
From the 1Department of Neuropsychology and Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht University, Maastricht, 2Limburg Brain Injury Centre, 3Department of Medical Psychology, Zuyderland Medical Centre, Sittard-Geleen, and 4School for Mental Health and Neuroscience, Department of Psychiatry and Neuropsychology, Faculty of Health, Medicine and Life Sciences, Maastricht University Medical Center, Maastricht, The Netherlands
Objective: To evaluate the construct validity of Psychomotor Vigilance Test performance for measuring fatigue in people with acquired brain injury.
Design: Observational cross-sectional study.
Participants: Fifty-four people with acquired brain injury and 61 healthy controls.
Methods: Participants performed the Psychomotor Vigilance Test and reported momentary fatigue before and after this test and general fatigue. Associations between performance and fatigue in patients were tested by correlational and hierarchical multiple linear regression analyses, controlling for sleep quality, daytime sleepiness, and mood.
Results: Patients performed worse on the test compared with controls. Within the patient group, worse test performance was associated with increases in momentary post-test fatigue and general fatigue, indicating convergent validity, but also with daytime sleepiness, and mood complaints, indicating a lack of divergent validity. When controlling for sleepiness and mood, the association between performance and general fatigue was no longer significant, whereas the association between performance and post-test fatigue remained.
Conclusion: Performance on the Psychomotor Vigilance Test cannot be used as a specific measure for fatigue, but it appears to be a more general measure of severity of symptoms including fatigue, mood, and sleepiness. Therefore, the Psychomotor Vigilance Test may be a useful measure to examine the effects of interventions aimed at reducing these symptoms.
Key words: Psychomotor Vigilance Test; fatigue; brain injury; sleepiness; mood; construct validity.
Accepted Oct 23, 2020; Epub ahead of print Nov 12, 2020
J Rehabil Med 2020; 52: jrm000129
Correspondence address: Jessica Bruijel, Department of Neuropsychology and Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht University, 6200 MD Maastricht, The Netherlands. E-mail: jessica.bruijel@maastrichtuniversity.nl
Doi: 10.2340/16501977-2766
Fatigue is a frequent symptom following acquired brain injury. Assessment is usually based on self-report, but additional objective measures are advised. The Psychomotor Vigilance Test has previously been found to be sensitive to the effects of acquired brain injury and performance on this test may relate to fatigue and sleepiness. This study examined whether Psychomotor Vigilance Test performance in people with acquired brain injury is associated with fatigue, after controlling for daytime sleepiness, sleep quality, and mood. The study found that performance on this test is related to fatigue, but also to sleepiness and mood. The Psychomotor Vigilance Test therefore cannot be used as a specific measure for fatigue, but could be used to measure changes or improvement of symptoms including fatigue, mood and sleepiness. The Psychomotor Vigilance Test thus has the potential to be implemented as an objective measure to evaluate these symptoms following acquired brain injury in both research and clinical practice.
Fatigue is a prevalent and disabling symptom following acquired brain injury (ABI) (1, 2). Fatigue may be a direct consequence of the brain injury (primary fatigue), but it can also be provoked by other symptoms related to the injury, such as mood or sleep disturbances (secondary fatigue) (3). Furthermore, fatigue following ABI is often associated with depressive mood and daytime sleepiness (3), and may negatively impact recovery and quality of life (1).
Assessment of fatigue is commonly based on self-report; however, accurate self-report may be complicated in people with ABI due to language and cognitive problems (4). Moreover, fatigue itself is multidimensional, and different factors, such as mood, medication and pain, may influence fatigue (1), making it difficult to measure subjective fatigue in a quantitative way. Therefore, additional objective measures are needed to evaluate fatigue in the ABI population (4). The few objective methods available, such as electroencephalography, are often impractical and too time-consuming for clinicians to use. Measuring fatigue using a simple and fast-to-administer cognitive task, such as the Psychomotor Vigilance Test (PVT), may therefore be more suitable in clinical settings (5).
The PVT is a simple reaction time (RT) task that measures sustained attention to visual or auditory stimuli (6, 7). It is one of the best-validated and most widely used measures of sleepiness-related sustained attention deficit (7–9). Two studies found that PVT performance was impaired in participants with ABI, compared with healthy controls (HC) (8, 9). Interestingly, these differences were no longer significant when controlling for feelings of fatigue, while some of the differences remained when controlling for feelings of sleepiness or sleep quality (8, 9). This indicates that performance differences between these groups were more associated with fatigue than with sleepiness. Therefore, PVT performance may be a useful objective measure for fatigue after ABI.
Even though fatigue often occurs in conjunction with sleepiness, these are distinct concepts with different treatment options (10). Therefore, to evaluate fatigue using the PVT, it is important to differentiate the unique contributions of fatigue and sleepiness on PVT performance. This differentiation is lacking in most studies. Furthermore, it is known that these symptoms are associated with depression and anxiety, frequently experienced following ABI (3, 11). Therefore, to examine whether PVT performance can be used as an objective measure of fatigue in people with ABI, the current study aimed to determine whether general and momentary fatigue contribute to PVT performance, after controlling for mood, daytime sleepiness, and sleep quality.
In line with previous research (8, 9), it was expected that participants with ABI would show performance deficits in the PVT compared with HC. To evaluate the construct validity of the PVT for measuring fatigue in people with ABI, it was hypothesized that PVT performance within the ABI group would correlate significantly with general and momentary fatigue scores (convergent validity), and that associations with daytime sleepiness, mood and sleep quality would be weak (divergent validity). Finally, it was hypothesized that associations between PVT performance and fatigue in participants with ABI would remain significant after controlling for these other constructs.
Participants
Participants were individuals with a history of ABI recruited from an outpatient rehabilitation unit at Zuyderland Medical Centre, the Netherlands, or as part of their involvement in a larger follow-up study examining sleep and fatigue following traumatic brain injury (TBI) in the period from November 2017 until September 2019 (12). ABI was confirmed by a neurologist using imaging data and/or injury characteristics, including loss of consciousness, post-traumatic amnesia and behavioural symptoms. This information was used to classify TBI as mild or moderate-severe using the Mayo classification system (13). Participants were referred to the study by a neurologist, rehabilitation doctor or neuropsychologist. Inclusion criteria were: history of ABI and age between 21 and 70 years. Exclusion criteria were: a neurological condition other than ABI, and a current diagnosed mental disorder based on clinical judgement.
The PVT data of HC (n = 61) from 3 previous studies conducted at Maastricht University under similar circumstances (14–16) were used for comparison with participants with ABI. HC were selected to match age, since age is known to affect PVT performance (17). Exclusion criteria were history of a neurological disorder or psychiatric illness, history or current drug or alcohol abuse, and current use of psychoactive medication, based on self-report and medical examination.
Procedure for participants with acquired brain injury
The study protocol was approved by the Ethics Review Committee Psychology and Neuroscience of Maastricht University (ERCPN-177_15_03_2017). All participants provided written informed consent before study enrollment. Participation consisted of one visit at the hospital, university, or participant’s home. During this visit, participants first completed questionnaires measuring their general feelings of fatigue, sleepiness, sleep quality, and mood. Next, the PVT was administered. Immediately before and after the PVT, participants completed a visual analogue scale for fatigue (VAS-f) to measure momentary fatigue. The duration of the visit was approximately 30 min. Visits were scheduled at participant’s convenience between 09.00 h and 17.00 h on a weekday.
Assessments
Psychomotor Vigilance Test. A computer-based version of the 10-min visual PVT was used for both groups (6). Participants were instructed to monitor a screen and respond by pressing a button with their dominant hand as soon as a number counting up from 0 was seen. This stopped the counter and displayed the RT in milliseconds (ms). The inter-stimulus interval varied randomly from 1,400 to 9,400 ms. The PVT has good psychometric properties (18, 19).
Mean inverse RT (1/RT) was used as primary outcome parameter, since it decreases the contribution of long lapses. To calculate 1/RT, each RT (ms) was divided by 1,000 and then reciprocally transformed (7). Number of lapses (RT ≥ 500 ms) were used as secondary outcome parameter. To normalize data, number of lapses were transformed using the square root formula (√x+√(x+1)) (8). Other outcome measures, used only for comparisons with HC, were mean RT, median RT, 10% slowest 1/RT and time on task RT decrements (7).
RTs ≤ 100 and ≥ 10,000 ms were considered invalid and not included in calculations, since these probably include premature responses and misses (7). Since no practice trial was included in the study, RTs of the first 5 stimuli were excluded from the analysis to minimize habituation effects. To examine time on task decrements, 1/RT was averaged per minute (i.e. blocks of 9–10 stimuli).
Validating instruments. A Dutch version of all questionnaires was available and all questionnaires have been used previously in the Dutch ABI population.
General fatigue. General feelings of fatigue were assessed with the Fatigue Severity Scale (FSS) (20). The FSS measures the impact of fatigue on activities of daily living and distress caused by fatigue. It includes 9 items related to fatigue, which are rated on a 7-point Likert scale. Scores range from 1 to 7 and a mean score of ≥ 4 indicate severe fatigue (20). The FSS has good psychometric properties (20). In people with ABI a high internal consistency was found (Cronbach’s α: 0.90) (21) and test-retest reliability of the FSS is satisfactory (Intraclass correlation coefficient: 0.82) (22). The FSS can distinguish levels of fatigue in brain-injured participants from that of controls (23).
Momentary fatigue. Momentary fatigue was measured with a 100-mm horizontal VAS-f before (VASpre) and after (VASpost) the PVT (23). The left-hand end of the line represented “absolutely no fatigue” and the right-hand end “most severe fatigue imaginable” with no intermediate divisions or descriptive terms. Scores range from 0 to 100, with higher scores indicating more fatigue. Participants are instructed to rate their fatigue intensity over the previous 5 min. The VAS-f has been used in previous studies with participants with ABI (11, 23, 24) and was found to be valid and reliable (25).
Sleep quality. Subjective sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI) (26). The PSQI contains 19 items, providing a global score ranging from 0 to 21. Higher scores indicate poorer sleep quality, with a global score > 5 indicating poor sleep quality (26). The PSQI has reliable psychometric properties (26) and has been used in participants with ABI (8, 9, 27).
Daytime sleepiness. Daytime sleepiness and sleep propensity were assessed with the Epworth Sleepiness Scale (ESS) (28). The ESS consists of 8 items, with scores range from 0 to 24, and a score of ≥ 10 indicates clinically significant sleepiness (28). The ESS is widely used in ABI research (9, 24, 27) and has good reliability (29).
Mood. Mood was assessed with the Hospital Anxiety and Depression Scale (HADS) (30). The HADS consists of 14 items, and includes 2 subscales for anxiety and depression. Total scores range from 0 to 42 with higher scores indicating a higher intensity of symptoms. Scores on the subscales range from 0 to 21 and a score ≥ 8 is an indicator of depression or anxiety (31). The HADS is a reliable measure and has been validated in the ABI population (31).
Statistical analysis
To achieve a power of 0.8, with α set to 0.05 and a medium-to-large effect size (f2 = 0.25) for a multiple regression analysis with 4 predictors the required sample size was 53 participants (32).
Differences between participants with ABI and HC were analysed using independent-sample t-tests (or Welsh t-tests in case of unequal variance) for age and PVT parameters, and a χ2 test for sex distribution. To compare the slope of the time-on-task effect between groups, RTs per minute were analysed using multilevel linear models. Construct (convergent/divergent) validity was evaluated by examining the association between PVT performance (1/RT, transformed lapses) and subjective measures of fatigue (FSS, VAS-f), and with measures of daytime sleepiness (ESS), mood (HADS) and sleep quality (PSQI), using Pearson’s correlation coefficients (r, 2-tailed). The same analysis was used to examine associations between general fatigue (FSS) and daytime sleepiness, mood and sleep quality. Correlations were considered high when r> 0.5 and moderate when r> 0.3 (33). In addition, multilevel linear models were used to examine the effect of fatigue on the slope of the time-on-task effect.
To examine whether fatigue was associated with PVT performance (1/RT) after controlling for mood and sleepiness, hierarchical multiple linear regression analyses were used. General fatigue (FSS) and momentary fatigue following the PVT (VASpost) were examined separately. A stepwise forced entry regression was used, in which fatigue was entered first (model 1), followed by mood (HADS, model 2), daytime sleepiness (ESS, model 3) and sleep quality (PSQI, model 4) to examine whether fatigue still contributes to the PVT outcome when controlling for sleep.
Statistical significance was set at 0.05. Statistical analyses were performed with IBM SPSS version 25.
Group characteristics
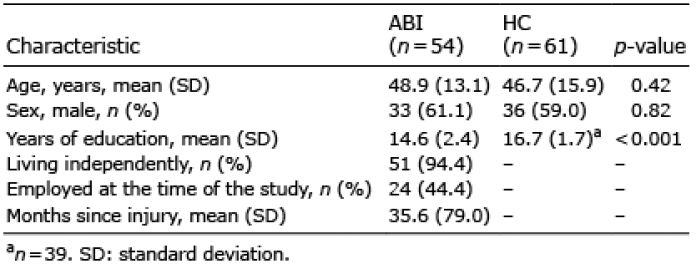
Demographic characteristics of the ABI and control groups are shown in Table I. A total of 54 participants with ABI (33 males, 21 females), age range 21–70 years participated, and 61 HC (36 males, 25 females) aged between 24 and 74 years old were included from historical datasets. HC did not differ in age or sex from the participants with ABI. The control group was more highly educated compared with the ABI group. Data about living situation and employment of the control group was missing. In the ABI group, time since injury ranged from 60 days to 35 years. Forty participants reported a TBI, 12 experienced a stroke and 2 had another type of ABI. Of the stroke participants 10 (83%) experienced an ischaemic stroke and 2 (17%) a haemorrhagic stroke. The main causes of injury in the TBI group were traffic accidents (n = 25) and falls (n = 15). The severity of TBI was moderate-severe in 35 (87.5%) participants and mild in 5 (12.5%) participants (13). Scores on the questionnaires of the ABI group are shown in Table II.
Table I. Demographics of participants with acquired brain injury (ABI) and healthy controls (HC)
Table II. Self-reported fatigue, sleep and mood variables of the participants with acquired brain injury (ABI) (n = 54)
Psychomotor Vigilance Test
Comparison between participants with ABI and HC. Participants with ABI had significantly longer mean RTs, more lapses, and longer 10% slowest 1/RT compared with HC (Table III). Analysis of time-on-task effects on 1/RT showed significant decrement in performance as the task progressed (F(1, 145.2) = 14.2, p < 0.01), but no significant interaction with group was found (F(1, 256.7) = 0.01, p = 0.9). Thus, there was no difference in vigilance decrement between participants with ABI and controls.
Table III. Psychomotor Vigilance Test (PVT) outcome parameters for participants with acquired brain injury (ABI) (n = 54) and healthy controls (HC) (n = 61)
Construct (convergent/divergent) validity. Moderate to high correlations were found between performance on the PVT, as measured by 1/RT and lapses, and levels of fatigue, as measured by the FSS, VASpre and VASpost, indicating convergent validity (Fig. 1; Table IV). PVT performance also showed moderate to high correlations with daytime sleepiness and mood, as measured by the ESS and HADS, respectively (Table IV), indicating a lack of divergent validity. There was no correlation between PVT performance and sleep quality, measured by the PSQI (Table IV). The time-on-task decrement in 1/RT in participants with ABI did not increase with higher levels of fatigue, as measured with the FSS (F(1, 127.1) = 0.01, p = 0.9) and VASpost (F(1, 126.8) = 1.68, p = 0.2). Fatigue as measures with the FSS showed moderate to high correlations with daytime sleepiness (ESS, r: 0.61, p < 0.001), mood (HADS, r: 0.57, p < 0.001) and sleep quality (PSQI, r: 0.46, p < 0.001).
Fig. 1. Relationship (a) between general fatigue and inverse reaction time (1/RT) on the Psychomotor Vigilance Test (PVT) with 95% confidence intervals (95% CI) and (b) between momentary fatigue and 1/RT, with 95% confidence intervals (95% CI). Note: Due to transformation, higher transformed reaction time (RT) values represent faster reaction times.
Table IV. Correlations (r) between Psychomotor Vigilance Test (PVT) outcome parameters and fatigue, sleep and mood questionnaires for participants with acquired brain injury (ABI) (n = 54)
Hierarchical multiple linear regression. Table V shows results of the hierarchical multiple linear regression analyses using 1/RT as dependent variable, with the focus on general fatigue measured with the FSS and the focus on momentary fatigue post-PVT measured with VAS-f. In the model focusing on general fatigue, when including the HADS, significant associations between FSS and 1/RT remained (model 2). After adding the ESS (model 3), the association between FSS and 1/RT no longer remained. The final model (model 4) including FSS, HADS, ESS and PSQI showed that ESS and HADS were the only significant individual predictors of 1/RT. The full adjusted model (model 4) explained 40% of the variance in 1/RT (F4, 50 = 9.98, p < 0.01). In the model focusing on momentary fatigue, when including the HADS, significant associations between VASpost and 1/RT remained (model 2). The final model including VASpost, HADS, ESS and PSQI showed VASpost, HADS and ESS were all significant predictors of 1/RT. The full adjusted model explained 48% of the variance in 1/RT (F4, 50 = 13.41, p < 0.001).
Table V. Results of hierarchical multiple linear regression analysis of the relation between mean inverse reaction time (1/RT) and general fatigue or momentary fatigue in participants with acquired brain injury (ABI) (n = 54)
The main objective of the present study was to examine the contribution of fatigue to PVT performance of people with ABI, in order to examine whether the PVT can be used as an objective measure of fatigue in these individuals. Results showed that PVT performance was worse in participants with ABI compared with HC. In line with the study hypothesis, performance deficits in participants with ABI were associated with increased levels of fatigue indicating convergent validity. However, divergent validity was poor, since PVT performance in people with ABI was also associated with mood and daytime sleepiness, and when controlling for these factors, the association between general fatigue and PVT performance was no longer significant. Nevertheless, the association between momentary fatigue following the PVT and PVT performance remained when controlling for daytime sleepiness and mood.
Contrary to our expectations, general fatigue no longer predicted PVT performance after controlling for mood, daytime sleepiness and sleep quality. In this model, daytime sleepiness and mood were the only independent predictors of PVT performance. It was expected that general fatigue would partly explain the performance deficits found in participants with ABI, because previous research suggested that PVT performance seemed mostly affected by fatigue when comparing participants with ABI with controls (8, 9). In the current study within a group of people with ABI, a strong association with sleepiness was found, similar to studies in healthy volunteers (7). Therefore, fatigue may adequately differentiate PVT performance between patients and controls, but might not be the best variable to differentiate performance within individuals with ABI.
Although momentary fatigue was still associated with PVT performance when controlling for mood, sleepiness and sleep quality, it was not unique. Sleepiness and mood were also independent predictors of PVT performance. Fatigue can be either a primary brain-injury induced symptom, but it can also occur in reaction to the injury (3). The same is true for sleep problems and depressive symptoms. It is very difficult to disentangle these primary and secondary symptoms, especially in a cross-sectional study, such as this. Taken together, we conclude that the PVT cannot be used to specifically measure only fatigue in people with ABI. Performance on the PVT seems to be a more general measure of fatigue, and symptoms often concurring with fatigue, such as depression and daytime sleepiness in people with ABI. Therefore, the PVT might be used to assess changes or improvement in these symptoms following ABI. However, more research is necessary to evaluate the validity of PVT performance as a measure of fatigue and fatigue-related symptoms.
Decrements in performance with time-on-task can be due to fatigue (34). In the current study, there was a decrement in performance with time-on-task in both the ABI and control groups. However, this decrement did not differ between groups, and was not associated with level of fatigue in participants with ABI. In contrast, overall response speed, as measured by 1/RT, did differ between groups, and was associated with levels of fatigue in participants with ABI. These results are in line with previous findings (35) and support the idea that people with ABI might be slower in general, but not necessarily show progressive slowing during task performance (8, 36).
To examine whether the results were driven by participants who reported the most symptoms, the data was reanalysed, excluding the 20% highest scores on the HADS and again excluding the 20% highest score on the FSS. This did not change the results, suggesting that the results are not driven by poor performance or over-reporting of symptoms.
For future research, it would be of interest to examine PVT performance in people with ABI over time after injury, and determine how mood, fatigue and sleepiness are related to PVT performance at different time-points. Since mood complaints have been shown to develop later in the disease process following ABI and have shown to be associated with reports of fatigue earlier in the disease process, there may be an indication that fatigue contributes to secondary mood complaints following ABI (3). Therefore, PVT performance may be more strongly related to fatigue early in the disease process compared with later in the disease process when secondary mood complaints might develop. Furthermore, future research could examine how a fatigue-inducing experience, such as a lengthy test battery, affects PVT performance, to evaluate the validity of the PVT as a measure of momentary or task-related fatigue. It might be interesting to explore this with the brief 3- or 5-min version of the PVT. A quick and easy-to-administrate test, such as the PVT, which could measure momentary/task-related fatigue, would allow for a broader understanding how fatigue might influence cognitive functioning and daily activities.
According to the COnsensus-based Standards for the selection of health Measurement INstruments Risk of Bias (COSMIN-RoB) checklist (37), the methodological quality of this study to test the construct validity of the PVT for measuring fatigue in people with ABI, can be considered as very good. PVT outcomes were compared with the FSS and VAS-f, which are well-validated measures of fatigue, and have been used previously in a Dutch-speaking population of people with ABI (38, 39). To test the hypothesis that PVT outcomes correlate more highly with the FSS and VAS-f (convergent validity) than with measures of other frequently co-occurring complaints (divergent validity), specifically sleep quality (PSQI) daytime sleepiness (ESS) and anxiety and depression (HADS), Pearson’s correlations were conducted.
Study limitations
This study has some limitations. First, the study did not differentiate between physical and mental fatigue, although this is recommended by previous studies examining fatigue in people with ABI (2). Research in patients with obstructive sleep apnoea and HC showed a relationship between physical fatigue and PVT lapses, but found no relationship between mental fatigue and PVT outcome measures (40). Future research should, therefore, examine whether certain aspects of fatigue may relate better to specific outcome measures of the PVT and whether the PVT could be utilized to quantify different aspects of fatigue in individuals with ABI.
Secondly, data about living situation and employment was missing from the control group, therefore groups could not be compared on these variables. However, previous research shows that PVT performance is affected mostly by age and sex, which were comparable between the groups (17). Furthermore, there was heterogeneity in the ABI sample with different causes of brain injury, diverse time since injury, variability in injury severity and a broad age range. However, we consider that this reflects everyday clinical practice. Injury severity may contribute to PVT performance, given its association with processing speed and attention (41). Moreover, multiple studies have indicated a relationship between age and PVT performance, with elderly subjects showing longer RTs than younger subjects (17). However, none of these variables were related to PVT outcome measures in this study (not reported). In addition, multiple studies did not find a relationship between injury characteristics, such as injury severity and time since injury, and PVT performance in participants with ABI (8, 9). Furthermore, this heterogeneity in this studies ABI sample indicates that the PVT could be used as a measure of fatigue and other symptoms, such as mood and sleepiness, in a wide variety of people with ABI and may, therefore, be useful in the clinic.
Finally, even though fatigue and sleepiness are distinct concepts, they often occur together and are frequently seen as the same concept by the general public (24). It is possible that much of the variance in PVT performance is shared by fatigue and sleepiness and that, therefore, general fatigue no longer predicts PVT performance when controlling for daytime sleepiness. The results indicate a strong association between the sleepiness and general fatigue questionnaires. Future studies including objective measures of daytime sleepiness could explore this relationship and differentiate fatigue from daytime sleepiness.
Conclusion
In conclusion, PVT performance is not exclusively associated with fatigue, but also shows strong associations with mood and daytime sleepiness. The PVT may therefore be a useful measure to examine the effects of interventions aimed at reducing fatigue or other symptoms.
The authors would like to thank J. Heijmink, S. Koch, I. Bras, M. Smeets, L. Tummers, and C. Voorter for data collection. This study is funded by Maastricht University.
The authors have no conflicts of interest do declare.


 Click to show fullsize
Click to show fullsize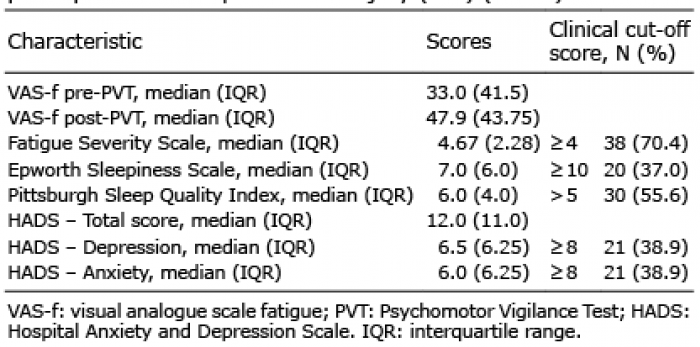 Click to show fullsize
Click to show fullsize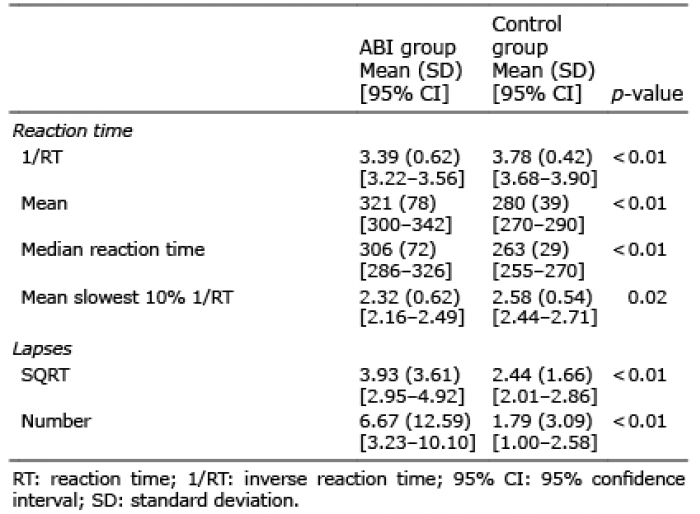 Click to show fullsize
Click to show fullsize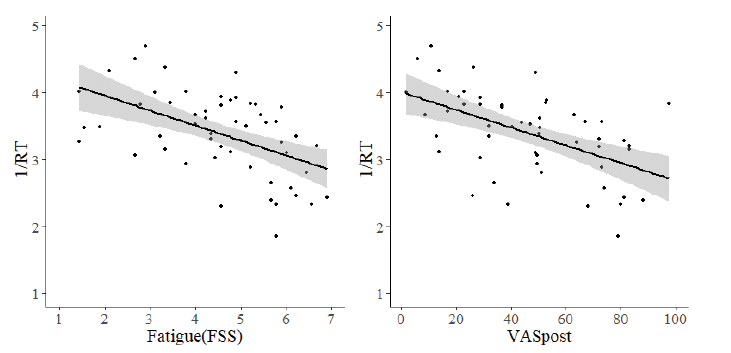 Click to show fullsize
Click to show fullsize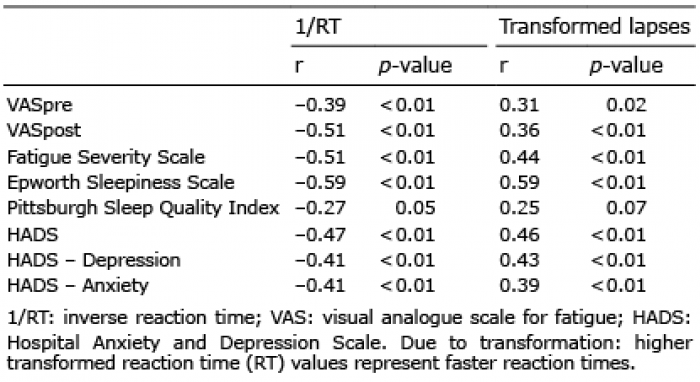 Click to show fullsize
Click to show fullsize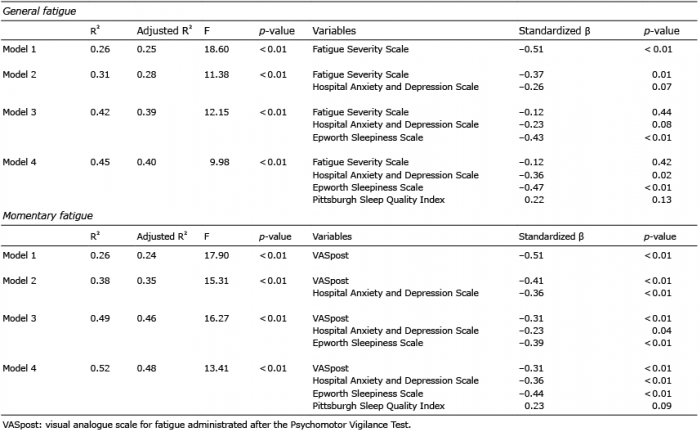 Click to show fullsize
Click to show fullsize