


Manuel Ginarte1, Ander Zulaica2 and Jaime Toribio1
Departments of Dermatology, 1Complejo Hospitalario Universitario, Faculty of Medicine, San Francisco SN, ES-15782 Santiago de Compostela, and 2Complejo Hospitalario Xeral-Cíes, Vigo, Spain. E-mail: mginartev@medynet.com
Accepted October 4, 2005.
Sir,
Sarcoidosis is a multisystem disease of unknown aetiology, which is characterized histopathologically by the presence of non-caseating granulomas in the affected organs. Cutaneous involvement occurs in 20–35% of patients with systemic sarcoidosis and it can be categorized as non-specific or specific based on histological findings (1). Non-specific lesions do not have granuloma and are considered as reactive events associated with sarcoidosis elsewhere. The specific cutaneous lesions of sarcoidosis are characterized histopathologically by non-caseating granulomas in the skin and are usually associated with a chronic course of the disease. The clinical picture of specific skin lesions are highly heterogeneous and a wide variety of different cutaneous manifestations have been reported (1, 2). Here we report a very infrequent form of specific cutaneous sarcoidosis that clinically simulated a linear morphea.
CASE REPORT
A 67-year-old Caucasian man presented with a 2-year history of cutaneous induration involving his left leg, knee and thigh. The lesion was asymptomatic but it impaired the complete flexion of the knee. The patient was a retired physician who had worked in a tuberculosis hospital for more than 30 years. He had a familial osteopoikilosis and had been diagnosed with non-specific bilateral uveitis 3 years previously. There was no history of previous trauma to the affected area. He was not taking any medication and did not treat his skin condition with any therapy. Physical examination showed a violaceous, sclerotic, linear area that was attached to the deeper tissues on his left leg and knee and the inner and lower aspect of the ipsilateral thigh (Fig. 1). On palpation two nodules located on the right knee and right buttock were detected. Additionally, examination also revealed a fibrotic plaque on the trunk. Histopathology showed an epidermis with normal characteristics and profuse epithelioid granulomas embracing the upper and lower dermis and subcutaneous fat tissue (Fig. 2). These granulomas were found along with prominent dermal collagenization. Polarized light examination did not show presence of foreign bodies. Stains for mycobacteria and fungi were negative.
Fig. 1. Linear indurated lesion on the medial aspect of the left leg that impaired flexion of the knee.

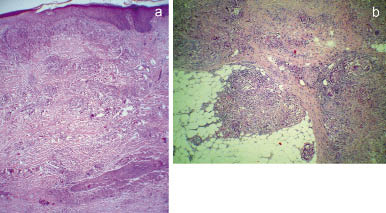
Fig. 2. (a) Epithelioid granulomas with prominent dermal collagenization embracing dermis and subcutaneous fat tissue. (b) Detail of the granulomas (sarcoidal type).
Based on the clinical and histopathological findings, a diagnosis of morpheaform sarcoidosis was made. Complete blood count, serum biochemistry, protein immunoelectrophoresis and urinalysis (including calcium 24-h urine test) did not reveal significant abnormalities. Antinuclear, anti-centromere, and anti-SCL-70 antibodies were negative. Serum levels of angiotensin- converting enzyme were slightly elevated (60 U/l; normal 5–33 U/l). An intradermal purified protein derivative (PPD) test was non-reactive and chest X-ray showed signs of remote tuberculosis (calcified nodule and pleural thickness in the left lower lung lobe) and stage III pulmonary sarcoidosis (thickness of the interlobar septa in middle and upper lobes). Pulmonary function tests revealed restrictive lung disease. Radiographs of the hands and feet and a complete ocular examination did not show abnormalities. The patient was given oral prednisone, 20 mg twice daily, and hydroxychloroquine, 200 mg/day. Within 4 weeks, the induration had improved considerably and the nodules had completely disappeared. The dose of oral prednisone was then gradually reduced for a further 3 months and finally stopped. Hydroxychloroquine was continued for a total of 6 months and withdrawn thereafter. After the first 2 months of therapy, cutaneous lesions had completely regressed leaving only a slight residual pigmentation and pulmonary function test had improved considerably. After the end of the treatment, the disease remained in complete remission during the subsequent 8-month follow-up.
DISCUSSION
Cutaneous sarcoidosis mimicking morphea is a very rare manifestation of cutaneous sarcoidosis and to our knowledge only four cases have been described previously in the English literature (3, 4). These four previously reported patients were women, three black and one white. The clinical picture is indistinguishable from the true morphea, frequently resembling a linear morphea, as in our patient. It is remarkable that three of the patients had chronic arthritis, which is a rare manifestation of sarcoidosis. The cutaneous lesions may precede or arise simultaneously or years after the extracutaneous sarcoidosis. Histopathologically, morpheaform sarcoidosis is characterized by a prominent dermal sclerosis, which is correlated with clinical induration, and the presence of sarcoidal granulomas (4). The mechanisms involved in the fibrosis in this form of sarcoidosis are not known. The activated T cells and macrophages from sarcoidal granulomas release several cytokines that could be a stimulus for secondary collagenization (5, 6).
As in our patient, a good response to antimalarial drugs has been reported, so these drugs may be considered the first choice therapy. Patients with intolerance to antimalarials or without response to them could be treated with systemic corticosteroids.
REFERENCES
1. Kerdel FA, Moschella SL. Sarcoidosis: an update review. J Am Acad Dermatol 1984; 11: 1–19.
2. English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol 2001; 44: 725–743.
3. Hess SP, Agudelo CA, White WL, Jorizzo JL. Ichthyosiform and morpheaform sarcoidosis. Clin Exp Rheumatol 1990; 8: 171–175.
4. Burov EA, Kantor GR, Isaac M. Morpheaform sarcoidosis: report of three cases. J Am Acad Dermatol 1998; 39: 345–348.
5. Thomas PD, Hunninghake GW. Current concepts of the pathogenesis of sarcoidosis. Am Rev Respir Dis 1987; 135: 747–760.
6. Mana J, Marcoval J, Graells J, Salazar A, Peyri J, Pujol R. Cutaneous involvement in sarcoidosis: relationship to systemic disease. Arch Dermatol 1997; 133: 882–888.

