


Takafumi Kamiya1, Kenji Saga1*, Rie Kaneko1, Ichiro Ono1, Masaya Kawada2 and Yoshihoru Maeda2
1Department of Dermatology, Sapporo Medical University School of Medicine, Minami 1 Nishi 16, Chyuo-ku, 060-8543 Sapporo, and 2Department of Surgery, Date Red Cross Hospital, Date City, Hokkaido, Japan. *E-mail: ksaga@sapmed.ac.jp
Accepted June 22, 2005.
Sir,
Ionizing radiation induces various malignant skin tumours. However, only two cases of post-radiation dermatofibrosarcoma protuberans (DFSP) have so far been reported in the literature. We report here another case of DFSP that developed on the skin with chronic radiation dermatitis where the patient had received radiation therapy 75 years earlier. Immunostaining for CD34 was useful for the diagnosis of this case.
CASE REPORT
A 75-year-old woman visited us in May 2003 because of a reddish nodule on her left breast (Fig. 1). The size of the tumour was 12×12×6 mm, and it had increased very slowly since 2000. The nipple of her left breast had not developed. The tumour was on the mottled brown poikilodermatous hard skin on her left breast. Her parents had told her that she had ‘red naevus’ on her left breast when she was born. Although, the size, type and histopathology of the ‘red naevus’ were not known, it must have been a type of haemangioma. She received radiation therapy on that lesion soon after she was born. The records of the dose, fraction and the source of radiation were not available. The haemangioma regressed after radiotherapy and chronic radiation dermatitis had persisted throughout her life.
We excised the tumour under the clinical diagnosis of a benign appendegeal tumour. The scanning magnification of the histopathology showed that the tumour was protruding from the surrounding skin (Fig. 2a). The tumour was asymmetrical and located on the upper dermis underneath the epidermis. Epidermis was thin and flat. No hyperpigmentation of the basal layer was noticed. No grenz zone was present under the epidermis. The lower margin of the tumour was facing thick eosinophilic bundles of collagen. The lower margin of the tumour was well demarcated. The high power view of the histopathology showed the characteristic cart wheel pattern composed of the spindle-shaped tumour cells with blunt nuclei (Fig. 2b). Few mitoses were observed. Immunohistochemistry showed positive staining with CD34 and vimentin. Alpha-smooth muscle actin, S-100, neurofilament, desmin and HMB-45 were negative. Based on these findings, we diagnosed this tumour as DFSP that developed on the site of the chronic radiation dermatitis. Mutation analysis of the tumour material was not available.

Fig. 1. Clinical appearance of the tumour showing a reddish scaly nodule on the poikilodermatous left breast.
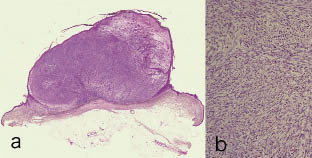
Fig. 2. Scanning magnification (a) of the histopathology showing an asymmetric tumour occupying the upper dermis and protruding from the surface. The lower margin of the tumour is well demarcated and surrounded by eosinophilic compact collagen fibres. High magnification (b) of the tumour shows spindle-shaped tumour cells arranged in irregular intertwining bands, forming a storiform pattern.
Because of frequent local recurrences due to insufficient margin of excision in the DFSP, and of the possibility that radiated skin may induce malignant skin tumours, we excised the whole area of the poikilodermatous hard skin, 3 cm away from the original operation scar. The lower margin of the resection included underlying fascia. In the poikilodermatous skin, orthohyperkeratosis, irregular acanthosis with spongiosis of the epidermis, homogenized collagen fibres and telangiectasia of small blood vessels in the dermis were observed. So called ‘radiation fibroblasts’ with enlarged, stellate-shaped and hyperchromatic nuclei were scattered in the dermis. Immunohistochemistry showed that radiation fibroblasts were positive with vimentin and negative with CD34, alpha-smooth muscle actin, S-100, neurofilament, desmin and HMB-45. One and half years after the excision of the tumour, neither local recurrence nor metastasis was noticed.
DISCUSSION
DFSP is an uncommon, cutaneous sarcoma that has aggressive local behaviour and a high rate of local recurrences in spite of low metastatic potential. DFSPs are anatomically distributed on the trunk (50–60%), on the limbs (25%) and in the head and neck area (10–15%) as shown by Gloster (1). They have a distinct microscopic appearance characterized by fibroblast-like cells arranged in a storiform pattern. Immunohistochemically, tumour cells of DFSPs are stained with CD34, although CD34 is negative in other fibrous tumours (2). Based on the morphology and arrangement of tumour cells in addition to positive staining with CD34, we diagnosed this tumour as a DFSP. However, the present case did not show the infiltration of tumour cells into subcutaneous fatty tissues that is almost always observed in DFSP. Instead, the tumour was protruding from the surrounding skin. Although the reason for this finding is not clear, we speculate that radiation-induced fibrotic dermis might have prevented the infiltration of the tumour cells into the subcutaneous fatty tissues.
Radiation therapy has been considered as an inducer of malignant neoplasms (3). Criteria of post-radiation soft tissue sarcoma normally include the following; i) prior history of radiation, ii) development of the second neoplasm in the field of radiation, iii) a latency period of at least 2 years between radiation and the appearance of the second tumour, and iv) proof that the sarcoma is histopathologically different from the irradiated primary lesion (4). The present case fulfilled all these criteria. Although we could not obtain the record of the radiation therapy, the patient’s memory of her parents’ statement and the signs of the chronic radiation dermatitis on her breast made it clear that she had received radiation therapy.
DFSP constituted less than 0.1% of all cutaneous malignancies and approximately 6% of all soft tissue sarcomas in the United States as reported by Kransforf (5). Laskin et al. (6) reported 53 cases of post-radiation soft tissue sarcoma. The most common soft tissue sarcoma was malignant fibrous histiocytoma (68%), followed by extraskeletal osteosarcoma (13%), fibrosarcoma (11%), malignant schwannoma (4%), extraskeletal chondrosarcoma (2%) and angiosarcoma (2%). No DFSP was found in their study. The dose of radiation therapy varied from 1600 cGy to 7600 cGy. The latency period of the 53 cases ranged from 2 to 40 years with a mean of 10 years and a median of 8 years. Chang et al. (4) reported seven cases of post-radiation sarcoma that developed in 2868 cases of cranial irradiation. Four cases were fibrosarcoma and three cases were malignant fibrous histiocytoma. There are only two case reports (7, 8) of post-radiation DFSP. Although DFSP is rare, it should be included in the differential diagnosis of post-radiation fibrohistiocytic tumours.
The pathogenesis of the soft tissue sarcoma after radiation is not yet clear. Meehan & LeBoit (9) studied the correlation between tumour cells of DFSP and radiation fibroblast, which is characteristically observed in chronic radiation dermatitis. From the differences in immunohistochemical stainings with factor XIIIa, CD34 and HHF-35, they concluded that the tumour cells of DFSP were not derived from radiation fibroblasts. In the present case, radiation fibroblasts were negative for CD34, indicating that radiation fibroblasts were not a source of DFSP. In normal tissues, CD34-positive dendritic cells are located around the blood vessels, nerves, hair follicles and sweat glands (2). CD34- and vimentin-positive intravascular circulating fibroblast-like cells (fibrocytes) were reported to be present (10). These cells are a subpopulation of leukocytes and are supposed to mediate tissue repair. We speculate that these CD34- positive cells can transform into malignancy by radiation directly or by long-term stimulation by cytokines, particularly by transforming growth factor (TGF)-β, secreted from tissues damaged by radiation therapy. The presence of super-numerary ring chromosome has been reported in DFSP. Because of the gene fusion, platelet-derived growth factor-β gene is placed under the control of the promoter of collagen type 1a1 gene in DFSP (11). The product of fused gene stimulates the growth of DFSP in an autocrine or paracrine manner.
REFERENCES
1. Gloster HM Jr. Dermatofibrosarcoma protuberans. J Am Acad Dermatol 1996; 35: 355–374.
2. Aiba S, Tabata N, Ishii H, Ootani H, Tagami H. Dermatofibrosarcoma protuberans is a unique fibrohistiocytic tumour expressing CD34. Br J Dermatol 1992; 127: 79–84.
3. Barcellos-Hoff MH. Integrative radiation carcinogenesis: interactions between cell and tissue responses to DNA damage. Semin Cancer Biol 2005; 15: 138–148.
4. Chang SM, Barker FG, Larson DA, Bollen AW, Prados MD. Sarcoma subsequent to cranial irradiation. Neurosurgery 1995; 36: 685–690.
5. Kransforf MJ. Malignant soft-tissue tumors in a large referral population: distribution of diagnoses by age, sex, and location. Am J Roentgenol 1995; 164: 129–134.
6. Laskin WB, Silverman TA, Enzinger FM. Postradiation soft tissue sarcomas. Cancer 1998; 62: 2330–2340.
7. McLoughlin PM, Girach M, Wood GA. Dermatofibrosarcoma protuberans of the scalp. Br J Oral Maxillofacial Surg 1992; 30: 401–403.
8. Argiris A, Dardoufas C, Aroni K. Radiation induced soft tissue sarcoma: an unusual case of a dermatofibrosarcoma protuberans. Clin Oncol 1995; 7: 59–61.
9. Meehan SA, LeBoit PE. An immunohistochemical analysis of radiation fibroblasts. J Cutan Pathol 1997; 24: 309–313.
10. Bucala R, Spiegel LA, Chesney J, Hogan M, Cerami A. Circulating fibrocytes define a new leukocytes subpopulation that mediates tissue repair. Mol Med 1994; 1: 71–81.
11. Simon MP, Pedeutour F, Sivent N, Grosgeorge J, Minoletti F, Coindre J-M, et al. Deregulation of the platelet-derived growth factor β-chain gene via fusion with collagen gene COL1A1 in dermatofibrosarcoma protuberans and giant-cell fibroblastoma. Nat Genet 1997; 15: 95–98.

