


Elena Campione, Anna Maria Mazzotta, Luca Bianchi and Sergio Chimenti
Department of Dermatology, University of Rome Tor Vergata, Viale Oxford 81, IT-00133 Rome, Italy. E-mail: campioneelena@hotmail.com
Accepted October 21, 2005.
Sir,
Effective systemic treatments for severe acne vulgaris, such as oral antibiotics, oral isotretinoin and anti-androgens, are often associated with undesirable side-effects or are limited to a selected patient population. Furthermore, some patients with severe acne fail to respond to these therapies (1).
Etanercept, a dimeric fusion protein linking part of the human p75 tumour necrosis factor (TNF) receptor extracellular domain with the Fc region of IgG1, is currently approved as monotherapy in Europe and in the USA for subcutaneous administration in patients with moderate-to-severe psoriasis who are candidates for systemic therapy or phototherapy (2). Etanercept targets TNF-α, one of the crucial pro-inflammatory cytokines involved in the pathogenesis of acne (3, 4).
We report here a young man with severe acne unresponsive to standard systemic therapies, who was successfully treated with etanercept.
CASE REPORT
A 22-year-old man was examined for painful, inflamed nodular lesions and sinus tracts as well as pustules and comedones located on the face, neck and trunk (Fig. 1a and b). The patient’s history revealed that acne had developed at the age of 14 years and, over time, had been treated unsuccessfully with topical treatments (benzoyl peroxide, erythromycin, azelaic acid and retinoids), systemic antibiotics (minocyclin: 200 mg/day for 6 months; lymecicline: 300 mg/day for 3 months, and azithromycin: 500 mg/day for 3 consecutive days per month for 3 months) and oral isotretinoin (0.5–1 mg/kg/day for an overall period of 18 months). A few nodular lesions on the zygomatic and mandibular regions had been surgically excised 4 years earlier. Over the last year, the disease had had a severe impact on the patient’s quality of life, causing low self-esteem, anxiety and difficulties in social relationships. The patient reported suicidal ideation. We proposed systemic treatment with etanercept based on the following considerations: (i) disease severity and failure of standard systemic treatments; (ii) patient’s psychological distress, and (iii) mechanism of action of etanercept.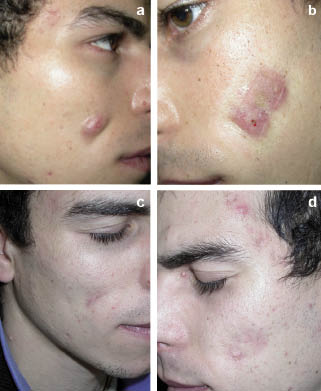
Laboratory investigations (complete blood chemistry profile, urinalysis, lymphocyte subsets, kidney and hepatic function, glycaemia, hepatitis A, B and C markers, and tests for anti-nuclear antibodies), chest X-ray, tine-test and echocardiogram, were performed before initiation of etanercept treatment and revealed no abnormalities. Etanercept was subcutaneously administered at the dosage of 25 mg twice weekly for 24 weeks. Laboratory investigations including complete blood chemistry profile, lymphocyte subsets, kidney and hepatic function, tests for antinuclear antibodies and urinalysis were performed monthly during etanercept treatment and at the end of treatment.
A significant decrease in pain and no appearance of new acne lesions were detected as early as week 2 of treatment. After 12 weeks of treatment, we observed partial regression of the lesions on the face and trunk, and complete regression was achieved after 24 weeks of treatment, with excellent cosmetic results (Fig. 1 c-d). The patient’s psychological status improved.
Laboratory tests performed during and after treatment showed no abnormalities, and no systemic adverse events or injection-site reactions were reported during etanercept treatment. After a follow-up period of 12 weeks, no recurrence was observed.
DISCUSSION
A fundamental initial step in the pathogenesis of acne is excessive sebum production, which provides an anaerobic, lipid-rich environment for Propionibacterium acnes proliferation. In vitro studies using human monocytic cell lines and freshly isolated peripheral blood mononuclear cells from acne patients or normal controls have shown that P. acnes directly stimulates the production of inflammatory cytokines such as interleukin (IL)-8, IL-1b, and TNF-α (3, 4). Graham et al. (5) showed that viable P. acnes in the stationary phase of growth stimulate keratinocytes to produce significantly higher amounts of IL-1b, TNF-α and granulocyte/macrophage colony-stimulating factor (GM-CSF) than unstimulated keratinocytes, suggesting that production of these cytokines may have an important role in the pathogenesis of inflammatory acne lesions.
In the case described here, treatment of severe acne with etanercept was effective and well tolerated, leading to improvements in both clinical manifestations and in the patient’s quality of life. Recently, Cortis et al. (6) described a 22-year-old man with pyogenic sterile arthritis, pyoderma and acne (PAPA) syndrome unresponsive to glucocorticoids, who achieved rapid and sustained remission of the arthritis and complete regression of cystic acne after treatment with etanercept (25 mg/dose twice weekly) for 30 months. High in vitro levels of TNF-α were observed before treatment, suggesting the possible role of TNF-α in the inflammatory process of PAPA syndrome.
Although dermatologic use of etanercept is currently approved in Europe only for psoriasis, several reports have described promising results in a variety of other skin disorders unresponsive to conventional therapies. Larger scale studies are warranted in diseases that are characterized by increased TNF-α production in cutaneous lesions.
ACKNOWLEDGEMENT
The authors wish to thank Barbara J. Rutledge, PhD, for editing assistance.
REFERENCES
1. Zouboulis CC, Piquero-Martin J. Update and future of systemic acne treatment. Dermatology 2003; 206: 37–53.
2. Goldsmith DR, Wagstaff AJ. Etanercept: a review of its use in the management of plaque psoriasis and psoriatic arthritis. Am J Clin Dermatol 2005; 6: 121–136.
3. Rossol S, Voth R, Brunner S, Muller WE, Buttner M, Gallati H, et al. Corynebacterium parvum (Propionibacterium acnes): an inducer of tumor necrosis factor-alpha in human peripheral blood mononuclear cells and monocytes in vitro. Eur J Immunol 1990; 20: 1761–1765.
4. Vowels BR, Yang S, Leyden JJ. Induction of proinflammatory cytokines by a soluble factor of Propionibacetrium acnes: implications for chronic inflammatory acne. Infect Immun 1995; 63: 3158–3165.
5. Graham GM, Farrar MD, Cruse-Sawyer JE, Holland KT, Ingham E. Proinflammatory cytokine production by human keratinocytes stimulated with Propionibacterium acnes and P. acnes GroEL. Br J Dermatol 2004; 150: 421–428.
6. Cortis E, De Benedetti F, Insalaco A, Cioschi S, Muratori F, D’Urbano LE, Ugazio AG. Abnormal production of tumor necrosis factor (TNF) – alpha and clinical efficacy of the TNF inhibitor etanercept in a patient with PAPA syndrome. J Pediatr 2004; 145: 851–855.
Fig. 1. Nodular lesions and sinus tract on the face before etanercept treatment (a-b) and the cutaneous lesions after 24 weeks of etanercept treatment (c-d).

