
From the 1Department of Health Sciences, Lund University, Lund, 2The PRO-CARE Group, School of Health and Society, Kristianstad University, Kristianstad, 3Department of Neurology, Rehabilitation Medicine, Memory Disorders and Geriatrics, Skåne University Hospital, Lund, Sweden
Objective: To determine how much people with late effects of polio are bothered by various impairments and their influence on everyday life.
Design: A mixed-methods design.
Subjects/patients: Seven women and 7 men (mean age 70 years) with late effects of poli.
Methods: Self-reported Impairments in Persons with late effects of Polio (SIPP) scale and face-to-face interviews. In SIPP, the participants rated, from 1 (not at all) to 4 (extremely), how much they had been bothered by late effects of polio-related impairments. Qualitative data were analysed using systematic text condensation. Each quotation was deductively analysed based on its conceptual representation regarding perceived influence on everyday life.
Results: Participants were most bothered by muscle and/or joint pain during physical activity, muscle weakness and general fatigue, which corresponded with the number of interview quotations. The impairments negatively influenced daily life, such as household chores, walking, riding a bicycle and social participation. Increased impairments and reduced functioning on the less-affected side also caused worry and distress.
Conclusion: Common late effects of polio-related impairments greatly affected participants’ activity and participation. By using both the SIPP scale and face-to-face interviews, an increased understanding of how late effects of polio-related impairments influence everyday life was achieved.
Key words: fatigue; pain; muscle weakness; psychological distress; activities of daily living; post-poliomyelitis syndrome; rehabilitation.
Accepted Jun 3, 2020; Epub ahead of print Jun 11, 2020
J Rehabil Med 2020; 52: jrm00084
Correspondence address: Catharina Sjödahl Hammarlund, Box 157; SE-221 00 Lund, Sweden. E-mail: catharina.sjodahl_hammarlund@med.lu.se
The aim of this study was to explore how much people with late effects of polio are bothered by various impairments and their influence on everyday life. Fourteen participants (7 men), mean age 70 years, participated. Face-to-face interviews and the Self-reported Impairments in Persons with late effects of Polio (SIPP) scale were used. In the SIPP, the participants rated how much they were bothered by their impairments, from 1 (not at all) to 4 (extremely). The interview data were coded with regard to the meaning of living with late effects of polio-related impairments. Each quotation was conceptually integrated with the SIPP ratings. Muscle and/or joint pain during physical activity, muscle weakness and general fatigue were perceived as most bothersome. The impairments, including the less-affected side, negatively influenced daily life, which caused worry and distress. The interviews complemented the SIPP ratings and improved our understanding of how late effects of polio-related impairments influence everyday life.
Many people who contracted acute paralytic polio in their childhood experience new or increased impairments several decades later, referred to as late effects of polio (LEoP) (1). These impairments typically involve muscle fatigue, muscle weakness, pain at rest and/or during activities, cold intolerance, generalized fatigue, dysphagia, as well as respiratory and sleep problems (1–3). These new and/or increased impairments may negatively influence life satisfaction (2), since the ability to walk and perform social activities and other everyday tasks may become affected (4–7).
One rating scale that can be used to assess perceived impairments in people with LEoP is the Self-reported Impairments in Persons with late effects of Polio scale (SIPP) (8). The SIPP consists of 13 items assessing how much people with LEoP have been bothered by their impairments during the past 2 weeks. The terminology used in these items correspond to components of body function in the International Classification of Function, Disability and Health (ICF) (9). SIPP has shown good psychometric properties in terms of construct validity and internal consistency (8), test-retest reliability with negligible measurement errors, and the ability to detect changes in self-reported impairments over time (10), making it well suited to the target population.
Although SIPP covers common LEoP-related impairments, there are still limitations to our understanding of how these impairments are perceived and how they influence everyday life, which may be contextual or related to special circumstances, that could be overlooked. Using a qualitative approach makes it possible to elaborate on each impairment using follow-up questions, and enables participants to report their experiences more fully. Thereby, using a mixed-methods approach with both a rating scale and interviews may provide a deeper understanding of how LEoP-related impairments influence everyday life among people with LEoP.
The aim of this study was to explore how much
people with LEoP are bothered by various LEoP-related impairments and their influence on everyday life, using a mixed-methods approach.
Research design
This study used a mixed-methods design based on qualitative in-depth interviews using a semi-structured interview guide to explore the participants’ perspectives of their impairments, and quantitative data from the SIPP scale (8). Quantitative and qualitative methods target different aspects, which may provide a broader perspective and deeper understanding of how much people with LEoP are bothered by various LEoP-related impairments and their influence on everyday life. The present study was part of a larger project aiming at understanding the experiences of ageing with LEoP (5) and the occurrence of falls and fear of falling (11). In the current study, only data on the participants’ perceived impairments and their influence on everyday life were included.
Participants
The Regional Ethical Review Board in Lund, Sweden approved the study (Dnr: 2014/186). The principles of the Declaration of Helsinki were applied and all participants gave their written informed consent after receiving written and oral information about the study.
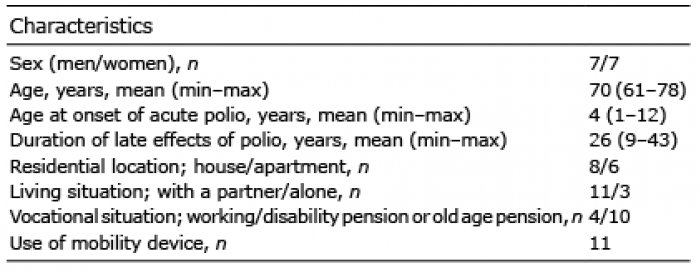
Seven men and 7 women were strategically selected (12) from a larger sample of people with LEoP (13). Their mean age was 70 (range 61–78) years and their mean age when contracting acute paralytic poliomyelitis was 4 (range 1–12) years. All participants had experienced a stable period of at least 15 years before developing clinically verified LEoP. The mean duration of LEoP was 26 (range 9–43) years. Eleven participants were cohabitating, 4 were working and 10 had either part-time disability or old age pensions. Most of the participants used mobility aids whilst walking (Table I).
Table I. Characteristics of the 14 participants with late effects of polio (LEoP)
Qualitative interviews
Face-to-face interviews were held in a rehabilitation clinic, which was familiar to the participants, in southern Sweden. The interviews lasted in mean 70 min (range 60–90 min) and were conducted by 2 of the authors (CSH, CB). Each interview started with an opening sentence: “The aim of this interview is to better understand how people with LEoP experience ageing and consequences of impairments following LEoP”. The interview guide included areas of interest such as: (i) managing everyday activities in the current life situation; and (ii) living with a disability following LEoP. All interviews contained follow-up questions such as: “Can you give an example?” and “Could you elaborate on this subject?”. All interviews were recorded and transcribed verbatim.
Ratings with the SIPP scale
The items in the SIPP scale cover 13 impairments perceived by persons with LEoP (muscle weakness, muscle fatigue, muscle and/or joint pain during physical activity and at rest, sensory disturbance, breathing difficulties at rest and during physical activity, cold intolerance, general fatigue, sleep disturbances, concentration difficulties, memory difficulties, and mood swings (irritability, anxiety, and feeling depressed)) (8). These items represent typical impairments of LEoP, as well as impairments indirectly associated with LEoP. The participants rated how much they had been bothered by each impairment during the past 2 weeks, using the following response options: 1 = not at all, 2 = a little, 3 = quite a bit, and 4 = extremely. The questionnaire was posted to the participants and completed before the interview. The results of the questionnaires were analysed after the interviews in order to avoid the interviews being influenced by the information.
Analysis
Systematic text condensation (STC) was used to analyse the data, as this method is well-suited to cross-case analysis. STC originated from Giorgi’s descriptive phenomenological approach, exploring the lived experiences of the respondents. The analysis consists of several steps of decontextualizing the data, systematically condensing the text into codes and meaning units. In the final steps of the analysis, the recontextualized data gives the abstracted meaning of the cross-case analysis a broad representation of the respondents (14).
First, the interview transcripts were read several times to identify and categorise primary themes that were related to perceived impairments or their impact on everyday life. Meaning units were identified, and the content was formulated into codes that represented the essence of the data. Next, the coded data were organized into subcategories by their conceptual representation and the gist was formulated into aspects representing the content. The subcategories were then organized into categories.
Each quotation was then deductively analysed from its representation with regard to the perceived impairment or the impact on everyday life. Each quotation that matched one of the items in SIPP received the corresponding number. Thereafter, all data from SIPP (i.e. how much the participants had been bothered by various impairments) were analysed using descriptive statistics and the results of each item and response category were presented as absolute and relative numbers (%).
RESULTS
Representation of the items in SIPP and corresponding qualitative data
Items that the participants rated as most and least bothersome. Nearly all participants were quite a bit or extremely bothered by muscle and/or joint pain during physical activity. Many also described that they were quite a bit bothered by muscle weakness and general fatigue. In contrast, most participants reported that they were not at all bothered by breathing difficulties at rest, or concentration difficulties and memory difficulties. All data regarding the participants’ ratings of SIPP are shown in Table II.
Table II. A description of how much people with late effects of polio (n = 14) have been bothered by various impairments according to the Self-reported Impairments in Persons with late effects of Polio (SIPP) scale
Deductive analysis
The highest representation with regard to the number of statements [in brackets] was general fatigue [38], muscle weakness [32] and muscle fatigue [27]. During the interviews, none of the participants reported being bothered by sensory disturbances (item 5) or memory difficulties (item 12). Therefore, these items are not included in the results. The results of the deductive analysis presented below follow the order of the items in the SIPP.
Muscle weakness (item 1). Nearly everyone rated their muscle weakness as causing quite a lot of problems. Muscle weakness in the lower limbs hampered physical activities, such as being able to go for a walk or riding a bicycle. The weakness also affected their balancing ability, and uneven surfaces could become challenging. Muscle weakness in the upper limbs also affected leisure activities; for example, painting, doing needlework or in practical situations, such as not being able to open a jar.
…to open a jar or something like that…. To get the lid off the jar that’s… I don’t think that I have enough strength in my hands… my fingers have become weaker… [P9]
The interviews revealed that muscle weakness also involved the less-affected side, which further limited participating in various activities. Feeling increasingly weaker and not being able to rely on the less-affected side were perceived as disturbing.
Strangely enough, I feel that my left leg, which is the so-called healthy leg, often becomes tired. But I feel that it’s that leg that I feel often gets tired now and it’s not as strong as it used to be. I haven’t had any problems with it before, but during the last 5–6 years my strength has declined considerably. [P7]
Muscle fatigue (item 2). Almost half of the participants reported that they were extremely or quite a bit bothered by muscle fatigue. In addition to decreased functioning, they felt that the “healthy” side fatigued more easily compared with before. It had become more evident that muscle fatigue also involved the whole body. The less-affected side, previously regarded as supportive and reliable, had now become less functional.
…it’s when walking longer distances…I avoid that…It becomes obvious just after some hundred meters that my legs become fatigued, and after that it becomes worse and worse the more you walk…. [P11]
Muscle and/or joint pain during physical activity (item 3). Nearly all participants were extremely or quite a bit bothered by muscle and/or joint pain during physical activity. They described how they had become increasingly limited due to pain in their joints and muscles, which now more frequently also involved the less-affected side. Being aware that physical activity would result in pain also meant that they avoided participating in such activities.
Well, I’ve noticed that it’s become a lot tougher over the last years. I’ve had more pain, more ache in my joints… [P2]
I can’t move around as much as I would have wanted to. I feel that I’ve become more tired and I get more pain if I, for example, walk further than I did six months ago. It really bothers me that I’m no longer able to do that… [P7]
Muscle and/or joint pain at rest (item 4). Most participants were not at all bothered by muscle and/or joint pain at rest. They believed that taking a rest was necessary to continue with their daily activities. However, those who were extremely and quite a bit bothered by muscle and/or joint pain at rest, felt that sleep was disturbed due to pain, especially in their hands and feet.
When I come home, I have to go to bed to lay down and rest, sleep for an hour, to manage… [P2]
Breathing difficulties at rest (item 6). Nearly all participants reported having no difficulties with breathing at rest. Those who felt short of breath and experienced problems in getting air into their lungs, described this as a most frightening experience.
…. you feel scared when you can’t get enough air into your lungs and it’s hard to breathe…. It felt like I couldn’t get up and I couldn’t get any rest either. [P8]
Breathing difficulties during physical activity (item 7). A few participants reported that they were quite a bit bothered by breathing difficulties during physical activity. They felt that they managed quite well if they could do things at their own pace. However, walking upstairs or uphill was difficult and could make them feel short of breath.
…well, I don’t think… what really is my problem is when I walk up the stairs or up hills, then I become a little short of breath… [P14]
Cold intolerance (item 8). Some participants reported that they were extremely or quite a bit bothered by cold intolerance. They were aware of their cold intolerance and tried to manage as best they could, especially during wintertime, for example by using extra blankets. Others disregarded their cold intolerance, which had become worse over time, as they continued to put pressure on themselves to continue as before.
I had more pain and became more tired and more intolerant to cold, but I’ve always been a person who wants to be on top of things and always putting pressure on myself and I had a hard time to accept the situation, quite frankly. [P12]
General fatigue (item 9). Half of the participants reported that they were quite a bit bothered by general fatigue. It felt like a sudden, profound loss of energy that completely drained the body of both physical and mental energy. The impact of this feeling was impossible to resist and it could just hit you at any time without warning.
It’s impossible to describe this tiredness, it just hits you and you become incredibly tired. It’s a feeling which doesn’t compare to being physically tired. It’s a strange tiredness that appears occasionally. [P5]
It just feels like, all your energy just vanish, sort of like you collapse or something like that…. [P14]
Sleep disturbances (item 10). Some participants reported that they were extremely bothered by sleep disturbances. Some found that it was difficult to fall asleep and that they needed medication to do so. Others woke up every now and then due to pain and aches in their muscles and joints. They also felt increased pain from the less-affected leg, which woke them up quite frequently.
I sleep very poorly and I need to take sleeping pills at times… [P8]
I rarely sleep through a whole night, I don’t. I often wake up due to pain and ache in my hands and feet…. [P5]
Concentration difficulties (item 11). A few reported having quite a bit of concentration difficulties. The participants described that it was important to concentrate whilst walking. In order to plan how to keep going forward and keep their balance, they needed to concentrate on every step they were taking to avoid falling, which was perceived as exhausting.
It takes a lot of determination and energy when concentrating on how to move forward, which naturally becomes worse if there’s a lot of people around…. [P5]
Mood swings (item 13). Some participants reported having quite a bit of mood swings. They stressed more easily in various situations and worried about not getting to appointments in time or about catching a bus or a train. Feeling generally stressed had become worse over time. They also worried about falling and hurting the less-affected leg, the one they depended on. The risk of hurting oneself was frightening, as the consequences of not managing were daunting. Some also felt that they had lost their energy and spark and they felt as if nothing was functioning.
I’ve fallen a couple of times and that’s what you’re afraid of… actually. What you fear the most is that then you may break the leg that’s most intact… or to break the leg that’s not functioning, that’s just as bad…. [P7]
I lost a bit of my spark when I felt that it’s not functioning. [P10]
This mixed-methods study has provided a deeper understanding of how self-reported impairments influence daily life in persons with LEoP. To the best of our knowledge, this has not been explored previously among people with LEoP. According to the ratings in the SIPP, the impairments that the participants were most bothered by were muscle and/or joint pain during physical activity, muscle weakness and general fatigue. Impairments that the participants were least bothered by were breathing difficulties at rest, concentration and memory difficulties, which are impairments that are commonly reported and indirectly associated with LEoP (8). Deductive analysis showed that general fatigue [38], muscle weakness [32] and muscle fatigue [27] had the highest representation with regard to the number of statements [in brackets]. The participants described that increased general fatigue, muscle
weakness and muscle fatigue contributed to making daily life more difficult; for example, carrying out daily chores and limited their participation in social activities. Another important finding was that several of these impairments had increased over time and now also engaged the less-affected side. The distress that was brought on from realizing that the “healthy” side was no longer reliable and functioning was considerable. Worrying about not being able to manage everyday activities and fear of losing one’s independence was noticeable. These concerns, which have been reported previously, must be considered when designing rehabilitation interventions (5).
General fatigue, muscle weakness and muscle fatigue were often mentioned in the interviews and the participants’ ratings in the SIPP showed that they were quite a bit and extremely bothered by these impairments. These impairments, as well as joint and muscle pain, have previously been reported as the most common in persons with LEoP (2, 15–17). The many quotations regarding general fatigue were in line with other studies, which have shown that this impairment is common and results in more pain, lower physical function and decreased vitality (18–20). However, the participants found it difficult to describe what it meant to have general fatigue. They felt that it occurred suddenly with an overwhelming loss of energy that drained the body totally of both physical and mental energy. It was impossible to resist, control or even predict, as it could just hit them at any time without warning. This description of fatigue was in line with a previous study, associating fatigue with impaired cognitive and/or physical functioning (21).
Muscle weakness impeded physical activities, such as going for a walk or riding a bicycle, but also other activities, such as managing household chores, as the weakness also affected hands and arms. This result confirmed a previous study, which found that muscle weakness in the upper limbs can lead to problems when performing activities, especially tasks above the head or heavy duties (4). In addition, muscle weakness also affected the participants’ balance, which limited their activities, and environments were not as available anymore to the participants, also reported previously (22–24).
Muscle weakness and pain were impairments that the participants were quite a bit bothered by, which has been reported previously (4, 25, 26). The participants felt increasingly limited due to pain in their joints and muscles, which engaged the less-affected side more frequently. Being aware of getting pain after physical activity also meant that they avoided activities in general. Pain has previously been reported to be common among people with LEoP affecting physical and psychological functioning (15, 18, 20, 27), which was in line with the findings in our study.
The results also showed that muscle weakness and pain were often present during physical activities; for example, walking. It has been shown previously that muscle strength in various muscle groups in lower limbs is important for walking ability and gait speed (28, 29). Since knee flexion during weight acceptance serves to reduce the impact of the reaction forces, the loading rate becomes increased. By walking at a slower self-selected speed, energy cost and the influences of reaction forces may be reduced (29, 30). These walking characteristics resulting from weak muscles, in particular quadriceps weakness, may explain the consequences of overuse exposure and additional pain in people with LEoP. Avoiding overuse of weak muscles in order to prevent adverse effects has been suggested previously (31).
Some participants found that muscle and/or joint pain at rest was quite bothersome, mainly for their sleep, as reported previously (15). Some reported that it was difficult to fall asleep, whereas others woke up quite frequently. Sleep problems have been reported previously as more common than in our study (32). It may also be associated with breathing difficulties during the night (31, 32) and at rest, which our participants described as a most frightening experience. Those who felt short of breath when walking upstairs or uphill, managed quite well if they could do things at their own pace. In a previous study of people with LEoP, the risk of shortness of breath was higher among women than among men (33).
The participants in the present study reported having quite a bit of mood swings and felt worried. They stressed more easily in various daily situations and worried about not making things in time, and feeling generally stressed had become worse over time. The participants also felt nervous about falling and hurting the less-affected leg that they depended on. The fear of hurting a body part was frightening, as the consequences of not managing was daunting. Some also described that they had lost their energy and spark when they felt as if nothing was functioning. Increased worries and anxiety may be related to the challenges of ageing and struggling with new impairments. Such emotional reactions need to be considered when designing rehabilitation interventions (5). A previous study has described an individualized, goal-oriented, comprehensive interdisciplinary rehabilitation programme, introducing self-management strategies and several interventions to maximize each individual’s physical, mental and social potential (34). The results of this programme showed reduced perceived disability due to improved self-confidence, acceptance and sense of control (34).
Clinical implications
SIPP is a psychometrically sound scale covering the most common impairments in people with LEoP. With face-to-face interviews we have broadened and improved our understanding of the impact of the LEoP-related impairments on everyday life. Furthermore, the reduced functioning in the less-affected side caused emotional reactions of worry, fear and general stress, underlining the importance of understanding the impact of each of the impairments on mental stress, activity and participation. This understanding might be helpful for clinicians when designing targeted rehabilitation interventions. In a clinical setting, we therefore suggest using a rating scale with predefined questions to assess impairments as a support for a face-to-face interview, to better understand the meaning of impaired functioning and the consequences for activity and participation in daily life.
Strengths and limitations
The strategically selected participants provided rich and relevant data, which provided valuable insight into the consequences of living with LEoP. As a precaution, we did not analyse the data from the SIPP before interviewing the participants, thereby avoid being influenced by these results. The authors worked individually during the process of coding the data. In order to maintain reflexivity, we had continuous discussions during the analysis to stay aware of our preunderstanding. Furthermore, to add transparency and trustworthiness to our findings, we have added the participants’ code number after each quotation to show the representation of our participants (35). With regard to transferability, none of the participants mentioned having sensory disturbances or memory difficulties in the interviews, impairments considered to be indirectly associated with LEoP, which may not be representative of all people with LEoP.
Conclusion
The participants were most bothered by muscle and/or joint pain during physical activity, muscle weakness and general fatigue, which corresponded with the high number of quotations in the interviews. Increased impairments and reduced functioning in the less-affected side brought on worry and distress. The consequences of the LEoP-related impairments involved reduced physical functioning and social activities, as well as restricted participation. The SIPP scale may be valuable as a guide for structured interviews mapping out perceived impairments, whereas the interviews provide a deeper understanding as to how they influence everyday life. By using both the SIPP scale and face-to-face interviews, an increased understanding of how LEoP-related impairments influence everyday life was achieved. This knowledge could be important for clinicians in order to provide targeted rehabilitation interventions to people with LEoP.
The authors wish to thank all participants for their cooperation. The study was supported by the Gyllenstierna Krapperup Foundation, Sweden, Stiftelsen för bistånd åt rörelsehindrade i Skåne, Sweden, the Department of Health Sciences at Lund University, Lund, Sweden, and the Faculty of Medicine at Lund University, Lund, Sweden.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize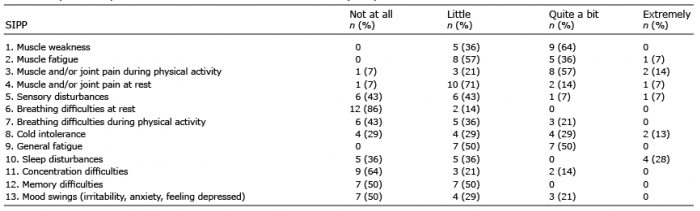 Click to show fullsize
Click to show fullsize