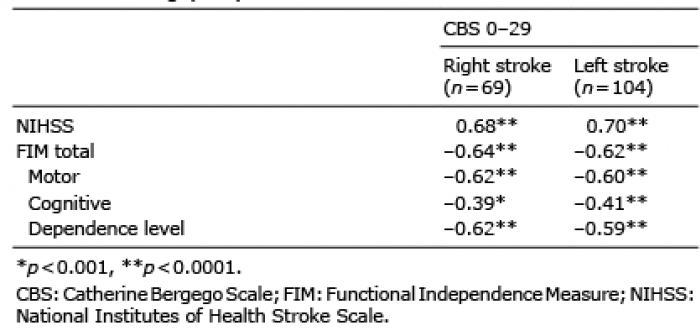 Click to show fullsize
Click to show fullsize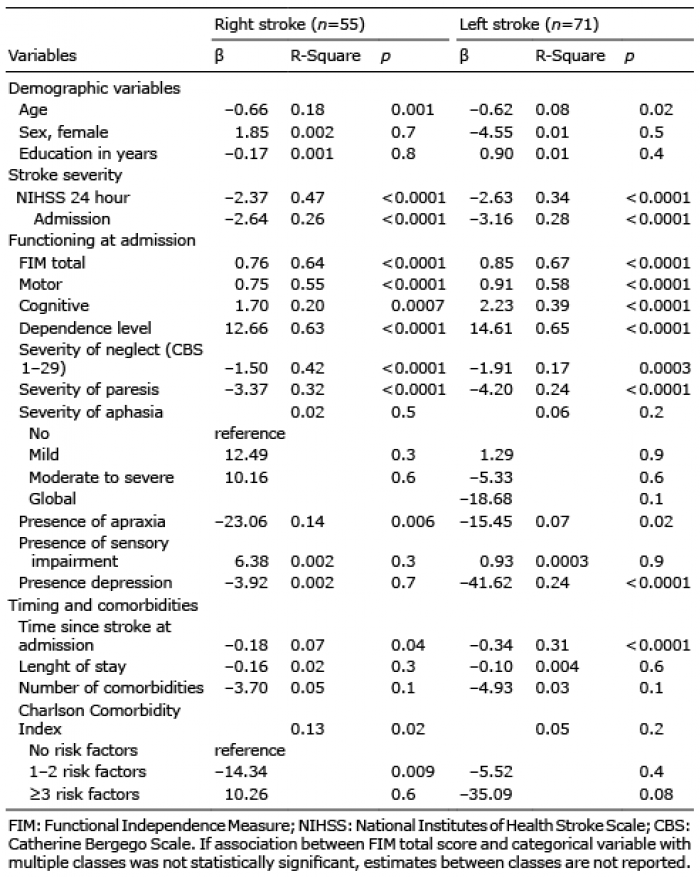 Click to show fullsize
Click to show fullsize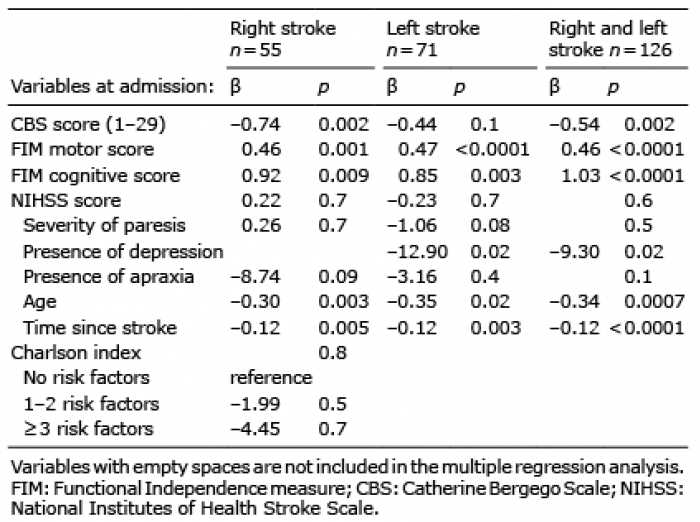 Click to show fullsize
Click to show fullsize