


Hiroo Yokozeki1, Kaoru Takayama1, Ichiro Katayama2 and Kiyoshi Nishioka1
1Department of Dermatology, Graduate School, Tokyo Medical and Dental University, Tokyo, and 2Department of Dermatology, Graduate School of Medicine, Osaka University, Suita, Japan
Atopy patch testing with Japanese cedar pollen extract has been used to investigate patients with atopic dermatitis whose condition is exacerbated by contact with Japanese cedar pollen. Comparative atopy patch testing, scratch tests, and assays for total IgE and specific IgE were performed in 74 patients with atopic dermatitis, 5 patients with Japanese cedar pollinosis and 15 control subjects. A skin biopsy was performed on any sites that were positive to Japanese cedar pollen patch test. The results after 48 h of atopy patch testing were compared with the patient’s history, skin scratch test and specific IgE. Twenty-two of the 74 patients (30%) had a history of exacerbation every spring after contact with Japanese cedar. Of these patients 68% showed a positive reaction to Japanese cedar pollen extract, as did 21% of patients with atopic dermatitis without a history of exacerbation by Japanese cedar pollen, 20% of patients with Japanese cedar pollinosis without eruption and 7% of control subjects. A histological examination revealed eczematous changes and infiltration of lymphocytes and eosinophils in atopy patch testing positive sites. In conclusion, atopy patch testing with Japanese cedar pollen extract is a useful method for investigating trigger factors for eczematous skin lesions in a subgroup of patients with atopic dermatitis. Key words: Japanese cedar pollen; atopic dermatitis; atopy patch test; pollinosis.
(Accepted September 5, 2005.)
Acta Derm Venereol 2006; 86: 148–151.
Hiroo Yokozeki, MD, PhD, Department of Dermatology and Immunodermatology, Graduate School, Tokyo Medical and Dental University, 1-5-45, Yushima, Bunkyo-ku, Tokyo 113-8519, Japan. E-mail: 3064derm@tmd.ac.jp
Atopic dermatitis (AD) is a common, chronically relapsing skin disease. IgE-mediated reactions to aeroallergens have been shown to play a part in a subgroup of patients with AD (1–5). Exacerbations of AD lesions have been described in such patients after contact with animal dander, house dust mites or pollen (4, 5). Horiguchi & Saito (6) reported the existence of patients suffering from Japanese cedar pollinosis in 1964. Air-borne Japanese cedar pollen has been further increasing, with yearly variations, thus leading to a marked increase in the number of patients with pollinosis (7, 8). The average incidence of cedar pollinosis is estimated to be 10–20% in adults and 5–10% in children in Japan (8). Japanese cedar pollen is globe-shaped with a short papilla, measuring 30 µm in diameter. The pollen ruptures in water, resulting in the escape of the intra-grain plasma to the outside of the pollen particle. Two allergenic substances, Cry j 1 and 2, have been extracted and their amino acid sequences have recently been determined (9, 10).
An exacerbation of AD lesions during the Japanese cedar pollen season (January to April) has been reported recently (11); however, it is still not clear whether Japanese cedar pollen causes exacerbation of AD. According to several authors, patch testing with allergens known to elicit IgE-mediated reactions can be used to induce eczematous skin lesions (12, 13). To examine whether Japanese cedar pollen elicits a skin reaction, atopy patch testing (APT) was conducted.
MATERIAL AND METHODS
Patients and controls
Seventy-four patients (40 women, 34 men, mean age 23.5 years) with severe AD were included in this study. All patients presented with AD according to Hanifin & Rajka’s criteria from 1991 to 1999 (14) and were severe cases of adult-type AD. These patients were divided prospectively into two subgroups, according their history. Twenty-two patients reported an exacerbation of pruritus and eczematous skin lesions during the previous Japanese cedar pollen spring season and 52 patients reported no such association. Twenty patients in the first group also suffered from allergic rhinoconjunctivitis (Japanese cedar pollinosis).
The control groups consisted of 5 patients with Japanese cedar pollinosis without any previous or acute skin change and 15 healthy non-atopic volunteers with no history of allergic rhinoconjunctivitis, bronchial asthma or AD. The total and specific IgE to common aeroallergens were normal for the healthy control subjects. All healthy volunteers were free of any skin stigmata due to atopy.
The patients with AD were all in a stable phase of partial or complete remission. Most had a few remaining eczematous skin lesions on some parts of their body but not on their back. Informed consent was obtained from each patient or from his or her parents.
Atopy patch test
APT was performed using a commercial crude Japanese cedar pollen extract (Cryptomeia japonica 1: Cry j 1 3,100 U/ml; Torii Comp., Tokyo, Japan), which was prepared by extracting in 50% glycerin and 5% NaCl aqueous solution; petrolatum was prepared as a negative control. After antihistamines and both systemic and topical steroids (test area) had been discontinued for at least 7 days, 30 μl allergen solution was transferred on a filter paper in the Finn chambers (8 mm; Epitest Ltd, Tuusula, Finland) and the patch test substances were applied for 48 h on the back on clinically uninvolved skin as described previously (15). The skin had been tape-stripped 15 times with 3M tape (3M, Sollentuna, Sweden) as described previously (16, 17). The test reactions were read after 48–72 h. In control areas, a vehicle without allergen was tested.
Skin biopsies were taken from positive patch test reaction sites of 5 patients with AD who consented to skin biopsy. One biopsy was fixed in formaldehyde and 2 µm sections were stained with haematoxylin and eosin.
Scratch test, IgE and statistics
A scratch test with the same commercial crude Japanese cedar pollen extract (Torii Comp., Tokyo) was performed in each subject on the forearms. The serum levels of total IgE were determined and Japanese cedar pollen-specific IgE was measured using RAST (Pharmacia, Uppsala, Sweden). Serum samples were taken before the patch test from each patient and control subjects.
Statistical analysis was performed using the χ2 test to compare the positivity rate for Japanese cedar pollen in different groups.
RESULTS
Atopy patch test reaction
Of the 16 patients with a history of exacerbation of AD during the pollen season (from February to May) and/or pruritus after contact with Japanese cedar pollen (Fig. 1), 68% showed one or more clear-cut positive APTs to Japanese cedar pollen extract (Table I). On the other hand, only 21% of the 19 patients of AD without a suggestive history showed a positive patch test reaction (Table I). In addition, 17% of the patients with Japanese cedar pollinosis were APT positive, while 7% of the healthy subjects showed also a positive reaction (Table I). The sensitivity and specificity of APT are 0.68 and 1.0, respectively.

Fig. 1. Clinical features of a patient with atopic dermatitis exacerbated by Japanese cedar pollen after (A) and before (B) exacerbation.
Table I. Results of allergic tests in patients with atopic dermatitis (AD) and controls
Groups of patients Subjects Total IgE RAST ST APT
(n) (U/ml) (UA/ml)
AD (with a 22 4054 47.7 15/15 11/16
suggestive history) (100%) (68%*)
AD (no suggestive 52 6693 6.2 30/35 4/19
history) (86%) (21%)
Japanese cedar 5 393 40.2 4/5 1/5
pollinosis without AD (80%) (20%)
Normal control 15 ND ND 0/15 1/15
(0%) (7%)
*< 0.05
ST, scratch test; APT, atopy patch test; ND, not done.
A histological examination of APT positive sites (Fig. 2) revealed spongiosis (80%), acanthosis (80%), exocytosis (80%), lymphocyte infiltration (100%) and eosinophil infiltration (60%) in the 5 cases who volunteered for biopsy (Table II).
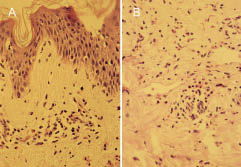
Fig. 2. Histological findings of the patch test sites in a Japanese cedar pollen-sensitized patient with atopic dermatitis. (A) Epidermal findings. (B) Dermal findings.
Table II. Histological features of APT-positive sites in patients with atopic dermatitis. Skin biopsies were taken from positive patch test reaction sites of 5 patients with AD who consented to skin biopsy
Histological findings Subject
1 2 3 4 5
Spongiosis – + +++ + ++
Acanthosis – + + + +
Exocytosis – + ++ + ++
Lymphocyte infiltration + ++ ++ ++ ++
Eosinophil cell infiltration – +++ + – +++
Serum level of IgE and RAST
The serum levels of IgE (geometrical mean values) in patients with AD with a suggestive history, i.e. an exacerbation of AD during the Japanese cedar pollen spring season was 4054 U/ml, that in AD without a suggestive history was 6693 U/ml, and patients with Japanese cedar pollinosis was 393 U/ml, and that in the control subjects was not done.
All patients with AD showed a RAST score of 2 or more Japanese cedar pollen. The average of specific IgE-level in patients with AD and a suggestive history did not differ from those of patients without a suggestive history (Table I).
Scratch test
All the patients with AD with a suggestive story exacerbation due to Japanese cedar pollen showed positive scratch test findings; however 86% of the patients with AD without a suggestive history were also positive.
DISCUSSION
The phenomenon of spring eruption is well known (11, 12). We hypothesized that a subpopulation of patients with AD show exacerbation of symptoms after contact with Japanese cedar pollen in the spring. However, without testing, it is very difficult to identify this subpopulation, since there are a lot of exacerbation factors of AD in the spring season; including sunlight, other pollens, Malassezia and house dust (7–9). We therefore conducted the APT to identify this subpopulation. The results of our studies showed that APT with cedar pollen is a very useful tool to evaluate patients with AD and a history of cedar pollen-induced exacerbation of eczematous skin lesions, identifying 68% of the patients. In control subjects, no APT reaction occurred, but 20% of subjects with Japanese cedar pollinosis and 21% of patients with AD who showed no exacerbation due to cedar pollen also showed a positive APT to Japanese cedar pollen. These results may be explained by the fact that Japanese cedar pollen extract may work as an irritant in AD patients. Most of Japanese cedar pollen APT-positive patients also had a positive scratch test or an elevated specific serum IgE to cedar pollen. No difference was seen the results of the total IgE level, cedar pollen specific IgE level and scratch test. Furthermore, we conducted a histological examination to clarify the mechanism of an exacerbation of AD induced by Japanese cedar pollen. A histological examination revealed spongiosis, acanthosis, exocytosis, lymphocyte and eosinophil infiltration in APT-positive reaction sites. These data indicated that a late phase reaction and contact hypersensitivity caused by Japanese cedar pollen may be a major mechanism in the exacerbation of AD (7, 8).
The higher prevalence of a positive APT reaction to Japanese cedar pollen in patients with a distribution of eczema in air-exposed areas also points to the clinical relevance of our findings. It is important to consider the possible relevance of other aeroallergens, e.g. house dust mite and ultraviolet radiation, in this group. The exact proportion reactive to Japanese cedar pollen remains to be determined. Further studies with specific provocation and elimination procedures need to be performed before APT can be recommended for routine clinical diagnosis of exacerbation of AD due to Japanese cedar pollen.
ACKNOWLEDGEMENTS
We thank Ms Motoko Sekiya for her excellent technical assistance. This work was partially supported by the Cosmetology Research Foundation and grants (13670869) from the Ministry of Education, Japan.
REFERENCES
1. Platts-Mills T, Chapman M, Michell B. Role of inhalant allergens in atopic eczema. In: Ruzica T, Ring J, Przybilla B, eds. Handbook of atopic eczema. Berlin: Springer-Verlag, 1991: 192–203.
2. Ring J, Bieber T, Vieluf D, Kunz B, Przybilla B. Atopic eczema, Langerhans cells and allergy. Int Arch Allergy Appl Immunol 1991; 94: 194–201.
3. Rajka G, Essential aspects of atopic dermatitis. Berlin: Springer-Verlag, 1989.
4. Darsow U, Behrendt H, Ring J. Germinae pollen as trigger factors of atopic eczema: evaluation of diagnostic measures using the atopy patch test. Br J Dermatol 1997; 137: 201–207.
5. Rasanen L, Reunala T, Lehto M, Virtanen E, Arvilommi H. Immediate and delayed hypersensitivity reaction to birch pollen in patients with atopic dermatitis. Acta Derm Venereol 1992; 72: 193–196.
6. Horiguchi S, Saito Y. Japanese cedar pollinosis in Nikko Tochigi. Jpn J Allergol 1964; 13: 16–18.
7. Tanihara S, Oki I, Ojima T, Nakamura Y, Yanagawa H. Process and current status of the epidemiologic studies on cedar pollinosis in Japan. J Epidemiol 1999; 9: 20–26.
8. Okuda M, Shida T. Clinical aspect of Japanese cedar pollinosis. Allegol Int 1998; 47: 1–8.
9. Yasueda H, Yui Y, Shimizu T, Shida T. Isolation and partial characterization of the major allergen from Japanese cedar pollen. J Allergy Clin Immunol 1983; 71: 77–86.
10. Kurihashi M. Physiochemical and immunological characterization of major allergens of Japanese cedar pollen and false cypress. Arerugiika 1997; 3: 203–211 (in Japanese).
11. Oyama K. Cutaneous late-phase reaction to environmental antigen in patients with atopic dermatitis. Dermatology 1993; 187: 182–185.
12. Richard AF, Clark F, Allen D, Adinoff MD. Aeroallergen contact can exacerbate atopic dermatitis: Patch tests as a diagnostic tool. J Am Acad Dermatol 1989; 21: 863–869.
13. Johansson C, Sandström MH, Bartosik J, Särnhult T, Christiansen J, Zargari A, et al. Atopy patch test reactions to Malasseria allergens differentiate subgroups of atopic dermatitis patients. Br J Dermatol 2003; 148: 479–488.
14. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol 1980; Suppl 92: 44–47.
15. Taniguchi H, Yokozeki H, Ohki O, Matsunaga T, Katayama I, Nisioka K. Patch test results in severe adult type atopic dermatitis. Jpn J Dermatol 1997; 107: 781–785.
16. Darsow U, Vieluf D, Ring J. Atopy patch test: Increased sensitivity in patients with an air-exposed pattern of atopic eczema. Br J Dermatol 1996; 135: 182–186.
17. Johansson C, Sandström MH, Bartosik J, Särnhult T, Christiansen J, et al. Atopy patch test reaction to Malassezia allergens differentiate subgroups of atopic dermatitis patients. Br J Dermatol 2003; 148: 479–488.

