
From the 1Department of Medicine and Surgery, University of Parma, Parma and 2Department of Surgical and Medical Sciences, University of Catanzaro “Magna Grecia”, Catanzaro, Italy
Objectives: To conduct a systematic review of randomized controlled trials about the safety (number and severity of adverse events) and efficacy (pain reduction and functional improvement) of mesotherapy in musculoskeletal disorders, and to compare them with other therapeutic options, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.
Methods: A search of PubMed, Cochrane Library and Scopus database resulted in an initial total of 16,253 records. A total of 931 articles were included in the study. A final total of 7 articles, published from 1 Jan 1999 until 30 Apr 2020 were selected. Two independent reviewers selected potentially relevant studies based on the inclusion criteria for full-text reading. They evaluated the methodological quality of each study and included only studies of high methodological quality, according to the Physiotherapy Evidence Database scale.
Results: Seven studies were included in the meta-analysis, and visual analogue scale scores before and after mesotherapy were considered. A statistically significant reduction in visual analogue scale score in the mesotherapy group was reported in comparison with the control group in all except one of the trials. Mesotherapy was found to be a safe procedure with mild and temporary side-effects, such as nausea, fatigue, numbness, sweating, headache, ecchymosis, bleeding, pain and local reaction at the injection site.
Conclusion: Mesotherapy proved to be more effective than systemic therapy in the treatment of local pain and functional limitations caused by a variety of musculoskeletal conditions. However, because of the heterogeneity of the analysed studies in terms of injected drugs, administration technique, associated treatments, frequency and total number of sessions, more randomized controlled trials are needed, comparing a standardized mesotherapy protocol with a systemic treatments.
Key words: mesotherapy; intradermal injection; subcutaneous injection; soft-tissue injection; musculoskeletal disorder.
Accepted Feb 26, 2021; Epub ahead of print Mar 25, 2021
J Rehabil Med 2021; 53: jrm00182
Correspondence address: Cosimo Costantino, Department of Medicine and Surgery University of Parma, Via Gramsci 14, 43126 Parma, Italy. E-mail: cosimo.costantino@unipr.it
Doi: 10.2340/16501977-2817
Mesotherapy is a minimally invasive technique, based on microinjections of active drugs into the surface layer of the skin in the area to be treated. The treatment implies 2 advantages: a lower dose of drug and a rapid onset with a prolonged duration of action. The aim of this review was to analyse the safety and efficacy of mesotherapy in musculoskeletal disorders comparing it with other therapeutic options. An initial search of the literature retrieved 16,253 records. Two independent reviewers selected relevant studies based on the inclusion criteria. Furthermore, 7 studies were included for meta-analysis. The injected drugs were non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, local analgesics and muscle relaxants, of different types and concentrations, alone or variously combined. Mesotherapy was performed in the painful area, via an intradermal or subcutaneous route. It resulted in a statistically significant reduction in visual analogue scale (VAS) score in comparison with the control group in all except one of the trials. Adverse events reported for mesotherapy were generally few and mild. In conclusion, mesotherapy may be effective in enabling pain relief and functional improvement in musculoskeletal disorders, allowing patients early access to rehabilitation services, such as physiotherapy and occupational therapy, in order to achieve better outcomes in terms of independence in activities of daily living.
Musculoskeletal conditions are extremely common and include more than 100 different syndromes and diseases, which are usually associated with pain and loss of function and are a major cause of disability (1).
According to the Fit for Work Europe study, 100 million European citizens have chronic musculoskeletal pain, with high prevalence in the working population (2). Data from the 2016 United States Bone and Joint Initiative suggest that 50% of American people live with a musculoskeletal condition, a prevalence comparable to that of cardiovascular and chronic respiratory diseases combined (3).
Musculoskeletal conditions cause more functional limitations in the adult population than any other disorder and are a major cause of years lived with disability worldwide. The prevalence of physical disabilities caused by a musculoskeletal condition has been estimated as to be high as 4–5% of the adult population living in Canada, the USA, and Western Europe (3).
The 2016 Global Burden of Disease (GBD) data for non-communicable diseases stated that disability-adjusted life years (DALYs) for musculoskeletal conditions increased by 61.6% between 1990 and 2016, with an increase of 19.6% between 2006 and 2016 (3). In the 2017 GBD study, musculoskeletal conditions were the second highest contributor to global disability, accounting for 16% of all years lived with disability, and lower back pain remained the single leading cause of disability (4).
Musculoskeletal pain and physical disability reduce social functioning and mental health, further diminishing the patient’s quality of life, but they also consume a large amount of health and social care resources. Their economic impact is well known, since they are associated with direct and indirect costs, with the latter being predominant (5).
It has been estimated that musculoskeletal diseases account for 50% of absence from work and 60% of permanent work incapacity (5). Elderly patients with a musculoskeletal disease have lower level of physical activity, poorer mobility, frailty, depression, cognitive impairment, higher risk of falls, and poorer sleep quality (6, 7).
Apart from non-pharmacological approaches, musculoskeletal pain disorders are traditionally managed with drugs to reduce pain, inflammation, and functional disability (8). However, the major drawback of systemic pharmacological therapy with analgesics and anti-inflammatory drugs is the frequent association with adverse effects, some of which can be life-threatening. Side-effects and drug–drug interactions can be detrimental, especially among older patients and those with concomitant disorders needing polytherapy (9, 10).
Paracetamol use is associated with gastrointestinal, cardiovascular, hepatic and renal adverse events. Moreover, paracetamol hypersensitivity is not uncommon (11–13). Non-steroidal anti-inflammatory drugs (NSAIDs) have been associated with a wide range of adverse events affecting the gastrointestinal, cardiovascular, and renal systems (14). NSAIDs are recognized to be the most common drugs involved in hypersensitivity drug reactions, in particular in the case of systemic administration (15). Systemic administration of corticosteroids is associated with adverse events, such as hypertension, hyperglycaemia, hyperlipidaemia, weight gain, glaucoma, cataract, gastrointestinal toxicity, osteoporosis, myopathy, avascular necrosis, immunosuppression, impaired wound healing, mood disorders, memory deficit, and even psychosis (16). Opioids, used either alone or in combination with paracetamol and/or NSAIDs, may cause a variety of side-effects, which are dose-limiting and reduce quality of life (17).
Among the various attempts to reduce systemic drug toxicity, the use of local therapy (e.g. interventional spine procedures, intra-articular or periarticular injections, topical administration of pharmacological agents) has gained popularity among physicians (18, 19). However, they require appropriately trained staff and equipment, and their therapeutic efficacy is controversial in many musculoskeletal disorders (20, 21). Intra-articular and periarticular injections are a viable option, but side-effects are still possible, such as infections and haematomas (22, 23).
Mesotherapy is an alternative therapeutic treatment that can be effective and reliable to treat a variety of painful musculoskeletal syndromes. The term mesotherapy comes from the word “mésothérapie”, introduced by the French physician Michel Pistor (24). It has been defined as a minimally invasive technique, based on microinjections of active ingredients into the surface layer of the skin corresponding to the area to be treated (25). This “micro deposit” gives rise to a slower release of the drug into the surrounding tissues compared with parenteral administration, with the possibility of 2 advantages: a lower dose of active compound can be used; and a rapid onset and prolonged action duration can be achieved (25). The goal of the treatment is to modulate the pharmacokinetics of the injected substance and to prolong the pharmacological effects in the affected area; the local pharmacological effect can be obtained with a lower dosage (26).
Concerning safety, some adverse events have been reported, many of which are caused by incorrect procedure, application by non-qualified personnel, or lack of asepsis technique (27).
Despite the growing interest in mesotherapy, scientific evidence regarding this technique is weak and there is a paucity of randomized controlled trials (RCTs) on this subject (25–28). In 2011 and 2014 Mammucari et al. conducted a review of the literature concerning mesotherapy and drew up a series of recommendations in the form of consensus report: nevertheless, non-randomized controlled trials were included in the analysis, and the authors confirmed the need for further studies (29, 30). Paolucci et al. performed a systematic review to examine the efficacy and safety of mesotherapy. They found that mesotherapy was effective and well tolerated, but non-randomized controlled trials were also included, and hence a comparison between different interventions was missing. Moreover, only the intradermal route of administration was considered (31). Recently Plachouri et al. have examined the efficacy of mesotherapy in the medical and cosmetic field, and have confirmed the need for larger systematic studies (27).
Objectives
The aims of the current study were to conduct a systematic review and meta-analysis of the literature, including only high-quality RCTs, about the safety (number and severity of adverse events) and efficacy (pain reduction and function improvement) of mesotherapy in musculoskeletal disorders; and to compare them with other therapeutic options. Safety was considered the primary outcome and efficacy the secondary outcome. Both the intradermal and subcutaneous routes of administration of mesotherapy were included, despite different pharmacokinetics (28–32).
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement.
Data sources
The goal of the current study was to determine the safety and efficacy of mesotherapy in patients with musculoskeletal conditions within the Population, Intervention, Comparison, and Outcome (PICO) framework. The population (P) was defined as individuals of both sexes and all ages with musculoskeletal conditions. The intervention (I) was mesotherapy. The comparison (C) was placebo or other therapeutic options. The outcomes (O) were safety (number and severity of adverse events) and efficacy (pain reduction and function improvement).
The following electronic databases were searched: PubMed, Cochrane Library and Scopus, for all papers published from 1 January 1999 until 30 April 2020, using the following keywords: ‘’mesotherapy’’; ‘’intracutaneous injection’’; ‘’intradermal injection”; ‘’subcutaneous injection’’; ‘’soft tissue injection’’; ‘’musculoskeletal’’. These keywords were used in several combinations with Boolean operators (AND/OR) and modified for databases. A manual search of reference lists of selected papers and reviews on the topic was performed to identify additional relevant studies.
Inclusion and exclusion criteria
Exclusion criteria were:
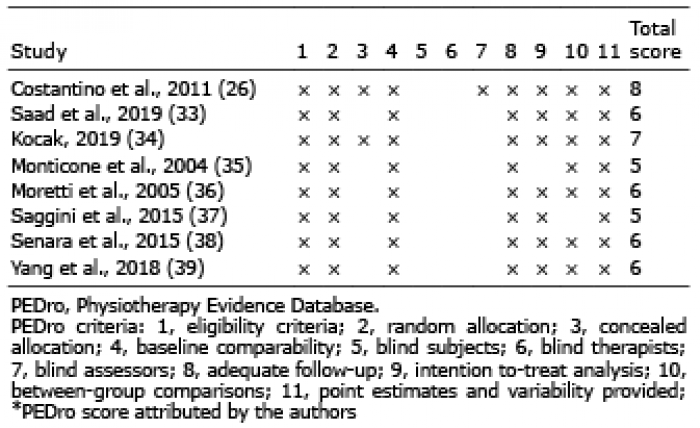
The methodological quality of selected studies was assessed using the Physiotherapy Evidence Database (PEDro) scale independently by 2 authors. Any discrepancies between reviewers were resolved through discussion with the third and fourth authors. For the purposes of this review, studies were included if they achieved a score of 5 or more. If the studies’ score was not reported in the PEDro database, 2 researchers assessed the score independently. The researchers were blinded to each other’s quality assessment, and in the event of disagreement, third and fourth opinions were sought.
This study also considered the presence/absence of eligibility criteria of included subjects, which correlates with the external validity of the study, in order to comprehend all the items in the Delphi list; however, such criteria were not used to calculate the final PEDro score, since they do not influence the internal or statistical validity of the trial (Table I).
Table I. Quality assessment of selected studies
Study selection
From a total of 16,253 studies retrieved from different databases, 15,322 were excluded since they were duplicate studies, non-RCT studies, studies written in languages other than in English, and without full text available. Of the remaining 931 studies, 919 studies did not meet the inclusion criteria listed above. From the 12 studies selected, 4 were excluded after quality assessment according to the PEDro score checklist. A total of 8 studies were considered for systematic review. Of these, 7 studies were considered for meta-analysis because of missing data in the study by Kocak (34).
The level of evidence of the included studies, according to the Oxford Center for Evidence-Based Medicine (OCEBM) Level of Evidence is II (https://www.cebm.net/2016/05/ocebm-levels-of-evidence/). The review process is shown in Fig. 1.
Fig. 1. Study flow diagram.
Data extraction
Two reviewers independently extracted the data from selected studies using a standard form. The following information was extracted for each article: author and year of publication; characteristics of the participants (age, sample size, treatment indication with symptoms length if available); description of the intervention in the experimental group (mesotherapy); description of the intervention in the control group; outcome measures; follow-up.
Assessment of risk of bias
The level of evidence of included studies was stratified according to the OCEBM. Two authors independently assessed methodological quality of data acquisition using the Critical Appraisal Skills Programme for Diagnostic Test Studies (CASP; http://www.casp-uk.net/checklists). In the case of 3 possible responses (“yes”, “no” or “can’t tell”), where one author entered “no”, often the other entered “can’t tell”, although both responses scored 0. In case of disagreement, a third and fourth opinion was sought.
Statistical analysis
Seven studies were included in the meta-analysis and visual analogue scale (VAS) values were considered before and after mesotherapy (Table II).
The mean difference as an effect size measure and a fixed effects model was used to calculate the pooled estimates with 95% confidence intervals (95% Cis). Heterogeneity was assessed by Q statistic and I2: I2<25% was low in heterogeneity and I2 >75% as high in heterogeneity.
Table II. Visual analogue scale (VAS) score before and after treatment
Possible publication bias was assessed using a contour-enhanced funnel plot of effect size against its standard error. All statistical analyses and forest plots were produced using Stata 12.0 (StataCorp, College Station, TX, USA) and RevMan 5.3. Statistical significance was established for p-values <0.05. The results of the meta-analysis are shown as a forest plot in Fig. 2. Possible publication bias was assessed using a funnel plot of the effect size against its standard error. The result of the funnel plot is shown in Fig. 3.
Fig. 2. Mesotherapy treatment compared with control group. 95% CI: 95% confidence interval. Kocak (2019) (34) was excluded due to missing data.
Fig. 3. Funnel plot with mean difference (MD) and size effect (SE) of the VAS: most studies, except for 1 (Moretti et al., 2005 (36)) report homogeneous results in favour of mesotherapy.
Details of selected studies are reported in Table III and Table IV. Four trials used mesotherapy to treat low back pain with (33) or without (26, 34, 38) radicular pain.
Table III. Summary of included studies
Table IV. Safety and efficacy of selected studies
The remaining 4 studies included patients with non-specific neck pain (39), pes anserine tendinopathy in knee osteoarthritis (37), tendinopathies and entrapment syndromes of the limbs (36), and acute pain in musculoskeletal disorders (34).
Exclusion criteria for most selected studies were pathologies of severe gravity and different origin from the musculoskeletal system, such as diabetes, anticoagulation therapy, cardiovascular, renal, hepatic, gastrointestinal, or psychiatric disease (26, 38); having injury at multiple sites, traumatic fractures, serious or life-threatening conditions (33); pregnancy, known hypersensitivity to injected products, infiltrative therapy with hyaluronic acid, polynucleotides or corticosteroids in progress, drug abuse or alcohol abuse, significant co-morbidities (such as neurological abnormalities, concomitant severe rheumatic disease, and systemic abnormalities, such as diabetes), a surgical intervention within 3 months before the study, psychiatric conditions, or psycho-therapy or physical therapy within 5 weeks before the study (37); having fracture, carcinoma, infection, neuropathy, spinal cord diseases or previous spinal cord surgery, infection at the injection sites, coagulopathy, opioid addiction, obesity with body mass index (body weight/height2) > 30 kg/m2, neuropsychiatric diseases or a related treatment history, pregnancy (39); cardiovascular, renal, hepatic, gastrointestinal (peptic ulcer), psychiatric disease, pregnancy, known hypersensitivity to administered substances, coagulation disorders (33). Monticone et al. (35) and Moretti et al. (36) did not clearly report the exclusion criteria for the mesotherapy group.
The mean age of study populations ranged from 31.0 years (34) to 53.5 years (standard deviation (SD) 2.64) (26).
The mesotherapy treatment protocol was heterogeneous in terms of injected drugs, administration technique, associated treatments, frequency and total number of sessions. In all studies the injected drugs were NSAIDs, corticosteroids, local analgesics and muscle relaxants, of different types and concentrations, alone or variously combined; mesotherapy was performed in the painful area, via an intradermal or subcutaneous route (26, 33–39). Point by point injection was the most frequently used technique; 3 studies did not report the adopted technique clearly (35–37). The needles used for mesotherapy had 27 G (33, 35) or 30 G (26, 34, 36, 38) diameter, with 4-mm (26, 33, 35, 38) or 6-mm 68 length; 2 studies did not report the needles characteristics clearly (37, 39). Mesotherapy was performed alone in all studies (26, 33, 34, 36–39) except for one (35), where it was combined with stabilization exercise, re-education, and a specific pelvic girdle. The therapeutic protocols were different in terms of number and frequency of sessions: Kocak (34) and Yang et al. (39) performed a single administration; Fathy et al. (33) performed 4 weekly administrations; Costantino et al. (26) and Senara et al. (38) performed 5 administrations in 2 weeks; Monticone et al. (35) performed 2 administrations a week for 4 weeks; Moretti et al. (36) performed 2 administrations a week for 5 weeks; Saggini et al. (37) performed 3 administrations a week for 3 weeks; the protocol by Moretti et al. (36) had the longest duration (5 weeks) and the most frequent sessions (2 sessions for 1 week).
Treatments adopted in the control groups were different: most trials compared mesotherapy with systemic therapy (26, 33, 34, 37–39), while Monticone et al. (35 compared mesotherapy with He-Ne laser therapy, and Moretti et al. (36) compared mesotherapy with oxygen-ozone therapy. Follow-up evaluations were different in number and time from the first mesotherapy session. The earliest follow-up was just after treatment (35), while the latest was after 12 months from the first session (34).
Primary outcome: safety
The safety of included studies is shown in Table III. Adverse events reported for mesotherapy were generally few and mild. When statistical comparison was reported, no difference was found between mesotherapy and control groups. In 2 studies (33, 34) no adverse events were noted, either in the mesotherapy group or in control groups.
Yang et al. (39) indicated a list of non-serious adverse events, such as nausea, fatigue, numbness, sweating, headache, ecchymosis, but the difference from the control group was not statistically significant.
Costantino et al. (26) reported cases of local and temporary bleeding and inflammation signs in the injection site, which resolved in a few days in all patients, both in the case group and in the control group, immediately after the injection; mesotherapy was well-tolerated overall and no local or allergic reactions were seen.
Moretti et al. (36) reported that 7 patients in 40 treated with mesotherapy reported pain in the injection site, allergic reaction or return of the pain some hours after mesotherapy treatment; no collateral effect was seen in the control group.
Saggini et al. (37), Senara et al. (38) and Monticone et al. (35) did not clearly report any adverse events.
Secondary outcome: efficacy
All the studies evaluated reported a reduction in pain, as measured by VAS (26, 33–39) with a statistically significant difference after treatment in 6 studies (26, 33–35, 38, 39).
The Forest plot (Fig. 2) reports a synthesis of the standardized mean difference (effect size) of the VAS obtained from mesotherapy and control groups. Possible publication bias was assessed using a Funnel plot of the effect size against its standard error. The result of the Funnel plot is represented in Fig. 3.
The meta-analysis indicates that patients treated with mesotherapy had a lower VAS score of pain after treatment, or, in other words, a greater reduction in pain, with an effect size of –0.868 (95% CI –1.509; –0.227).
The difference between experimental and control groups was statistically significant in 5 studies (33–35, 37, 39); in contrast, oxygen-ozone therapy was found to be more effective than mesotherapy in the reduction of pain (35); in one study (36) no statistical intergroup comparison was found.
Four studies evaluated and documented an improvement in function, as measured by different validated functional scales: the Roland Morris Disability Questionnaire (RMDQ) and/or Oswestry Low Back Pain Disability Questionnaire (ODQ) and/or range of motion (ROM) for the low back (26, 38), the Neck Disability Index (NDI) for the neck (39), the Knee Injury and Osteoarthritis Outcome Score (KOOS) for the knee (37). Statistically significant improvement was found after treatment in all studies (26, 37–39) and between mesotherapy and control group in 2 of those 3 studies (38–39). In one study (36) no statistical intergroup analysis was found.
Moreover, Yang et al. (39) evaluated and documented an improvement in self-reported evaluation scales, measured using questionnaires, regarding patients’ opinions about the effectiveness of the proposed mesotherapy and satisfaction. The same author (39) also found that patients treated with mesotherapy had a lower score in the Patient Global Impression of Change (PGIC) on day 3.
Furthermore, Monticone et al. (35) evaluated and documented improvement in Laslett’s test and Men test for sacroiliac dysfunction: both test were negative at the end of mesotherapy treatment.
This review found that mesotherapy seems to be a safe procedure, with mild and temporary adverse events. A statistically significant reduction in visual analogue scale (VAS) score in comparison with the control group in all trials except one, was recognised. Reported side-effects were: nausea, fatigue, numbness, sweating, headache, ecchymosis, temporary bleeding and signs of inflammation, pain at the injection site, allergic reaction, and pain relapse. Conversely, Moretti et al. (36) reported side-effects only in the mesotherapy group (7 in 40 patients: 14% of the whole population, having experienced pain in the injected sites, pain relapse and allergic reaction) and not in the control group treated with oxygen-ozone therapy. Since the author did not clearly report the exclusion criteria for the study or the specific musculoskeletal diseases of the patients reporting these side-effects, no specific conclusion can be drawn about these data.
Mesotherapy proved efficient in treatment of local pain and functional limitations caused by a variety of musculoskeletal conditions, and a statistically significant improvement was measured in outcome evaluation scales. With one exception, (35) the evaluated studies reported a reduction in pain according to the VAS.
It is important to note that mesotherapy was used alone in 6 of these 7 trials: Monticone et al. (35) associated mesotherapy with specific exercise for the pelvic girdle to treat sacroiliac dysfunction, and therefore it is difficult in this case to determine if the reported positive outcomes can be attributed to mesotherapy solely.
Five studies (26, 33, 37–39) evaluated and documented a significant improvement in patients’ function, as measured with the appropriate evaluation scales (RMDQ, ODQ, ROM, NDI, KOOS). In all of these studies, mesotherapy was the sole intervention.
Mesotherapy characteristics, such as number of sessions, frequency of application, drugs injected, were heterogeneous between studies. Mesotherapy technique, as well as needle sizes and diameters, were not always reported, hence no conclusions can be drawn about a possible specific correlation with outcomes.
Senara et al. (38) compared conventional mesotherapy, bee venom mesotherapy, and systemic therapy. Because of its large availability and utilization, the current study considered only conventional mesotherapy (using NSAIDs, local anaesthetic and glucocorticoid). Notably, bee venom mesotherapy was equally effective and well tolerated as conventional mesotherapy and pain reduction and functional improvement were reported to be statistically greater in patients treated with mesotherapy in comparison with different types of interventions in the control groups in at least one follow-up.
The most frequent indication for treatment was low back pain with (33) or without (26, 35, 38) radiculopathy. Monticone et al. (35) treated patients with low back pain and sacroiliac dysfunction. Different musculoskeletal conditions were examined in the remaining studies (non-specific neck pain, pes anserine bursitis in knee osteoarthritis, acute musculoskeletal injuries, tendinopathies and entrapment syndromes of the limbs) (34, 36, 37, 39).
The treatments used in the control groups were also heterogeneous: while 6 of the included studies compared mesotherapy with systemic therapy with various anti-inflammatory drugs (NSAIDs and/or glucocorticoids), Monticone et al. (35) used physical therapy with He-Ne laser, and Moretti et al. (36) used oxygen-ozone therapy.
All the studies reported a significant reduction in pain, and the difference was statistically greater in the mesotherapy group in comparison with control groups in 5 studies (33–35, 38, 39). Four of these 5 studies used mesotherapy alone, while Monticone et al. (35) added physiotherapy and a pelvic girdle too, hence it is difficult to state whether these better results can be attributed to mesotherapy alone. The diseases in which mesotherapy achieved better pain reduction were low back pain (33–35, 38) and non-specific neck pain (39). Costantino et al. (26) showed that mesotherapy was equally effective as systemic therapy, but using half of the total pharmacological dosage.
One could conclude that mesotherapy is at least as effective as systemic therapy in the treatment of low back pain and more effective in the treatment of specific neck pain. However, some studies did not clearly report pain duration, so we cannot draw further conclusions.
Among the 5 studies evaluating patients’ function, Senara et al. (38) and Yang et al. (39) reported that functional improvement was significantly better in the mesotherapy group than in the control groups. Both of these studies used mesotherapy alone and compared it with systemic therapy. Patients included were affected by low back pain and non-specific neck pain. Fathy et al. (33) and Saggini et al. (37) used mesotherapy alone, and documented a functional improvement, although without statistical difference, from control groups. Costantino et al. (26) also showed similar improvement in functional disability in the daily life activity, with a 50% reduction in dosage of drugs (NSAIDs (ketoprofen) and corticosteroid (methylprednisolone).
Study limitations
The analysed studies showed different algorithms and test procedures. In some cases test procedures were not clearly reported. Different diseases were treated and different therapies were used in control groups. When interpreting the results of the current study, the substantial heterogeneity of the included studies must be taken into account.
More research is needed in this field, especially methodologically robust RCTs with adequate samples to enable statistical analysis. Further studies should use a standardized mesotherapy protocol, with a specific set of injected active agents, administration route, needle characteristics, number and frequency of administration sessions, comparing outcomes with control groups with the optimum available disease-specific treatment option, or at least with an adequate pharmacological systemic therapy, in order to draw more precise conclusions about the safety and efficacy of mesotherapy in the musculoskeletal field.
Conclusion
Mesotherapy was found to be a safe procedure with mild and temporary side-effects, such as nausea, fatigue, numbness, sweating, headache, ecchymosis, bleeding, pain and local reaction at the injection site. Use of mesotherapy proved to be more effective than systemic therapy for statistically significant pain reduction and functional improvement in the treatment of non-specific neck pain and low back pain, and had no more side-effects than systemic therapy.
Since musculoskeletal disorders are best managed with multidisciplinary care, and mesotherapy may be effective in pain relief and functional improvement, it could allow patients early access to rehabilitation services, such as physiotherapy and occupational therapy, leading to better outcomes in terms of independence in the activities of daily life. Hence, mesotherapy may be a viable option for use in the management of painful and disabling musculoskeletal conditions in clinical practice.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize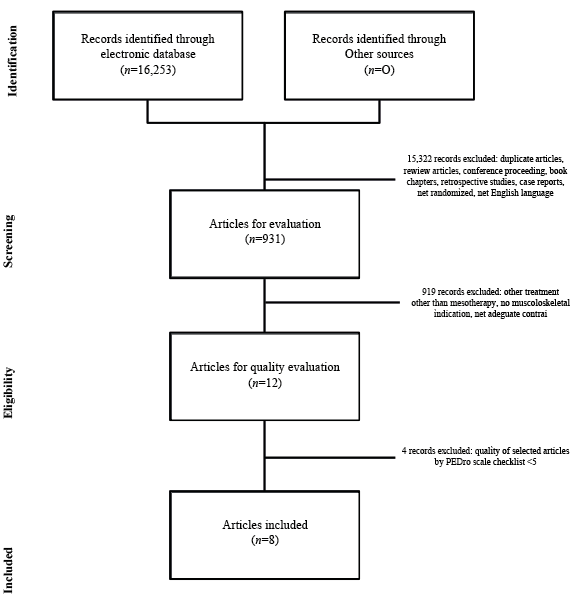 Click to show fullsize
Click to show fullsize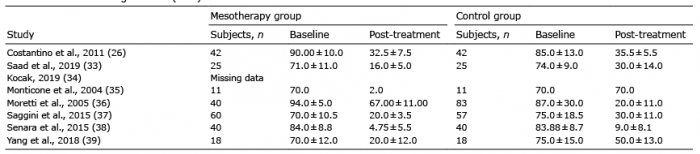 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize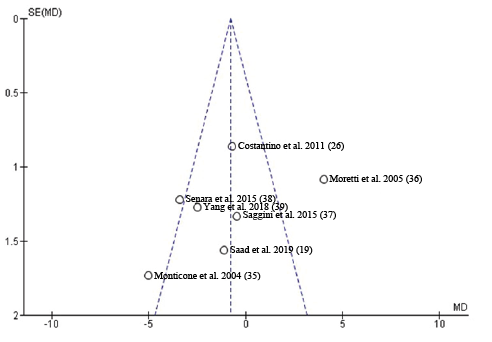 Click to show fullsize
Click to show fullsize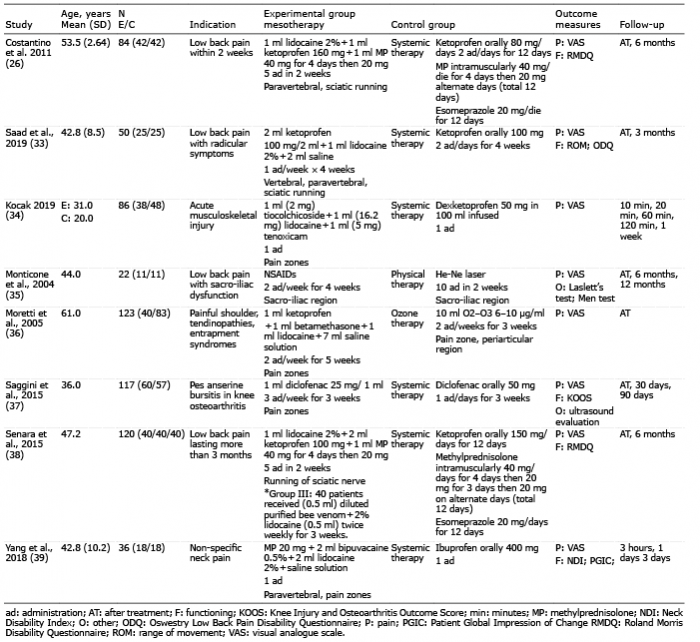 Click to show fullsize
Click to show fullsize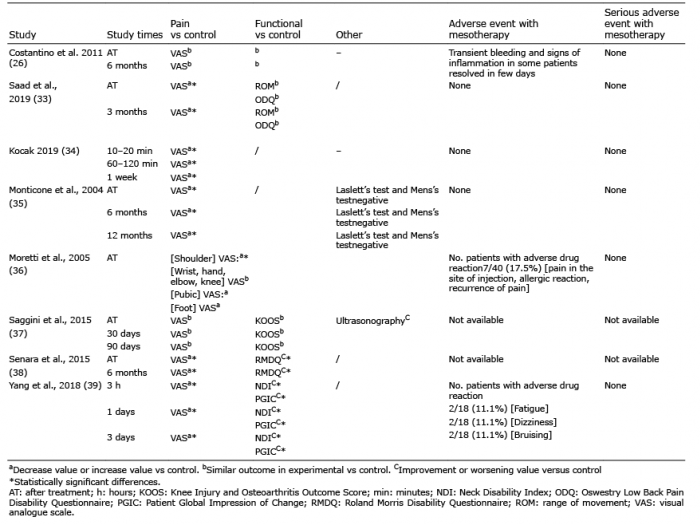 Click to show fullsize
Click to show fullsize