
From the 1Faculty of Medicine and Dentistry and University Hospital, Palacký University Olomouc, Olomouc, Czech Republic, 2Moss Rehabilitation, Philadelphia, PA, USA, 3Department of Physical Medicine and Rehabilitation, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA, 4Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany and 5Department of Physical Medicine and Rehabilitation and the Department of Neurology, Northwestern University Feinberg School of Medicine and Shirley Ryan AbilityLab, Chicago, IL, USA
Objective: This post hoc analysis assessed the impact of repeated incobotulinumtoxinA injections on muscle tone, disability, and caregiver burden in adults with upper-limb post-stroke spasticity.
Design: Data from the double-blind, placebo- controlled main period and three open-label extension cycles of two Phase 3, randomized, multicentre trials were pooled.
Methods: Subjects received incobotulinumtoxinA 400 Units at 12-week intervals (±3 days) (study 3001, NCT01392300) or ≤ 400 Units at ≥12-week intervals based on clinical need (study 0410, NCT00432666). Ashworth Scale (AS) arm sumscore (sum of elbow, wrist, finger and thumb flexor, and forearm pronator AS scores), Disability Assessment Scale (DAS), and Carer Burden Scale (CBS) scores were assessed.
Results: Among 465 subjects, from study baseline to 4 weeks post-injection, mean (standard deviation) AS arm sumscore improved continuously: main period, –3.23 (2.55) (placebo, –1.49 (2.09)); extension cycles 1, 2, and 3, –4.38 (2.85), –4.87 (3.05), and –5.03 (3.02), respectively. DAS principal target domain responder rate increased from 47.4% in the main period (placebo 27.2%) to 66.6% in extension cycle 3. Significant improvements in CBS scores 4 weeks post-injection accompanied improved functional disability in all cycles.
Conclusion: IncobotulinumtoxinA conferred sustained improvements in muscle tone, disability, and caregiver burden in subjects with upper-limb post-stroke spasticity.
Key words: botulinum neurotoxin; duration of effect; incobotulinumtoxinA; upper limb; spasticity; caregiver burden; rehabilitation.
Accepted Oct 7, 2020; Epub ahead of print Oct 28, 2020
J Rehabil Med 2021; 53: jrm00138
Correspondence address: Petr Kaňovský, Faculty of Medicine and Dentistry and University Hospital, Palacký University Olomouc, Olomouc, Czech Republic. E-mail: petr.kanovsky@fnol.cz
Doi: 10.2340/16501977-2760
Spasticity (muscle overactivity) often occurs in patients after stroke and may lead to further disability. The results of 2 clinical trials were used to assess the effect of incobotulinumtoxinA injections (maximum dose used per injection session 400 Units) on arm and hand spasticity in patients after stroke. This study looked at the impact of treatment on disability and the burden on carers. The results from 4 treatment cycles were assessed. There was a continuous decrease in spasticity, together with improvements in disability in all treatment cycles. The burden on those who cared for patients also decreased. We showed that repeated incobotulinumtoxinA treatment across 4 cycles led to a decrease in spasticity, patient disability and burden on carers.
Stroke is an increasing cause of disability globally (1), and the development of spasticity in stroke survivors may contribute to further disability (2, 3). The prevalence of post-stroke spasticity ranges from 4.0% to 42.6% (2, 4, 5) and may be associated with reduced ability to perform the basic activities of daily living, and detrimental effects on quality of life (4, 6, 7). In addition to the loss of independence experienced by those affected, post-stroke spasticity can also result in a considerable burden on caregivers (6).
The safety and efficacy of botulinum neurotoxin type A (BoNT-A) injections have been well established for the treatment of upper-limb post-stroke spasticity (8–13). Notably, the 24-week BEST study evaluated the efficacy and safety of onabotulinumtoxinA in adults with upper-limb or lower-limb post-stroke spasticity (n = 273), and the addition of onabotulinumtoxinA to the existing standard of care demonstrated improvements in passive goal-oriented activities compared with placebo, as well as additional benefits in active functional goals with no new safety signals (14).
IncobotulinumtoxinA (Xeomin®, Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany) is a BoNT-A approved for the treatment of upper-limb spasticity at doses up to 400 Units (U) at intervals no sooner than every 12 weeks in the USA (15); while in Europe doses of up to 500 U at intervals of at least 12 weeks are approved, enabling treatment of a greater number of muscles (16). Two Phase 3 studies have confirmed the efficacy and safety of incobotulinumtoxinA in subjects with upper-limb post-stroke spasticity (17, 18); both studies included a placebo-controlled main period (MP) comprising a single injection cycle, followed by an open-label extension (OLEX) period with 3 fixed, 12-week incobotulinumtoxinA injection cycles (study 3001) (17), or a maximum of 5 flexible-duration injection cycles (study 0410) (19), respectively. Compared with placebo, incobotulinumtoxinA resulted in significant improvements in muscle tone (Ashworth Scale; AS) and functional disability (Disability Assessment Scale, DAS, for the principal target domain) 4 weeks post-treatment in the MP of both studies (17, 18). These improvements were sustained during the OLEX period of both studies (19–21) and associated with significant improvement in caregiver burden from the study baseline to the end of the OLEX period in study 3001 (21).
We report here the results of a post hoc analysis, using data pooled from the MP and the first 3 OLEX injection cycles of both studies, to assess the efficacy of incobotulinumtoxinA in a large subject population using the AS sumscore; a novel approach that allows for a holistic clinical assessment of arm spasticity. In addition, we assess the impact of repeated incobotulinumtoxinA injections on caregiver burden in this large population.
Study design and participants
This study was a post hoc analysis of 2 Phase 3, double-blind, randomized, placebo-controlled, multicentre trials, each with an OLEX period: studies 3001 and 0410. The study designs and full inclusion/exclusion criteria for both studies have been described previously (17–19). In brief, adult subjects with spasticity of the upper limb as a result of stroke were included if they had clinical patterns with a score of ≥ 2 on the AS (22) with respect to wrist and finger flexor spasticity (study 0410) (18) or in the muscle groups associated with the flexed elbow, flexed wrist, and clenched fist clinical patterns (study 3001) (17).
Exclusion criteria in both studies included spasticity of any aetiology other than stroke; bilateral upper-limb paresis; fixed contracture or severe atrophy in the target muscles; previous treatment with phenol; and previous treatment with BoNT within 4 (study 0410) or 12 months (study 3001) (17, 18).
Both studies were registered on clinicaltrials.gov (NCT00432666, study 0410 (MP, NCT00465738); and NCT01392300, study 3001) and conducted according to the principles of the Declaration of Helsinki. The study protocols and other appropriate study-related documents were reviewed and approved by the local independent ethics committees and institutional review boards at each participating site. All subjects provided written, informed consent (17, 18).
Treatments
Subjects were randomized to receive 1 injection of incobotulinumtoxinA or placebo in the MP, followed by 3 (study 3001) (17) or up to 5 (study 0410) (19) repeat injections of incobotulinumtoxinA in the OLEX period. IncobotulinumtoxinA injections were performed under the guidance of electromyography and/or electrical nerve stimulation, although ultrasound guidance was also permitted in study 3001 (17–19).
In study 3001, subjects received incobotulinumtoxinA at fixed 400 U total doses at fixed 12-week intervals (with an allowed deviation of ±3 days), with the option of a repeat visit for reinjection within 7 days of the end-of-cycle visit if there was no clinical need for repeat treatment at the time of the end-of-cycle visit. One primary target clinical pattern chosen by the physician at study baseline was treated with a predefined fixed dose of 200 U (flexed elbow), 150 U (flexed wrist), or 100 U (clenched fist). The physician determined the doses for treatment of other upper-limb muscle groups within predefined ranges based on clinical experience. All muscle groups with an AS score of ≥ 2 had to be treated (17).
In study 0410 subjects received incobotulinumtoxinA at total doses ≤ 400 U at flexible intervals of ≥ 12 weeks (median total doses received were 320 U in the MP, 385 U in OLEX cycle 1, and 400 U at all subsequent OLEX injection cycles). Subjects returned for scheduled study follow-up visits, and retreatment was provided if indicated in the study protocol with the agreement of the subject and the investigator, based on AS scores and clinical need (18, 19). Treatment of flexed wrist and clenched fist was mandatory in all subjects, and all muscles associated with these clinical patterns had to be treated (wrist and finger flexors). Elbow and thumb flexors and forearm pronators were treated if they had an AS score ≥ 2. Within elbow flexors, treatment of the biceps and at least one other muscle was mandatory. For the clinical patterns thumb-in-palm and pronated forearm, muscle groups were treated based on the clinical judgement of the treating physician. In cases where a clinical pattern was present in all muscle groups with an AS score ≥ 2, muscles for treatment were prioritized by the physician with a maximum dose of 400 U (18, 19).
Outcome measures
Ashworth Scale. The muscle tone of the treated arm was assessed using the 5-point AS (from 0 (no increase in muscle tone) to 4 (limb rigid in flexion or extension)) (22). In this post hoc analysis, the AS scores for all 5 clinical patterns (i.e. flexed wrist, clenched fist, flexed elbow, thumb-in-palm, and pronated forearm) that could be treated according to the clinical study protocols, were summed for each subject to generate the AS arm sumscore. Using a sumscore represents a novel, but not validated, approach similar to that of the Resistance to Passive Movement Scale (REPAS) for the whole body (23), which allows for a holistic assessment of arm spasticity. The AS arm sumscore included AS scores for all 5 clinical patterns, although not every subject required or received treatment for all 5 clinical patterns.
Disability Assessment Scale. The extent of functional disability in 4 domains: hygiene (defined as the extent of palm maceration, ulceration, or infection; cleanliness of the palm, ease of cleaning, and nail trimming; and the effect of hygiene-related disability on other areas of functioning), dressing (the ability to dress and the effect of dressing-related disability on other areas of functioning), limb position (psychological or social interference associated with spasticity), and pain (intensity and interference with activities of daily living), was assessed using the 4-point DAS (from 0 (no disability) to 3 (severe disability)) (24). A principal therapeutic target from 1 of the 4 domains was chosen by the subject, assisted by the investigator, before each treatment. Responders were defined as subjects with ≥1-point improvement in DAS scores 4 weeks post-injection compared with the score at study baseline.
Carer Burden Scale. The impact of treatment on the physical burden on the caregiver was assessed using a modified version of the Carer Burden Scale (CBS) (25) including an additional item, “applying a splint”, which is known to be troublesome for caregivers, and was added based on expert advice (18). The level of help required to perform 5 care activities (cleaning the palm of the hand, cutting the fingernails, cleaning the armpit, putting the affected arm through a coat or shirt sleeve, and applying a splint) was assessed by the same caregiver in relation to the affected limb at the study baseline and weeks 4, 8, and 12 post-injection. Each item for which the caregiver’s help was required was rated on a 5-point Likert scale ranging from 0 (no difficulty) to 4 (cannot complete the task). Data presented are based on the means of all applicable items per subject. The sum of item scores was divided by the total number of items answered to give a mean score (e.g. for those without splint the calculation is based on 4 items, and on 5 items for those with splint), summarizing caregiver burden for all tasks in one score for each subject (25).
Statistical analysis
The statistical software SAS version 9.4 was used for this post hoc analysis. Efficacy outcomes were evaluated using data pooled from the MP and first 3 OLEX injection cycles of both studies. All efficacy analyses were based on observed cases from the full analysis set (FAS), comprising all subjects randomized before and after protocol amendment in study 3001 (17) and all randomized subjects in study 0410 (18). Data from the placebo-controlled MP were analysed by treatment arm (incobotulinumtoxinA treatment vs placebo). Data from subsequent OLEX cycles, during which all subjects received incobotulinumtoxinA, were analysed for the total population, including those who received placebo in the MP, and who therefore received incobotulinumtoxinA treatment for the first time during the OLEX period.
The changes in AS arm sumscore from study baseline to weeks 4, 8, and 12 in the MP and from study baseline to weeks 4 and 12 of each OLEX injection cycle were assessed using summary statistics. The between-group difference for the changes in AS arm sumscore from study baseline to weeks 4, 8, and 12 in the MP was assessed using analysis of covariance (ANCOVA) with MP baseline score as covariate and containing sex as a factor.
The changes in CBS score (the mean score and the score for individual caregiving activities) from study baseline to weeks 4, 8, and 12 in the MP and from study baseline to the injection visit and weeks 4 and 12 of each OLEX injection cycle were assessed using Wilcoxon signed-rank test. The between-group differences from study baseline to weeks 4, 8, and 12 of the MP were evaluated using ANCOVA with MP score as covariate and containing sex as a factor. DAS data were assessed using descriptive statistics.
Subject characteristics and treatments
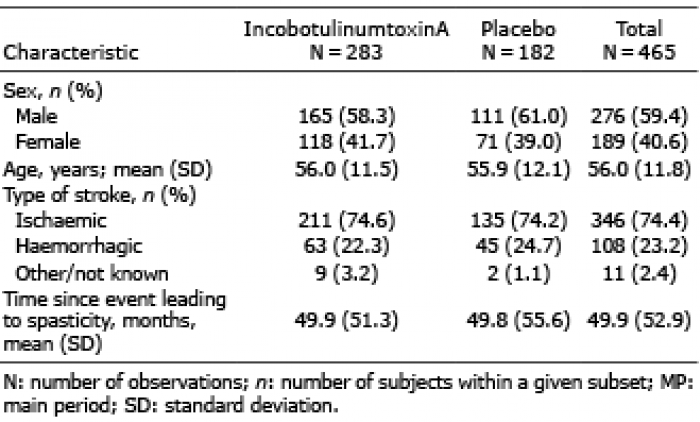
There were 465 subjects included in the FAS for this post hoc analysis, including 283 and 182 subjects who were randomized and received incobotulinumtoxinA and placebo, respectively, in the MP. The mean (standard deviation; SD) age of the pooled population was 56.0 (11.8) years, and the majority of subjects were male (276/465, 59.4%). Most subjects had spasticity because of either ischaemic stroke (346/465, 74.4%) or haemorrhagic stroke (108/465, 23.2%), and the mean (SD) time since the spasticity-causing event was 49.9 (52.9) months (Table I).
Table I. Subject demographics and characteristics at study baseline
IncobotulinumtoxinA doses administered for each clinical pattern are summarized in Table II. Consistent with the study protocols, most subjects received treatment of wrist and finger flexors during the MP.
Table II. IncobotulinumtoxinA doses administered in the main period (N = 283)
Efficacy outcomes
Muscle tone. IncobotulinumtoxinA treatment resulted in a significantly greater improvement (reduction) in AS arm sumscore vs placebo from study baseline to 4, 8, and 12 weeks post-injection in the MP (p < 0.0001, p < 0.0001, and p = 0.001, respectively; ANCOVA) (Fig. 1). AS arm sumscore improved with incobotulinumtoxinA treatment from study baseline to 4 weeks post-injection in all injection cycles. Mean (SD) improvements in incobotulinumtoxinA-treated subjects increased continuously from –3.23 (2.55) at week 4 of the MP (placebo, –1.49 (2.09)) to –4.38 (2.85), –4.87 (3.05), and –5.03 (3.02) in OLEX cycles 1, 2, and 3, respectively (Fig. 1). The improvement associated with incobotulinumtoxinA was sustained to the end of OLEX cycle 3, with a mean (SD) improvement of –3.01 (2.96) vs the study baseline (Fig. 1), and –2.13 (2.99) vs the end of the MP.
Fig. 1. Change in Ashworth Scale (AS) arm sumscore from study baseline at all visits. Subject numbers at each time-point are noted in the table beneath the figure. *p = 0.001, **p = 0.0001, analysis of covariance (ANCOVA) for the difference between incobotulinumtoxinA and placebo treatment groups. AS arm sumscore was calculated for each subject by adding AS scores for the clinical patterns flexed wrist, clenched fist, flexed elbow, thumb-in-palm, and pronated forearm; data based on observed cases from the full analysis set: a pooled analysis of studies 3001 and 0410. BL: baseline; MP: main period; OLEX: open-label extension; SD: standard deviation.
Disability. The DAS domains most frequently chosen as the principal target for treatment at the study baseline were “limb position” and “dressing” (incobotulinumtoxinA: 113/280 (40.4%) and 92/280 (32.9%), respectively; and placebo: 68/182 (37.4%) and 64/182 (35.2%), respectively). For the principal target domains chosen at study baseline, there was further improvement with repeated incobotulinumtoxinA injections, compared with a single injection in the MP. The DAS responder rate was 47.4% for incobotulinumtoxinA-treated subjects 4 weeks post-injection during the MP (placebo, 27.2%) and increased to 66.6% during OLEX cycle 3. The DAS responder rate remained high at 12 weeks post-injection (59.7% in OLEX cycle 3, Fig. 2).
Fig. 2. Disability Assessment Scale (DAS) responder rate for the principal target domain for treatment in main period (MP) and open-label extension (OLEX) injection cycles. Responder rates were calculated from the study baseline for the principal target domain. Responders were defined as subjects with ≥1-point improvement in DAS scores 4 weeks post-injection vs the study baseline. Data based on observed cases from the full analysis set: a pooled analysis of studies 3001 and 0410. Data labels within each bar represent the number of DAS responders/number of observations. Data labels above each bar represent the DAS response rate.
Carer Burden Scale. Compared with placebo, incobotulinumtoxinA resulted in a significantly greater reduction (improvement) in mean CBS score from study baseline to 4, 8, and 12 weeks post-injection in the MP (p = 0.0137, p = 0.0025, and p = 0.0290, respectively; ANCOVA; Table III). A significant and sustained improvement from the study baseline to 4 and 12 weeks post-injection was also shown in subsequent injection cycles in the OLEX period, as well as from the end of the MP to the end of OLEX cycle 3 (p < 0.0001 for all; Wilcoxon signed-rank test) (Table III).
Table III. Carer Burden Scale score
There was an improvement in all caregiving activities from study baseline to 4 weeks post-injection in all treatment cycles (Fig. 3). During the MP, there was a significant improvement in all caregiving activities from study baseline to 4 weeks post-injection (p < 0.001; Wilcoxon signed-rank test), except “applying a splint”, which applied to only 25 and 13 subjects receiving incobotulinumtoxinA or placebo, respectively. There was a similar improvement from study baseline to 8 and 12 weeks post-injection (p < 0.05 and p ≤ 0.001, respectively, for all caregiving activities except “applying a splint”; Wilcoxon signed-rank test).
Fig. 3. Improvement in Carer Burden Scale (CBS) from study baseline to 4 weeks post-injection. Improvement was defined as a ≥1-point reduction on CBS score. Data based on observed cases from the full analysis set: a pooled analysis of studies 3001 and 0410. Data labels within each bar represent the number of subjects with improvement/number of observations. Data labels above each bar represent the percentage of subjects with improvement. Inco/A: incobotulinumtoxinA; MP: main period; OLEX: open-label extension.
During the OLEX period, further significant improvement from study baseline to 4 weeks post-injection was shown for all caregiving activities, including “applying a splint” (p < 0.05; Wilcoxon signed-rank test). This improvement was sustained at 12 weeks post-injection in all OLEX cycles (p < 0.001 for all caregiving activities except “applying a splint”, p < 0.05 for “applying a splint” in OLEX cycle 3 only; Wilcoxon signed-rank test).
Furthermore, the percentage of subjects with an observed improvement in individual caregiving activities ranged from 31% to 43% at week 12 of the MP, and increased to 47% to 59% of subjects at the end of OLEX cycle 3, indicating sustainable improvements for all 5 items of the CBS.
This post hoc analysis assessed the effects of incobotulinumtoxinA treatment on muscle tone and functional disability over 4 injection cycles and up to 48 weeks’ duration, and its impact on caregiver burden, using data pooled from 2 Phase 3 studies in subjects with post-stroke spasticity of the upper limb (17–19).
The pooled analysis assessed the effects of incobotulinumtoxinA treatment on muscle tone using the AS arm sumscore; this allowed for a more integrated clinical assessment of arm spasticity, especially when doses per muscle and the number of muscles treated are variable in line with each subject’s specific impairment and treatment goals, as is the case in the present study population and clinical practice (26). Although the minimal clinically important difference on this novel scale is not defined, the approach follows the principles of the REPAS scale for assessment of the whole body (23). As the reliability of the AS may be affected by the lack of standard guidelines for positioning and performance, it is important to perform the AS as per the principles of the REPAS scale, i.e. with instructions for individual joint motions (23), as also done in comparator studies (14). Passive range of motion in the REPAS arm subscore is well associated with manual dexterity, suggesting that paresis, resistance to passive movement, and arm function are closely related (23). Here, incobotulinumtoxinA resulted in significant improvement in muscle tone of the whole arm vs placebo at 4, 8 and 12 weeks post-treatment, which was consistent with previous reports for individual clinical patterns (8, 10, 12, 27, 28) and was associated with a reduction in disability. At 4 weeks post-injection in the MP, there were almost twice as many DAS responders for the principal target domain with incobotulinumtoxinA compared with placebo. Importantly, muscle tone continued to improve with repeated incobotulinumtoxinA treatment during the OLEX period, and the DAS responder rate remained high 12 weeks post-injection in OLEX cycle 3. Furthermore, repeated incobotulinumtoxinA treatment was associated with a significant and sustained reduction in caregiver burden. Improvements after a single injection cycle were enhanced by repeated treatment during the OLEX period, consistent with previous studies (29, 30).
In the present analysis, rather than the usual 4 items, the CBS was based on 5 items with the inclusion of “applying a splint”, which is known to be troublesome for caregivers (18). This additional item was added based on expert advice and, although no formal validation of this modified scale has been performed against the original scale, the overall reductions in CBS score presented here were consistent with those of a previously published study that assessed only 4 items (29). Improvements from study baseline to 4 weeks post-injection in all caregiving activities were shown in the MP, reaching significance for all items except “applying a splint”, which applied to a low number of subjects. For all items, compared with a single injection in the MP, carer burden was further improved with multiple incobotulinumtoxinA injections during the OLEX period, suggesting a cumulative effect of treatment.
Study limitations previously discussed for the individual studies also apply to this post hoc analysis (17–20). The main limitation of this analysis is that the data are pooled from 2 Phase 3 studies. However, the design of these studies is generally comparable, and the statistical power to study treatment effects is increased with the larger sample size in the pooled population.
In summary, this post hoc analysis supports the findings of the original studies across a larger pooled subject population. The results presented here add to the body of evidence showing that incobotulinumtoxinA confers sustainable improvements in muscle tone in such chronic populations, with cumulative improvement in DAS responder rate, and show the continuous improvement in caregiver burden with repeated incobotulinumtoxinA treatment.
The authors wish to thank the subjects and study investigators. Medical writing support, under the direction of the authors, was provided by Claire Cairney, PhD, CMC Connect, McCann Health Medical Communications, and was funded by Merz Pharmaceuticals GmbH, Frankfurt am Main, Germany, in accordance with Good Publication Practice (GPP3) guidelines (31).
Conflicts of interest. PK: Has received honoraria and speaker’s fee from Desitin/Merz Pharmaceuticals, Medtronic, EverPharma, AbbVie, and fees for participation in the Gedeon Richter Spasticity Advisory Board. EPE: Participated in a Speakers’ Bureau for Ipsen Biopharmaceuticals Inc., and received funding from Merz Pharmaceuticals to participate as coordinating investigator for study 3001. His spouse is an employee of Allergan plc. MCM: Was an advisory board participant for Merz Pharmaceuticals in November 2017. AH: Employee of Merz Pharmaceuticals GmbH. IP: Employee of Merz Pharmaceuticals GmbH. MA: Employee of Merz Pharmaceuticals GmbH. RH: Employee of Merz Pharmaceuticals GmbH. CM: Employed by Shirley Ryan AbilityLab, formerly known as the Rehabilitation Institute of Chicago. This institution received funding from Merz Pharmaceuticals for work performed for study 3001. The Shirley Ryan AbilityLab also receives funding from Ipsen Biopharmaceuticals Inc., and Revance Therapeutics Inc. for Dr Marciniak’s research-related activities.


 Click to show fullsize
Click to show fullsize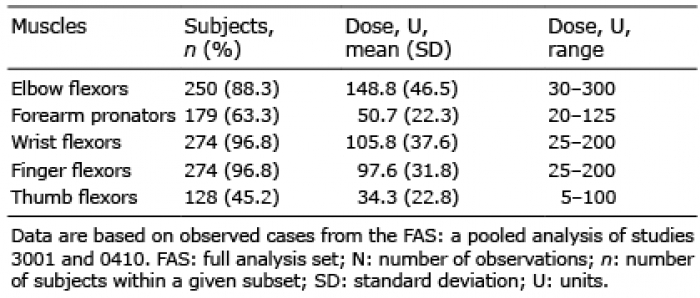 Click to show fullsize
Click to show fullsize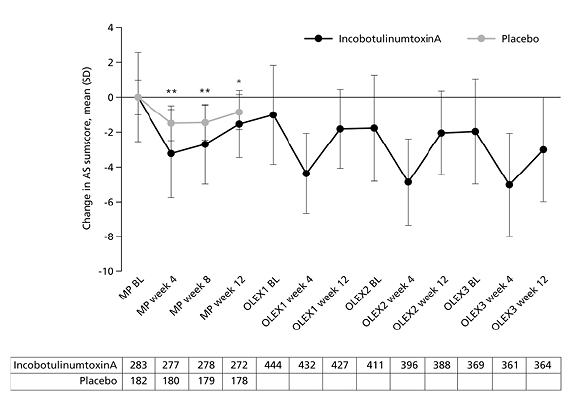 Click to show fullsize
Click to show fullsize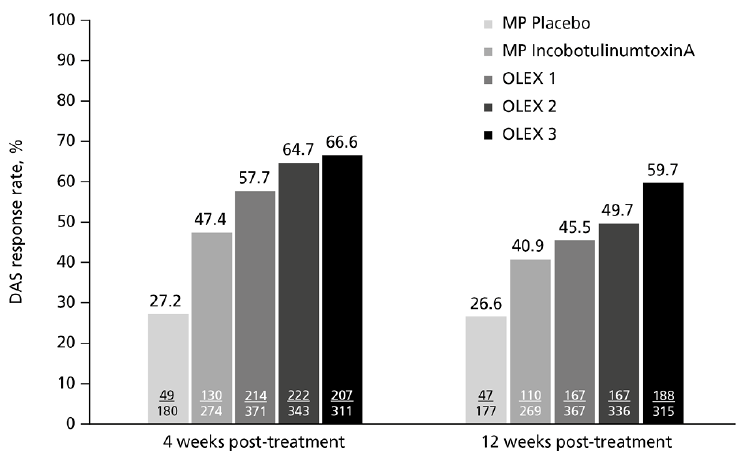 Click to show fullsize
Click to show fullsize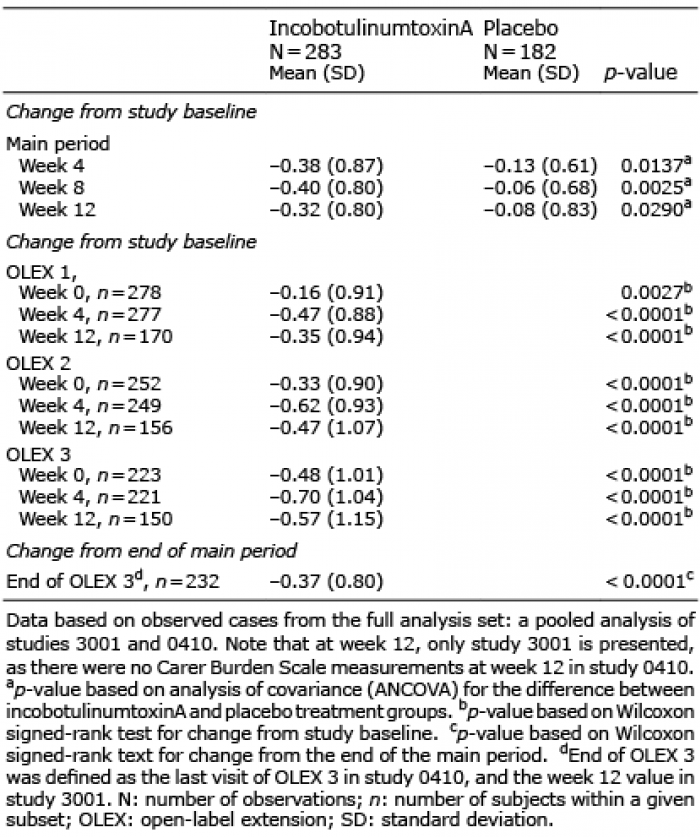 Click to show fullsize
Click to show fullsize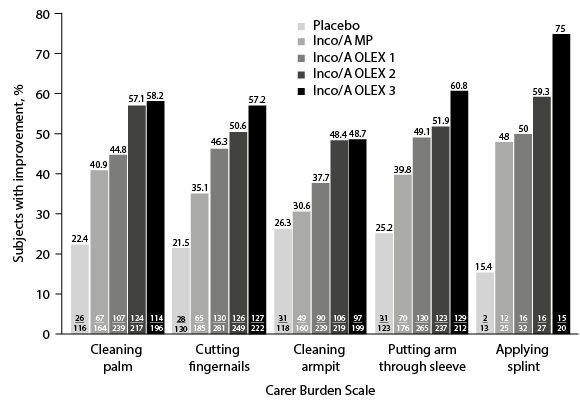 Click to show fullsize
Click to show fullsize