
From the 1Research Department, Sunnaas Rehabilitation Hospital, 2Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Norway, 3Faculty of Health Sciences, University of Sydney, Australia, 4China Rehabilitation Research Center, China, 5Institute of Physiotherapy, Faculty of Health Sciences, OsloMet – Oslo Metropolitan University, Oslo, Norway
Objective: To investigate the effectiveness of self-administered, home-based, upper limb practice in improving upper limb activity after stroke. To compare structured home-based practice vs non-
structured home-based practice.
Methods: Databases were searched for randomized or quasi-randomized controlled trials using a pre-
defined search strategy. Data were extracted from 15 studies involving 788 participants. The quality of included studies was assessed using the PEDro scale.
The studies included an experimental group that received self-administered, home-based practice for upper limb activity limitations of any level of severity and any time after stroke, and a control group that received no intervention, or received non-structured home-based practice. Only measures of upper limb activity were investigated.
Results: Self-administered, home-based practice did not improve activity compared with no intervention (standardized mean difference 0.00, 95% confidence interval; –0.47 to 0.48). There was no difference between structured and non-structured home-based practice in terms of upper limb activity (SMD –0.05, 95% CI –0.22 to 0.13).
Conclusion: Existing self-administered, home-based practice is not more effective than no intervention in improving upper limb activity in chronic, severely disabled stroke survivors. Structured home-based practice is no more effective than non-structured home-based practice.
Key words: home care services; upper extremity; recovery of function; stroke rehabilitation.
Accepted Aug 21, 2020; Epub ahead of print Sep 11, 2020
J Rehabil Med 2020; 52: jrm00118
Correspondence address: Yih Wong, Research Department, Sunnaas Rehabilitation Hospital, Bjoernemyrveien 11, 1453 Bjoernemyr, Norway. E-mail: yihw@uio.no
Doi: 10.2340/16501977-2738
Therapist-supervised, home-based practice early after stroke is known to reduce poor outcome in people with stroke. However, due to limited resources in the community, self-administered, home-based, upper limb practice is often prescribed after stroke. Whether such practice (without therapist supervision) is effective in reducing upper limb activity limitation is unknown. It is also not known whether home-based practice is more effective with or without the use of technology and assistive devices. We reviewed 15 studies involving 788 participants. The findings indicate that, in chronic and severely disabled stroke survivors, self-administered, home-based practice is no more effective than no intervention in improving upper limb activity. Also, home-based practice involving technology and assistive devices is no more effective than home-based practice without such devices. The existing evidence is insufficient to draw a more robust conclusion. Further research is needed to determine the effect of self-administered, home-based practice in these patients.
Stroke is one of the most significant causes of disability worldwide (1, 2). Two-thirds of people have limitations in upper limb activity in the acute phase of stroke (3). Six months later, 30–66% of these people will still have limitations, leading to increased dependence in activities of daily living, restricted social participation, anxiety, low quality of life and poor well-being (4, 5). Thus, finding the best way to continue rehabilitation in the subacute phase in order to improve upper limb activity is paramount (6).
One systematic review reported the beneficial effect of early-supported discharge services in terms of improvement in outcome and reduction in dependency, length of hospital stay, and risk of readmission to hospital compared with clinic-based care (7). Another systematic review of early, therapist-supervised, task-oriented practice in the home found such rehabilitation to be beneficial in promoting independence in activities of daily living compared with no intervention (8). From these reviews, it appears that therapist-supervised, home-based practice is no worse than clinic-based practice when appropriately resourced and initiated early after stroke. However, a systematic review by Coupar et al. found no significant benefit of home-based practice specifically targeting the upper limb in terms of activities of daily living or upper limb activity in comparison with placebo, no intervention or usual care (9). No robust conclusion could be drawn, as the data for the analysis were obtained on the basis of only one study.
Due to limited resources in the community, self-administered, home-based practice is often prescribed to people with physical sequelae after stroke. The possible advantages of home-based practice are flexibility of scheduling, family support, a familiar environment, and reduced travel costs (10–12). However, whether self-administered, home-based practice without the supervision of a therapist is effective in improving upper limb activity after stroke is unknown. Effectiveness may be reduced due to the absence of a therapist to ensure adherence, safety, appropriate dose and progression. Technology and assistive devices provide motivation, feedback or instruction (e.g. gaming, virtual reality, robotics), which can enable people after stroke to perform self-administered training with minimal therapist supervision (12). However, the clinical effects of such highly structured home-based practice compared with non-structured self-administered practice are unclear. The specific research questions investigated in this review were therefore:
1. Does self-administered home-based, upper limb practice improve upper limb activity after stroke?
2. Is structured home-based practice more effective than non-structured home-based practice?
Home-based practice was defined as a programme prescribed by a health professional carried out in the person’s residence consisting of at least 50% self-administered, task-oriented training. The review analysed practice aimed at upper limb activity. Structured home-based practice was defined as a task-oriented programme involving the use of technology and/or assistive devices in providing motivation, instruction or feedback to people after stroke.
Identification and selection of studies
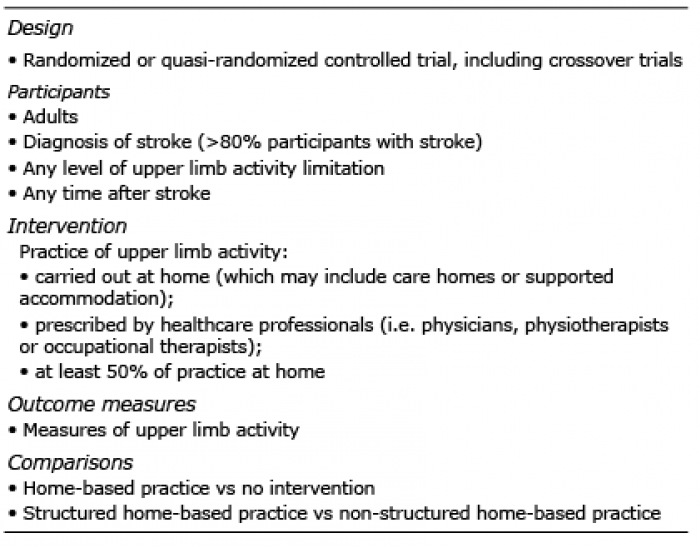
Searches were conducted in the following databases: Medline (Ovid) (1946 to 28 January 2020), Physiotherapy Evidence Database (PEDro) (28 January 2020), ExcerptaMedica Database (EMBASE) (1947 to 28 January 2020), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (1981 to 28 January 2020), Cochrane Central Register of Controlled Trials (CENTRAL) (1966 to 28 January 2020), Allied and Complementary Medicine Database (AMED) (1985 to 28 January 2020), OT-seeker (28 January 2020) and Web of Science (1900 to 28 January 2020) and the first 50 results of Google Scholar (28 January 2020). Search strategies were developed in consultation with the university library specialist at OsloMet – Oslo Metropolitan University (Appendix 1 shows the full search strategy). The searches were restricted to relevant publications in English. Titles and abstracts of identified records were screened by 2 reviewers (YW and RR) to determine full-text articles to be examined. Consensuses were sought through discussion and a third reviewer’s opinion (BL). Subsequently, full-text copies of relevant studies were retrieved and independently assessed by 2 reviewers (YW and LA) against the inclusion criteria in Table I. Any disagreement that occurred between the 2 reviewers was resolved by the third review author (BL). The protocol was registered on the International Prospective Register of Systematic Reviews (identification number CRD42018094863).
Table I. Inclusion criteria
Assessment of study characteristics
Quality. The methodological quality and risk of bias of included studies was assessed using the PEDro scores from the Physiotherapy Evidence Database (www.Pedro.org.au) (13). The scores were obtained from 10 questions pertaining to the internal validity and the statistical information provided in the studies.
Participants. Studies were included if 80% of the sample were adults with stroke. Information, such as sample size, time after stroke, and severity of upper limb activity limitations, was extracted in order to examine the similarity of the studies.
Intervention. To answer the first research question: as to whether self-administered, home-based, upper limb practice improves upper limb activity after stroke, the experimental group had to receive self-administered, home-based upper limb practice and the control group had to receive no intervention. No intervention was defined as nothing and/or small amounts of intervention.
To answer the second research question, as to whether structured home-based practice is more effective than non-structured home-based practice, the experimental group had to receive structured home-based practice and the control group had to receive non-structured home-based practice. Structured home-based practice could be forced use (e.g. constraint-induced movement therapy (CIMT), modified CIMT; feedback (e.g. mirror therapy, gaming, virtual reality, finger tracking, music therapy); or assistive devices (e.g. robotics, orthosis, functional electrical stimulation). Participants could be receiving additional rehabilitation, as long as both groups received the same dose. Dose, frequency and duration of intervention were recorded in order to examine the similarity of the studies.
Outcome measures. Upper limb outcomes according to the International Classification of Functioning, Disability and Health framework (ICF) activity level were used in the analysis. When a study reported more than one relevant outcome measure, the measure selected for meta-analysis was chosen in the following order:
i) Direct observation of performance reported as interval data (e.g. Box and Block Test (BBT), Nine-Hole Peg Test (9HPT), Purdue Pegboard Test (PPT), Wolf Motor Function Test (WMFT)-performance time, Test Evaluant la Performance des Membres supérieurs des Personnes âgées (TEMPA) – speed of execution).
ii) Direct observation of performance reported as ordinal data (e.g. Action Research Arm Test (ARAT), WFMT – functional ability scale, TEMPA – functional rating, Chedoke Arm and Hand Inventory (CAHAI), Arm Motor Ability Test (AMAT), Motor Assessment Scale (MAS)).
iii) Non-observed (interview) of performance reported as ordinal data (e.g. Motor Activity Log (MAL) – amount of use scale, MAL – how well scale).
Consensus about the selection were sought through discussion (YW and LA) and 2 other reviewer’s opinions (BL and GM).
Data collection and analysis
Data were extracted by one reviewer (YW) and verified by a second reviewer (RR). Details of included studies (i.e. study design, participants’ characteristics, intervention and measures) and outcome data (i.e. number of participants, mean and standard deviation (SD)) were extracted. Authors of papers with missing data were contacted. Continuous data are presented as means and SD. If 95% CI from individual groups were reported, SD was re-calculated using the formula: =(upper limit–lower limit)/2*TINV(0.05; n–1)*SQRT(n) in Microsoft Excel. If median and interquartile range were reported, the mean and standard deviation of a sample were estimated by methods devised by Luo et al., Hozo et al. and Wan et al. (14–16).
Post-intervention scores were used to obtain the pooled estimate of the effect of intervention immediately after intervention. Since different outcome measures were used, the effect size was reported as Cohen’s SMD with 95% CI. Heterogeneity was assessed using the I2 statistic. In the case of substantial heterogeneity (I2 > 50%), a sensitivity analysis was carried out to investigate the source of heterogeneity. The fixed-effects model was reported if I2 score was ≤ 50% or there was no difference in means between fixed- and random-effects analyses (17). Subgroup analyses based on the time after stroke and severity of activity limitations were planned a priori if there was a sufficient number of comparable studies. All analyses were performed using Cochrane Collaboration’s Review Manager software, RevMan 5 (18).
Flow of studies through the review
A total of 3,707 records were identified from the search of different electronic databases. After removing duplicates and clearly irrelevant studies, 102 were eventually selected for full-text review. Of these 102 papers, 15 studies were included (Fig. 1; see Appendix 2 for excluded papers).
Fig. 1. Flow of studies through the review. *Papers may have been excluded for failing to meet more than one inclusion criteria.
Characteristics of included studies
Of the 15 studies, 5 investigated home-based practice vs no intervention (19–23) and 10 investigated structured home-based practice vs non-structured home-based practice (24–33). Almost all included studies were individually-randomized parallel-group trials except 2 (27, 33), which were randomized cross-over trials. Additional information was obtained from the authors for one trial (33). A summary of the included studies is shown in Table II.
Table II. Summary of included studies
Quality. The mean PEDro score of the papers was 6.6 out of 10 (range 4–8) (Table III). Most of the included studies: were randomized (100%), had concealed allocation (60%), had similar groups at baseline (100%), had blinded assessors (60%), had <15% dropouts (80%), carried out an intention-to-treat analysis (67%), analysed the between-group difference (100%), and reported point estimates and variability (93%). Blinding of participants and therapists was not possible due to the nature of the intervention.
Quality. The mean PEDro score of the papers was 6.6 out of 10 (range 4–8) (Table III). Most of the included studies: were randomized (100%), had concealed allocation (60%), had similar groups at baseline (100%), had blinded assessors (60%), had <15% dropouts (80%), carried out an intention-to-treat analysis (67%), analysed the between-group difference (100%), and reported point estimates and variability (93%). Blinding of participants and therapists was not possible due to the nature of the intervention.
Table III. PEDro scores of included studies
Participants. The mean time since stroke of participants across the studies ranged from 57 days to 5.6 years, with 12 of the 15 studies (80%) having participants who were more than 6 months after stroke. Most of the participants were moderate-to-severely disabled according to baseline measurements (Table II) .
Intervention. For the 5 studies included in answering the first research question (whether self-administered home-based, upper limb practice improves upper limb activity after stroke), the experimental group received 64–100% of their intervention as self-administered, home-based, task-oriented upper limb practice prescribed by healthcare professionals. The types of home-based practice were: forced use (3 studies), feedback (2 studies). Both groups received 11–36% supervised training (3 studies).
For the 10 studies included in answering the second question (whether structured home-based practice is more effective than non-structured home-based practice), the experimental group received 71–100% structured, home-based, task-oriented upper limb practice prescribed by healthcare professionals, while the control group received the same amount of non-structured, home-based, task-oriented upper limb practice. Types of structured home-based practice were: feedback (6 studies), assistive device (3 studies) and a combination (1 study). Both groups received 17–29% supervised training (3 studies). Non-structured home-based practice was an exercise programme with written instructions and log to record the amount of practice.
The dose varied across studies, with the session length ranging from 20 to120 min, frequency ranging from 3 to 7 times a week, and duration from 2 to 8 weeks.
Outcome measures. The measures chosen for the analysis of upper limb activity were: BBT (6 studies), 9HPT (1 study), PPT (1 study), WMFT-performance time (3 studies), ARAT (2 studies), CAHAI (1 study), and MAL-amount of use scale (1 study).
Effect of home-based practice vs no intervention
The immediate effect of self-administered, home-based, upper limb practice compared with no intervention on upper limb activity was analysed by pooling post-intervention scores from 5 comparisons comprised of 275 participants, using a random-effects model. The mean PEDro score was 7 out of 10. Home-based practice did not improve activity (SMD 0.00, 95% CI –0.47 to 0.48) compared with no intervention (Fig. 2). There was substantial statistical heterogeneity among the studies (I2 = 63%), indicating that the variation between the results of the trials was above the variation expected by chance. No specific reason for the heterogeneity could be identified in the sensitivity analysis.
Fig. 2. Standardized mean difference of the effect of self-administered, home-based practice compared with no intervention on improving activity immediately after the period of intervention by pooling data from 5 trials (n = 275) using a random-effects model (I2 = 63%). 95% CI: 95% confidence interval. *Mean (standard deviation; SD) estimated from median (minimum–maximum).
Effect of structured home-based practice vs non-structured home-based practice
The immediate effect of structured home-based upper limb practice compared with non-structured home-based practice on upper limb activity was analysed by pooling post-intervention data from 10 comparisons comprised of 513 participants, using a fixed-effects model. The mean PEDro score was 6.4 out of 10. Structured home-based practice was no better than non-structured home-based practice (SMD –0.05, 95% CI –0.22 to 0.13, I2 = 0%) (Fig. 3).
Fig. 3. Standardized mean difference of the effect of self-administered, home-based practice compared with non-structured home-based practice on improving activity immediately after the period of intervention by pooling data from 10 trials (n = 513) using a fixed-effects model (I2 = 0%), 95% CI: 95% confidence interval; SD: standard deviation.
This systematic review found that self-administered, home-based, upper limb practice was no more effective than no intervention in improving upper limb activity. Neither was structured home-based practice more effective than non-structured home-based practice. Overall, considering 8 is the maximum PEDro score achievable in trials using complex interventions (since it is not possible to blind the therapists or participants), the mean score of 6.6 suggests that the findings of this review are credible.
An explanation for the lack of difference between the groups may be that home-based practice was performed in the chronic period after stroke. Almost 80% of the studies were conducted in a population more than 6 months after stroke, which raises the question of whether home-based practice would be more effective if performed in an earlier time period. The majority of behavioural recovery occurs within 3 months post-stroke and slowly plateaus after that (34–36). The Stroke Recovery and Rehabilitation Roundtable recommends that this early subacute period is considered a critical window for brain repair processes (37). However, when the studies were sub-grouped according to the time after stroke, there was no support for such a hypothesis. According to this review, there is no significant difference between the groups for both subacute (≤ 6 months) and chronic populations. Self-administered, home-based practice in comparison with no intervention yielded an effect size of –0.20 (95% CI –1.12 to 0.73) in subacute population (1 trial), while in chronic population (4 trials) the effect size was 0.04 (95% CI –0.53 to 0.60).
Eighty percent of the studies involved people who were severely disabled after stroke (i.e. had less than 50% of maximum achievable score of their selected upper limb measures at baseline). Thus, a possible reason for lack of effect may be that there was simply no capacity for improvement in severely disabled people a long time after stroke. After all, the most important predictive factors for upper limb recovery following stroke is the initial severity of motor impairment or function (38). Home-based practice may be effective if applied with less-disabled people. Additional randomized clinical trials are warranted in order to determine the effect of home-based practice in the early subacute period and in less-disabled people after stroke. Also, studies with larger sample size are needed to reduce the level of uncertainty related to the wide confidence intervals regarding the difference between groups.
Study limitations
This review was based on trials of good quality. There is low-to-moderate risk of selection bias, as 40% of included studies did not report their concealment allocation. There is low risk of attrition or reporting bias. Published outcome data were generally complete. Performance bias is high in all included trials, as blinding of participants or therapist was impossible due to the complex nature of the intervention. We judged that there is low-to-moderate risk of detection bias, because 40% of studies did not clearly report using an independent assessor of outcomes. Another limitation is that some of the studies were not 100% home-based, and in making a decision of including those with at least 50% self-administered, task-oriented training may have affected the effect of home-based practice. Also, our meta-analyses may have been affected by small sample size bias. On average, there were 53 participants per study included in the meta-analyses. Some missing data were imputed by using statistical methods rather than raw study data, although this accounts for less than 10% of the total data. There could also be publication bias inherent to this systematic review by limiting our search to studies published in the English language. Furthermore, the high level of statistical heterogeneity in our analysis of home-based practice against no intervention could not be explained by our sensitivity analysis. Nor does it appear to be related to intervention dose.
Conclusion
Even though this review is based on trials of reasonably good quality, the existing evidence is insufficient to draw a robust conclusion on the effect of home-based practice for the upper limb. However, it does seem clear that in chronic, severely disabled stroke survivors, home-based practice does not improve upper limb activity. Furthermore, the use of technologies and assistive devices in providing motivation, feedback and instructions to the stroke survivors does not seem to yield the desired effect. Future study and design of home-based practice protocols could be guided by these findings.
The authors thank Malene Wøhlk Gundersen from OsloMet – Oslo Metropolitan University for her help in developing the search strategy for this review.
The authors have no conflicts of interest to declare.
Appendix 1. Search strategy.
Appendix 1. Search strategy. Cont.
Appendix 2: Excluded papers (n = 87).
Appendix 2: Excluded papers (n = 87). Cont.
Appendix 2: Excluded papers (n = 87). Cont.


 Click to show fullsize
Click to show fullsize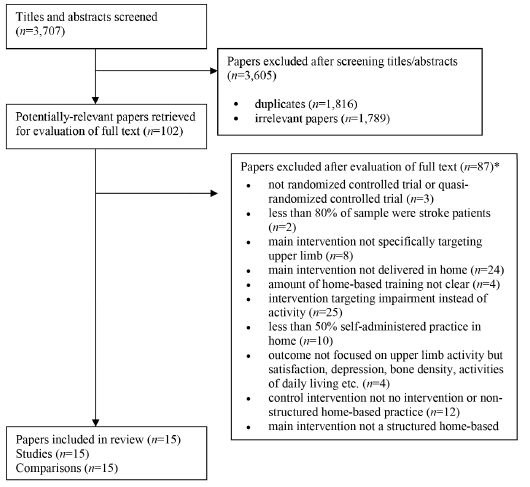 Click to show fullsize
Click to show fullsize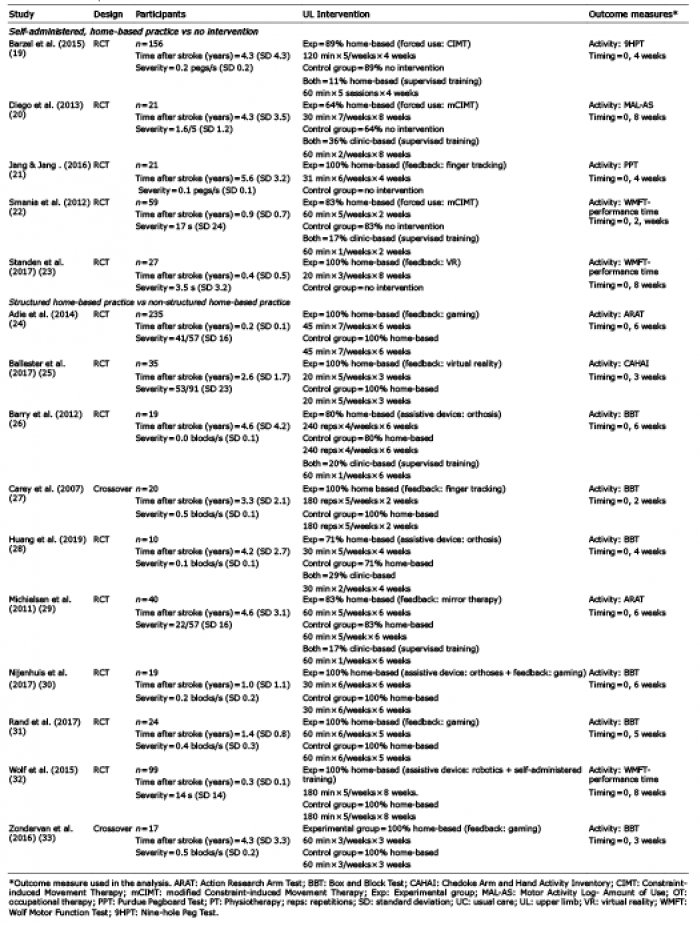 Click to show fullsize
Click to show fullsize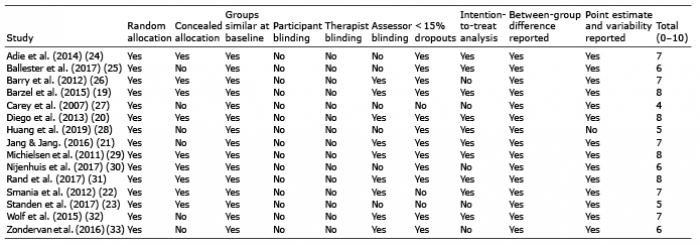 Click to show fullsize
Click to show fullsize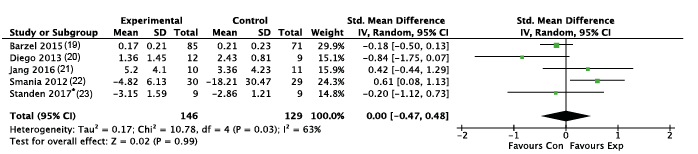 Click to show fullsize
Click to show fullsize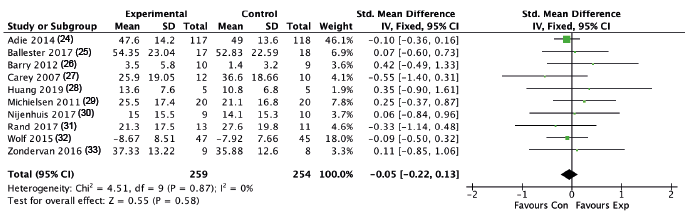 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize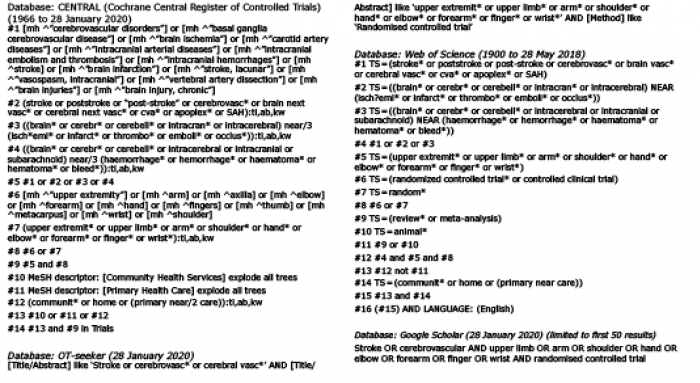 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize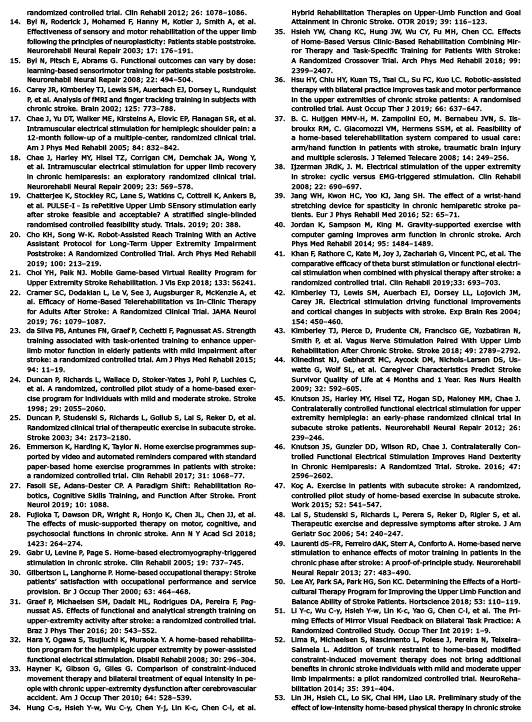 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize