
From the 1Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), Institute of Health and Society, Faculty of Medicine, University of Oslo, 2Department of Physical Medicine and Rehabilitation, Oslo University Hospital, Oslo, Norway, 3Department of Family Medicine and Population Health, Division of Epidemiology, Virginia Commonwealth University, Richmond, VA, USA, 4Department of Rehabilitation Medicine, Hannover Medical School, Hannover, Germany, 5Department of Rehabilitation, University Hospital of North Norway, 6Department of Clinical Medicine, Faculty of Health Sciences, UiT, The Arctic University of Norway, Tromsø, 7Institute of Clinical Medicine, Faculty of Medicine, University of Oslo and 8Institute of Nursing and Health Promotion. Oslo Metropolitan University, Oslo, Norway.*These authors contributed equally.
Objective: To determine how health-related rehabilitation services have been described in recently pub-lished randomized clinical trials, using the International Classification System for Service Organization in Health-Related Rehabilitation (ICSO-R 2.0) as a framework.
Methods: Medline was searched for English--language randomized clinical trials (RCTs) published between
1 January 2018 and 31 December 2018. RCTs were eligible if the primary goal was to provide rehabilitation services to targeted patient populations. Two authors independently screened and extracted data, and assessed the methodological quality of eligible trials. Descriptive analysis was used to compare service descriptions between eligible trials and the ICSO-R 2.0 framework (23 categories, 9 categories for provider, 14 categories for delivery).
Results: Twenty-nine RCTs, with a wide range of organizational units and target groups, were included. The median number of categories reported in the provider dimension was 4 (range 3–5). The median number of categories reported in the service delivery dimension was 8 (range 6–12). None of the RCTs described all ICSO-R recommended categories.
Conclusion: Descriptions of service organization in rehabilitation varied widely among recently publish-ed randomized clinical trials. Use of the framework for the classification of service organization and standardization of description of services is recommended in future RCTs, to facilitate better comparisons in service research across studies.
Key words: rehabilitation; health service; clinical trial; international classification; International Classification System for Service Organization in Health-Related Rehabilitation.
Accepted Aug 3, 2020; Epub ahead of print Aug 18, 2020
J Rehabil Med 2020; 52: 000093
Correspondence address: Nada Andelic, Research Centre for Habilitation and Rehabilitation Models and Services (CHARM), Institute of Health and Society, Faculty of Medicine, University of Oslo, Oslo, Norway. E-mail: nada.andelic@medisin.uio.no
The aim of this review was to determine how health--related rehabilitation services have been described in randomized controlled trials published in 2018, using the International Classification System for Service Organization in Health-Related Rehabilitation (ICSO-R 2.0) as a framework. A total of 29 randomized controlled trials that met the inclusion criteria were identified. The description of service organization in rehabilitation varied widely among recently published randomized controlled trials. None of the randomized controlled trials review-ed described all ICSO-R 2.0 categories of provider and service delivery. In general, this review found that only half of the recommended categories of provider and service delivery dimensions were reported frequently in the reviewed literature. Future randomized controlled trials should use the framework for classification of service organization and for standardization of descriptions of services, in order to facilitate better comparisons in service research across studies.
Health-related rehabilitation aims to enable people with health conditions experiencing and likely to experience disability to achieve optimal functioning in interaction with the environment (1, 2). Thus, rehabilitation aims to maximize an individual’s ability to live, work, and learn in one’s living environment (3). Rehabilitation services must meet needs at different stages of disease and injury and deliver appropriate rehabilitation and interventions that ensure functional recovery and promote well-being (4, 5). Rehabilitation services are complex and differ in approach and set-up. Variations in service provision also exist due to context (i.e. geographical region, culture and available resources) (6–9). Successful rehabilitation should be person-centred and involve service users, their peers and families at all stages of the process (10). However, services are often developed in an ad hoc way in response to immediate rehabilitation needs within a budget, leading to inequality or lack of consistency in service provision (4). A possible reason for this has been a lack of conceptual models that can be used to guide and classify health-related rehabilitation service provisions in terms of organizational setting, technical and human resources, and goals (11).
The recently developed International Classification System for Service Organization in Health-Related Rehabilitation (ICSO-R) and its revised version (ICSO-R 2.0) aim to provide uniform criteria to describe and classify rehabilitation services at the meso-level of healthcare (i.e. the organization and availability of services) (12–14). The ICSO-R 2.0 consists of 2 dimensions, “provider delivery” and “service delivery”, each with a more extensive list of categories and subcategories that characterize rehabilitation service organization (15). The provider dimension describes the framework of the organizational units, with the primary goal of providing rehabilitation services, and could be applied to describe where, by whom, and in which context the service is delivered (13, 15). The service delivery dimension contains interventions, procedures and devices provided to the service users within the context of the provider, and can be used to describe what and how services are delivered and for what reason (13, 15).
Clinical trials in the field of rehabilitation have been used as evidence-based medical decision-making tools to evaluate treatment effectiveness. In 2020, Gutenbrunner & Nugraha proposed including health system and organization as a fourth factor in the evidence-based medical decision-making process (16). This process considers the health system and organizational factors when evaluating the outcomes of a clinical trial. In clinical trials evaluating rehabilitation service provision, many factors, such as health professionals, facilities, service availability, diagnostic and treatment devices, and other aspects are covered by the ICSO-R 2.0. Therefore, by comparing service descriptions between clinical trials and the framework of ICSO-R 2.0, it is possible not only to provide insight into service provision research, but it is also feasible to appraise service descriptions systematically in the field of health-related rehabilitation. Hence, the aim of this study was to determine how these factors were described in recently published randomized clinical trials (RCTs) in the field of rehabilitation, using the framework of the ICSO-R 2.0.
Literature search and study selection
A Medline search was performed for articles published between 1 January and 31 December 2018, among indexed English-language studies, to identify eligible RCTs in the field of health-related rehabilitation. The search strategy included the following terms:
“rehabilitation” [Subheading] OR “rehabilitation” [All Fields] OR “rehabilitation” [MeSH Terms] AND
“health services” [MeSH Terms] OR (“health” [All Fields] AND “services” [All Fields]) OR “health services” [All Fields] AND
“rehabilitation centre” [All Fields] OR “rehabilitation centers” [MeSH Terms] OR (“rehabilitation” [All Fields] AND “centers” [All Fields]) OR “rehabilitation centers” [All Fields] OR (“rehabilitation” [All Fields] AND “center” [All Fields]) OR “rehabilitation center” [All Fields] AND
“hospitals, rehabilitation” [MeSH Terms] OR (“hospitals” [All Fields] AND “rehabilitation” [All Fields]) OR “rehabilitation hospitals” [All Fields] OR (“rehabilitation”[All Fields] AND “hospital” [All Fields]) OR “rehabilitation hospital” [All Fields] AND
“randomized controlled trial” [Publication Type] OR “randomized controlled trials as topic” [MeSH Terms] OR “randomized clinical trials” [All Fields] OR “randomized clinical trials” [All Fields] AND
2018 [All Fields] AND
Clinical Trial [ptyp].
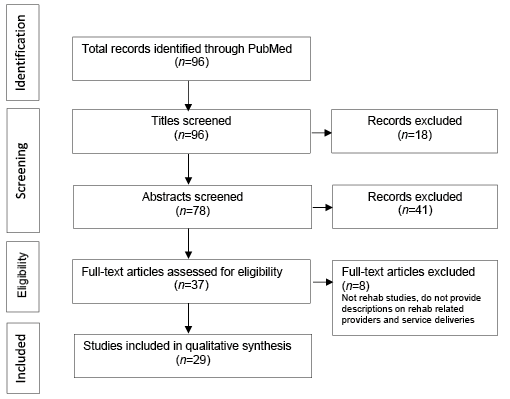
All RCT reports published during the study period were eligible if the primary goal was to report the effectiveness of the rehabilitation interventions, and if the trials comprised rehabilitation programmes or services used in the targeted patient population. The RCTs were excluded if the primary objective was not to provide rehabilitation services. Based on the defined eligibility, 2 authors (NA and JL) independently screened the studies and finalized the study selection. Discrepancies between the 2 authors were evaluated, and a consensus was reached for the results. Fig. 1 presents the study selection process via the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommended flowchart (17).
Fig. 1. Study selection process.
Data extraction
A standardized protocol and a data extraction sheet were developed to extract the relevant information from each original report and compare the data with the provider and service delivery dimensions and corresponding categories, as proposed by ICSO-R 2.0 (15). Prior to the formal data extraction process, the authors (NA and JL) extracted data and studied the concepts of the recommended service description items. All discrepancies were resolved through consensus or through consulting other co-authors.
According to the ICSO-R 2.0, the provider dimension is defined as “organizational units with the primary goal of providing rehabilitation services”, consisting of 9 categories: context, ownership, location, governance/leadership, quality assurance and management, human resources, technical resources, funding of provider, and other categories of provider. The service delivery dimension is defined as the provision of “A set of products (interventions, procedures, devices, and pharmaceuticals, etc.) to a specified group of individuals (patients, informal caregivers, and/or other users and clients), aiming at achieving or maintaining optimal functioning (rehabilitation) within an organizational context (provider)”. This dimension describes the characteristics of service delivery, including 14 categories: health strategies, service goals, target groups, modes of referral, location of services delivery, facility, setting, integration of care, patient-centredness, aspects of time and intensity, rehabilitation team, reporting and documentation, funding of service delivery, and other categories of service delivery. A set of pre-defined inclusion and exclusion criteria is included in 2 ICSO-R 2.0 dimensions for corresponding categories and subcategories (15). The outcome measurements from the selected studies were reported along with the dimensions of the International Classification of Functioning, Disability and Health (ICF) (Body Function, Activity and Participation, and Environmental Factors) (18).
Methodological quality assessment
The methodological quality of all 29 eligible RCTs was assessed independently by 2 authors (NA and JL), with the assessment items set out by Cicerone et al. (19). The original 16 items were developed to assess the quality of RCTs on cognitive rehabilitation in patients with a traumatic brain injury. This study selected 10 items that were relevant to the current study objective:
specified eligibility criteria;
described method of randomization;
concealed treatment allocation;
described interventions;
blinded outcome measurements;
described withdrawal or dropout;
sample size description;
intention-to-treat analysis;
point estimate and variability;
statistical comparison treatment effects.
Based on a total score of 10, the methodological quality was classified as “high”’, “moderate” or “low” for RCTs receiving a score of 9–10, 6–8 or 5 or less, respectively.
Data analyses and synthesis
Data on the characteristics and methodological quality of the eligible RCTs are summarized descriptively, e.g. the continuous variables were summarized as means and standard deviations or medians and ranges, as appropriate, and discrete variables were presented as frequencies and percentages. The information regard-ing the recommended ICSO-R 2.0 service descriptions is presented in tables/figures based on the provider and service delivery dimensions by category and subcategory under each dimension and methodological quality of RCTs. All data analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Characteristics of included randomized controlled trials
A total of 29 eligible RCTs were included in the current review (20–48). Most of the studies (79%) were conducted in hospital settings or independent rehabilitation units. Table I illustrates the descriptive summary of the characteristics of all RCTs. Overall, 21% were pilot RCTs, and 79% were RCTs. A majority of the RCTs (86%) used a parallel design, and the rest were cross-over (10%) or clustered designs (4%). Approximately one-third of the RCTs (31%) were multi-centred studies, and the remainder (69%) were single-centred studies. The target patient groups from these studies were patients with neurological disorders, such as stroke or chronic stroke (62%), musculoskeletal conditions (14%), heart diseases (14%), lung diseases (7%) and elderly patients (3%). The size of the RCTs ranged widely from 15 to 914 subjects. Most of the studies (76%) had fewer than 100 participants. Half of the studies were conducted in Europe (52%). The remaining studies were conducted in Asia (34%) and the USA or Canada (14%). Using the Methodological Quality Assessment criteria (19), 55% of the RCTs were rated as of high methodological quality, 38% were rated as of moderate quality, and 7% of low quality. The details of the methodological quality evaluations are shown in Table SI1.
Table I. Study characteristics (n = 29)
The median number of corresponding provider categories reported by all 29 RCTs was 4 (range 3–5) out of 9 possible categories. The median number of the corresponding service delivery categories was 8 (range 6–12), out of 14 possible categories. A similar pattern was found in median numbers of reported provider and service delivery categories in high-quality studies (4 and 8), and these were somewhat higher than the median numbers reported in moderate-quality studies (3.5 and 7). None of the RCT reports described all ICSO-R recommended categories for either the provider or service delivery dimension.
Report on the provider dimension
Fig. 2 and Table II show provider dimension descriptions from all RCTs compared with the ICSO-R 2.0. Of the 9 possible categories, 1.1 Context and 1.3 Location were described by all trials (100%). The categories 1.6 Human Resources (86%) and 1.7 Technical Resources (79%) were also reported frequently. For the category 1.1 Context, most trials were performed in rehabilitation hospitals, clinics, or centres (55%); multiple settings (17%); or the community (7%). Category 1.6 Human Resources primarily reports different types of healthcare providers, such as physicians, nurses, physical therapists and occupational therapists, among others. Finally, the category 1.7 Technical Resources predominantly includes equipment and infra-structure, such as therapeutic and assistive devices and technical infrastructure.
Fig. 2. Categories of ICSO-R 2.0 at dimension of provider.
Table II. Current rehabilitation-related randomized controlled trial reports vs International Classification of Service Organizations in Rehabilitation (Version 2)’s recommendations regarding descriptions of service providers*
Table II. cont.
Only one study reported public ownership for Item 1.2 Ownership. The assessed trials did not report the following categories:
1.4 Governance/Leadership and its subcategories 1.4.1 Mission, 1.4.2 Vision and 1.5 Quality Assurance and Management;
1.5 Quality assurance and management;
1.8 Funding of Provider and its subcategories 1.8.1 Source of Money and 1.8.2 Criteria of Spending; and
1.9 Other Categories of Provider.
Report on the service delivery dimension
Fig. 3 and Tables III and IV present information from all trials that address the proposed service delivery categories. Out of all 14 categories, the categories 2.2 Service Goals, 2.3 Target Groups, 2.10 Aspect of Time and Intensity, and 2.12 Reporting and Documentation were reported by all RCTs. The categories 2.7 Setting (93%), 2.11 Rehabilitation Team (90%), and 2.13 Funding of Service Delivery (69%) were also reported frequently. The categories 2.4 Modes of Referrals (55%), 2.5 Location of Service Delivery (21%), 2.6 Facility (17%), 2.8 Integration of Care (28%) and 2.9 Patient-Centeredness (52%) were reported less often. Only one of the selected RCTs reported 2.1 Health Strategies (other than rehabilitation), whereas none of the studies reported 2.14 Other Categories of Service Delivery.
Fig. 3. Categories of ICSO-R 2.0 at dimension of service delivery.
Table III. Current rehabilitation-related randomized controlled trial (RCT) reports vs International Classification of Service Organizations in Rehabilitation (ICSO-R) (version 2)’s recommendations on descriptions of service deliveries*
Table III. Cont.
Table IV. Current rehabilitation-related randomized controlled trial (RCT) reports vs International Classification of Service Organizations in Rehabilitation (ICSO-R) (version 2)’s recommendations on descriptions of service deliveries*
Table IV. Cont.
The results show that all studies reported recovery and improvement in functioning or health status as the goals of the services (2.2 Service Goals). Item 2.3.1 Target Group-Health Conditions includes patients primarily exhibiting neurological conditions (62%), including stroke (55%), with an age range of 20–87 years. Only 3 studies directly reported the level of care (2.7.1), either tertiary or secondary. In 2.7.2 Mode of Service Delivery, most services were delivered through inpatient (28%), outpatient (34%), multiple settings (17%) and at home (3%). The most frequent types of care (2.7.3 Phase of Health Care) were post-acute and chronic rehabilitation (58%), followed by acute rehabilitation (14%) and subacute rehabilitation (14%).
The subcategories of rehabilitation teams (2.11.1 Professions) includes physicians and physiotherapists. In addition, 2.11.2 Interaction Approach was described in only 38% of the studies (e.g. multi-professional team (17%) and counselling (14%)). Regarding 2.12 Reporting and Documentation, most primary and secondary outcome measurements could be linked to the body function and body activities of the ICF. Furthermore, 24% of the studies reported measurements of health-related quality of life (HRQL), whereas only one study used an outcome measurement that can be linked to the participation level.
In this review, reports regarding the category 2.13.1 Funding to Service Delivery were mostly related to the sources and modalities of the payment (i.e. research grants for trials (38%) or multiple sources, such as a combination of research grants, state funding and health insurance (31%)). However, 2.13.2 Criteria of Payment was not reported in the studies.
The aim of this topic review was to determine how health-related rehabilitation services were described in RCTs published in 2018, using ICSO-R 2.0 as a frame-work (15). The review identified 29 RCTs that met the inclusion criteria. Considerable heterogeneity in service descriptions is exhibited in the study design and setting, targeted population, and provided interventions in the trials. However, the results indicate that only half of the recommended categories of provider and service delivery dimensions were frequently reported in the reviewed literature.
Concerning the provider dimension, most trials were performed in hospitals or independent rehabilitation units or centres. Few studies were performed in multiple settings. It is challenging to design and conduct multicentre RCTs; therefore, these results are unsurprising. Furthermore, most trials did not report the ownership of the provider (i.e. the legal and contextual characteristics of the owning entity). Both public and private service organizations are important aspects for policymakers and stakeholders, and such characteristics may influence the outcomes (49).
None of the studies reported information regarding the governance/leadership category, which is defined as “political, economic and administrative authority in the management of the provider”, and its corresponding subcategories: mission, vision and involvement in governance and management. Quality assurance and management, funding of provider, source of money, and other categories of provider were not reported. This may reflect the fact that this review captured rehabilitation interventions trials and not trials directly targeting the organizational aspects of rehabilitation services. It cannot be excluded that organizational research is insufficiently covered in Medline, but the scarce body of research in rehabilitation services has also been well documented by the World Health Organization (WHO) (50). The governance and leadership category of service provision has been documented to affect services, the target group choices and treatment programmes (51). However, the extent to which these factors also influence the outcome of rehabilitation interventions and thus are relevant to clinical trials is not clearly documented.
Concerning the service delivery dimension, only one study was identified that focused on health strategieoneother than rehabilitation. Important contextual factors, such as the location of services, were described in only one-fifth of the studies. Most trials addressed post-acute and chronic rehabilitation care phases, whereas only one-quarter of the studies addressed acute/subacute care phases. The limited number of trials from these phases may reflect the practical and ethical restraints imposed on the randomization of severely affected individuals for whom no realistic alternatives to specialist intervention are available (52).
The rehabilitation team category and professions and competencies subcategories were mentioned in the majority of trials, but team interaction and methods of team organization and communication pathways were described less frequently. However, multi-disciplinary team interactions and team members with relevant expertise are suggested as key features of a successful specialist rehabilitation service (52). The other characteristics of successful rehabilitation services, such as integration of care (i.e. timely, comprehensive and well-coordinated care along the continuum of care) and patient-centredness (i.e. rehabilitation tailored to patient needs and shared decision-making) were also less frequently reported categories. The majority of studies that identified these categories were from Europe and the USA or Canada (20, 22, 24, 26, 30, 31, 37, 39–42, 44, 45, 47, 48). This may reflect the conceptual definitions of integration of care and patient-centeredness from these geographical regions (53) or the type of intervention provided in the studies. Further research studies should investigate whether these categories apply to all regions of the world and address various types of rehabilitation trials.
In the reporting and documentation category, which is defined as “health and functioning parameters in individual patient’s records”, primary and secondary outcome measurements were extracted from trials and reported along with the ICF dimensions (18). Most measurements used in the reviewed studies were previously linked to the ICF domains of body functions and activities, whereas only one study reported a participation outcome measurement. One-quarter of the studies reported HRQL measurements. The results regarding the participation domain and HRQL were somewhat unexpected, because the main goal of rehabilitation is to provide people with disabilities with a meaningful existence and a life within their expectations.
The ICSO-R 2.0 was specifically developed to cover rehabilitation services at the meso-level (15), acknowledging the lack of classification systems at this level and the importance of the meso-level in the quality and effectiveness of rehabilitation interventions. The present review indicates some awareness of the service organization (meso-level factors) in studies focused on rehabilitation interventions at the micro-level. How-ever, the distinction between service delivery at the meso-level and the interventions at the micro-level is not always clear, as reported in a recent review by Røe et al. (54). The current review found a similar situation; thus, guidelines or standards for reporting rehabilitation service organization in clinical trials are needed. However, a current version of ICSO-R 2.0 with 23 categories is too extensive for such use and provides categories in clinical rehabilitation trials beyond those reported. Thus, a shorter version of ICSO-R may be considered for minimum reporting standards for service organization in clinical trials.
Study limitations
Several limitations should be considered in interpreting the results. This is a topic review based on a literature search of Medline for 2018 and, thus, can serve only as an initial review of the subject. A further effort with an extensive study period, including a wide range of rehabilitation studies, is recommended to confirm the findings of this study. The current review includes only studies with experimental designs, which may limit the generalizability of the results to studies with other designs, such as longitudinal observational studies. Of all eligible studies, 52% were from Europe, 22% were in the pilot phase, 69% were single-centre studies, and the trial sizes were mostly small. These study characteristics may influence the results of this review. In addition, the generalizability of the study results may be limited by the fact that the majority of the studies were of targeted inpatients with stroke and heterogeneous rehabilitation intervention programmes and designs (e.g. 21% pilot RCTs). The evaluations of the studies may be biased by the outlook and experience of the authors, because the standardized evaluation manuals and value sets of ICSO-R 2.0 are still not developed.
Conclusion
Descriptions of service organization in rehabilitation varied widely among recently published RCTs. None of the reviewed RCTs described all of the ICSO-R 2.0 provider and service delivery categories. Use of the framework in classification of service organization and standardization of descriptions of services is recommended in future RCTs, in order to facilitate better comparisons in service research across studies.
This study was supported by funds from the Institute of Clinical Medicine and Institute of Health and Society, Research Centre for Habilitation and Rehabilitation Models and Services (CHARM) at the University of Oslo, Oslo, Norway.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize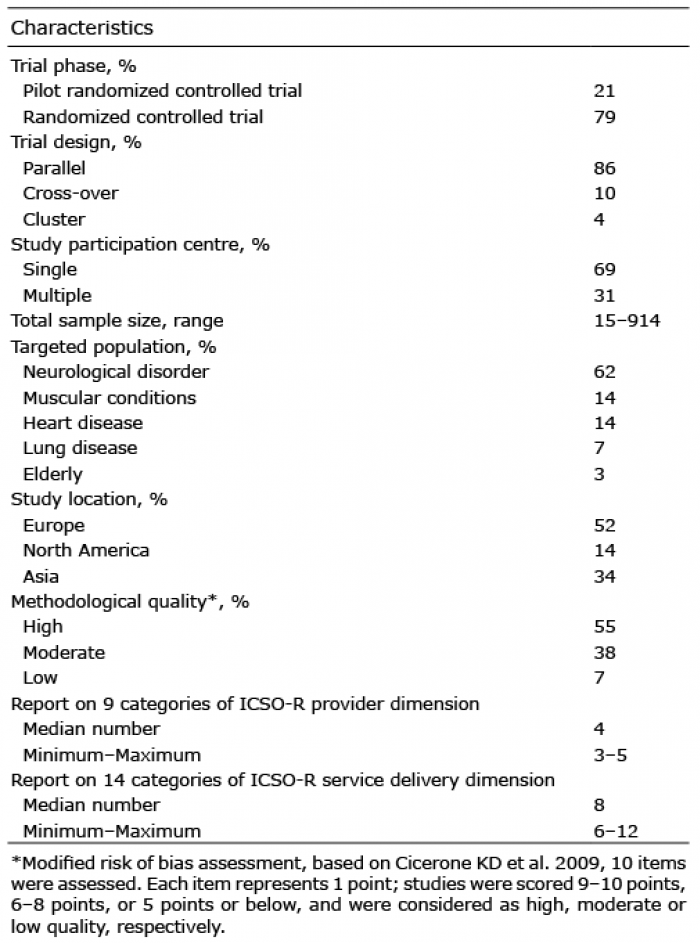 Click to show fullsize
Click to show fullsize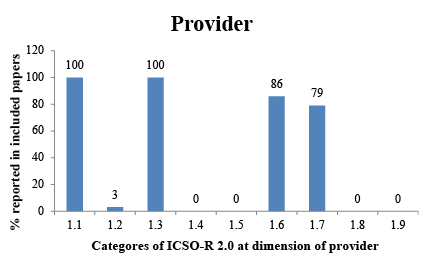 Click to show fullsize
Click to show fullsize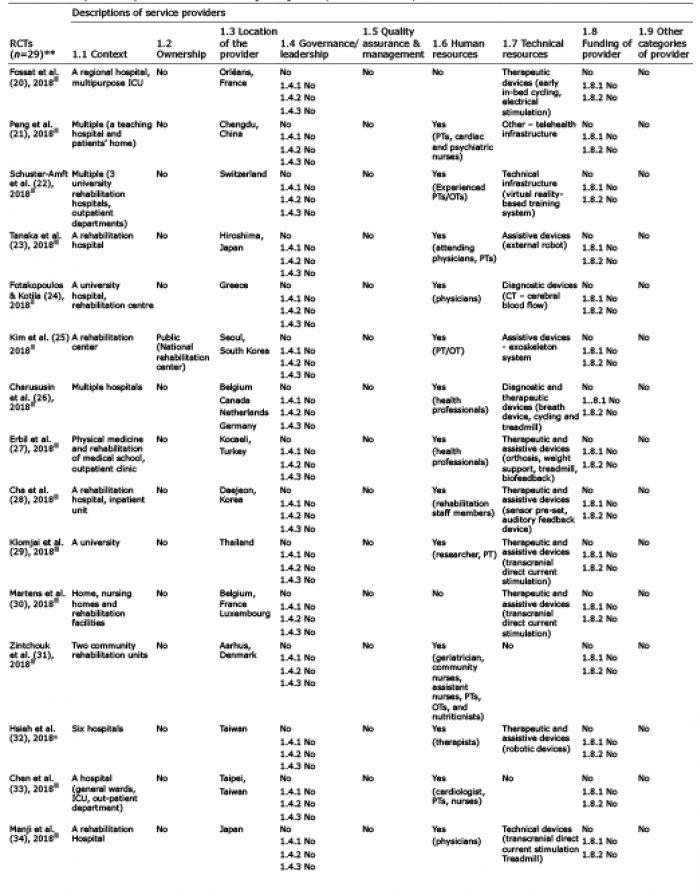 Click to show fullsize
Click to show fullsize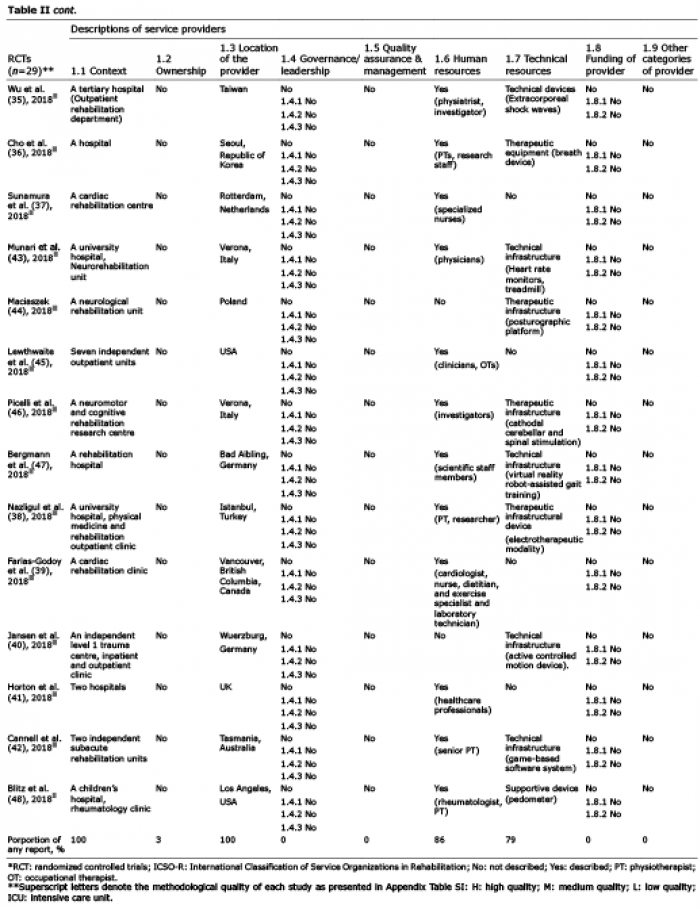 Click to show fullsize
Click to show fullsize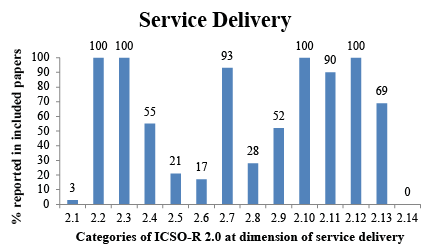 Click to show fullsize
Click to show fullsize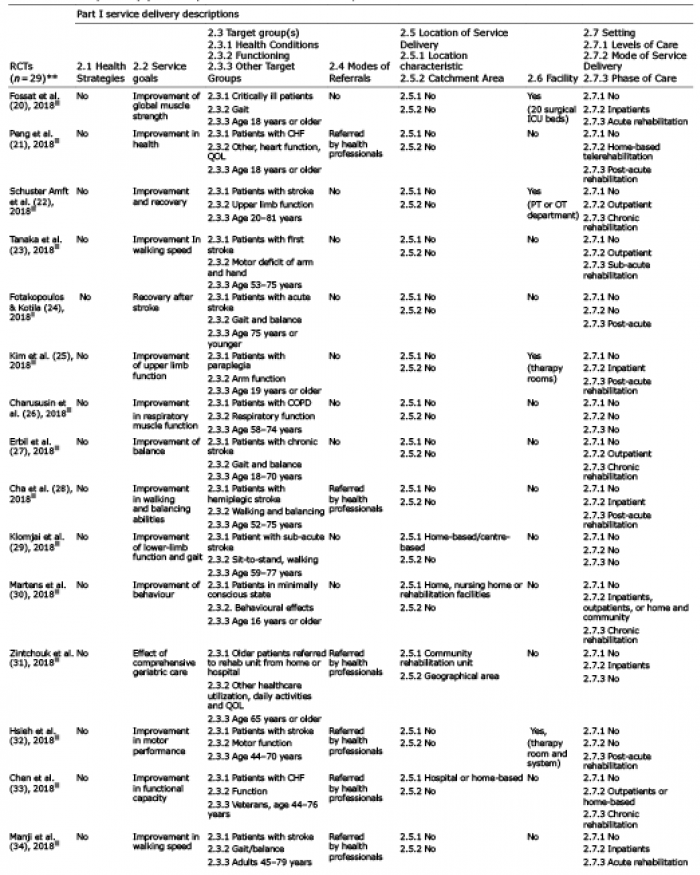 Click to show fullsize
Click to show fullsize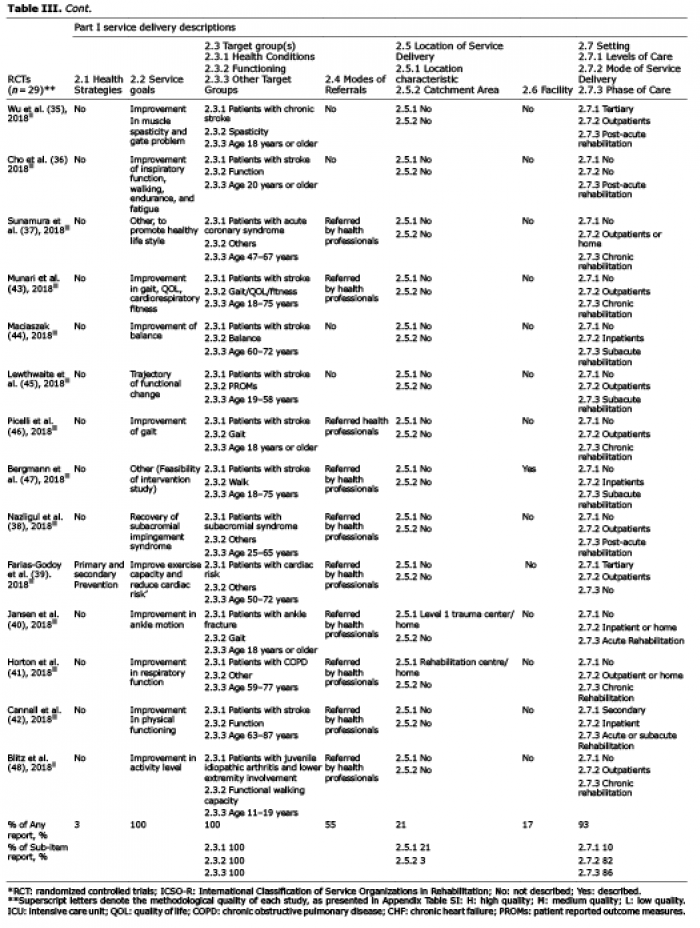 Click to show fullsize
Click to show fullsize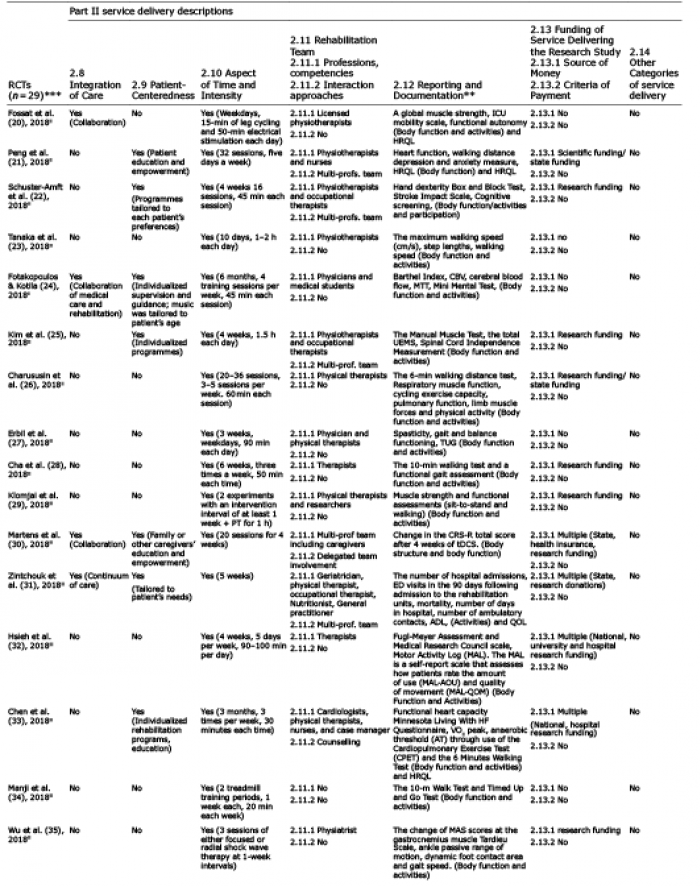 Click to show fullsize
Click to show fullsize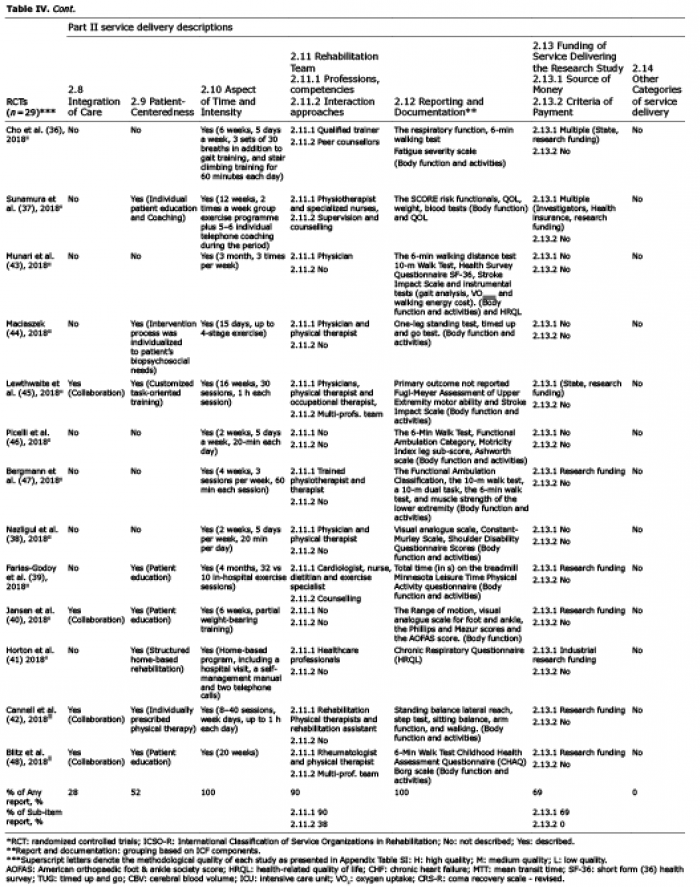 Click to show fullsize
Click to show fullsize