


Sook Jung Yun, Jee-Bum Lee, Eun Jung Kim, Gen Quan, Seong-Jin Kim, Young-Ho Won and Seung-Chul Lee
Department of Dermatology, Chonnam National University Medical School, Gwangju, Korea
Drug rash with eosinophilia and systemic symptoms (DRESS) is characterized by fever, rash and internal organ involvement after exposure to certain drugs. Most of the aromatic anticonvulsants, such as phenytoin, phenobarbital, and carbamazepine, can induce DRESS. Cross-sensitivity between not only the aromatic anticonvulsants, but also the aromatic and non-aromatic anticonvulsants, is possible. We report here a case of a Korean woman who had previously tolerated valproate, but developed DRESS due to valproate after carbamazepine intake, which indicates cross-sensitivity. Her skin lesions displayed diffuse oedematous patches on the entire body associated with tense bullae on her arms and legs. Circulating auto-antibody to 190-kDa antigen was detected in the patient’s serum by indirect immunofluorescence and immunoblotting, which might contribute to a pathogenic role in DRESS. Key words: auto-antibody; carbamazepine; DRESS; valproate.
(Accepted January 16, 2006.)
Acta Derm Venereol 2006; 86: 241–244.
Jee-Bum Lee, Department of Dermatology, Chonnam National University Medical School, 8 Hak-Dong, Gwangju 501-757, Korea. E-mail: jbmlee@chonnam.ac.kr
Drug rash with eosinophilia and systemic symptoms (DRESS), first reported in 1950 (1), is a rare and potentially life-threatening adverse drug reaction that leads to death in 10% of cases. Anticonvulsants, sulphonamides, dapsone, allopurinol, minocycline and other drugs are causative agents (2). It occurs 2–6 weeks after exposure to, in particular, the aromatic anticonvulsants, such as phenytoin, phenobarbital or carbamazepine (3). Cross-sensitivity between the aromatic and non-aromatic anticonvulsants is possible (4, 5). There are a few reports on the induction of DRESS to a previously well-tolerated aromatic anticonvulsant by a second aromatic anticonvulsant (6, 7). We present here a case of DRESS caused by anticonvulsants, which is unusual because the patient who displayed diffuse generalized erythema on the entire body associated with tense bullae on the arms and legs had previously been able to tolerate valproate, but developed DRESS when given valproate (a non-aromatic anticonvulsant) subsequent to therapy with carbamazepine (an aromatic anticonvulsant). We also detected circulating auto-antibody targeted to epidermal antigen by indirect immunofluorescence (IIF) and immunoblotting studies.
CASE REPORT
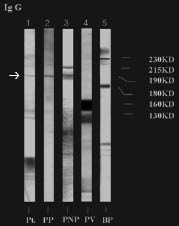
A 39-year-old Korean woman visited the emergency room of our hospital in November 2003, because of pruritic erythematous generalized oedematous patches associated with bullae on her arms and lower legs for 14 days. She also complained of fever and chills. She had a history of epileptic absences for 10 years and had taken intermittent herbal medication. In May 1998, she started treatment with 600 mg/day valproate, and continued this for 11 months without adverse skin rashes during that period. She stopped taking the medication in April 1999. After that, her epileptic attacks were aggravated, so she visited a private clinic and commenced taking carbamazepine from September 2003. After 1 month, she developed facial oedema and suffered from generalized pruritic erythematous patches 2 weeks later. She stopped taking carbamazepine and instead started on valproate, which had been previously well tolerated, 7 days before her visit to our clinic, and her skin lesions were aggravated with bullae formation and oozing, accompanied by fever and chills. Her family history was non-contributory. On physical examination, there was facial oedema with scales and diffuse generalized erythema with tense vesiculobullous lesions on the arms and legs (Fig. 1), and high fever (40oC), but there was no mucosal involvement. Laboratory examination showed leukocytosis (white blood cell count 25,500/μl; normal 4,000–10,000/μl), eosinophilia (16.3%), abnormal liver function tests (aspartate aminotransferase (AST) 70 U/I; normal 10–35 U/I, alanine aminotransferase (ALT) 71 U/I; normal 10–40 U/I), and an elevated lactate dehydrogenase level (1828 U/I; normal 270–530 U/I). After admission, leukocytosis (52500/μl), eosinophilia (34%), and atypical lymphocytes (7%) were increased, and multiple enlarged cervical and axillary lymph nodes were palpated. We stopped all the anticonvulsants and treated her with oral antihistamines and prednisolone 45 mg/day. Subsequently, her high aminotransferase values decreased to normal range without fever. On the 10th day, she had an epileptic attack that was controlled for 2 days with valproate from the department of neurology because valproate was thought to be tolerated; however, her skin lesions were immediately aggravated along with high fever, elevated AST (602 U/I) and ALT (488 U/I), and eosinophilia (21.1%). Seven days after stopping the valproate, the aminotransferase levels were normalized, but she still had eosinophilia (40.1%). A histopathological examination of the vesicular lesion on the lower leg showed subepidermal bullae due to marked oedema in the upper dermis, and perivascular lymphocytic infiltrates with a few eosinophils (Fig. 2). To rule out the possibility of drug-induced autoimmune bullous diseases, such as pemphigus and bullous pemphigoid, we performed IIF and immunoblotting analyses of the patient´s serum. IIF on normal human skin revealed immunoglobulin (Ig)G deposited in the epidermal intercellular space (Fig. 3). Immunoblotting using human epidermal extracts demonstrated that IgG antibodies bound to a 190-kDa polypeptide, which precisely co-migrated with a polypeptide detected by anti-periplakin polyclonal antibody (Santa Cruz, California, USA) and para-neoplastic pemphigus (PNP) serum having auto-antibodies to 210-kDa and 190-kDa antigens (Fig. 4).
Fig. 1. (a) Generalized erythema on the entire body and (b) tense vesiculobullae on the arms and (c) legs.

Fig. 2. Histopathological examination of the legs shows subepidermal oedema with inflammatory cells infiltrate (haematoxylin and eosin, original magnification ×40).
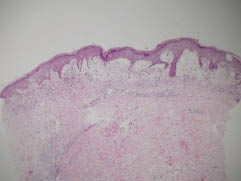
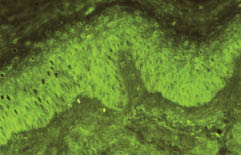
Fig. 3. Indirect immunofluorescence test reveals IgG deposits in the epidermal intercellular space (original magnification ×400).
Fig. 4. Immunoblot analysis using human foreskin epidermal extracts. Lane 1: the patient’s serum. Lane 2: goat polyclonal anti-periplakin antibody. Lane 3: para-neoplastic pemphigus serum having auto-antibodies to 190-kDa and 210-kDa antigens. Lane 4: pemphigus vulgaris serum having auto-antibodies to 160-kDa and 130-kDa antigens. Lane 5: bullous pemphigoid serum having auto-antibodies to 230-kDa and 180-kDa antigens. Arrow indicates the band of auto-antibody to 190-kDa antigen.
A diagnosis of DRESS induced by valproate and carbamazepine was made, and the patient was treated with oral antihistamines and corticosteroids. She is now controlling the epilepsy with 50 mg of topiramate a day and has remained well to date.
DISCUSSION
The clinical manifestations of DRESS occur 2–6 weeks after the start of medication, and they include a maculopapular rash (87%) that often progresses to a pustular eruption or erythroderma, fever (100%), and lymphadenopathy (78%). Internal organ involvement is frequent, and this ranges from mild to toxic hepatitis, nephritis, lung involvement and blood dyscrasia that includes eosinophilia and atypical lymphocytosis (8). Aromatic anticonvulsants are common among causative drugs, but valproate, a broad-spectrum non-aromatic anticonvulsant, rarely induces DRESS (9–12). DRESS due to valproate has been reported while taking ethosuximide at the same time, and skin rashes in a patient of taking valproate are higher when lamotrigine is newly started (13, 14). Our patient, who had been well with valproate, first developed DRESS after starting carbamazepine. She complained of facial oedema and generalized skin rashes after 1 month of taking carbamazepine, which was substituted by valproate, and then symptoms are aggravated.
Cross-sensitivity is as high as 75% among the aromatic anticonvulsants (15, 16) and the cross-sensitivity between valproate and the aromatic anticonvulsants has also recently been reported (4, 5).
It is notable that cross-sensitivity between anticonvulsants is possible in DRESS, not in other adverse cutaneous drug reactions, such as Stevens-Johnson syndrome and toxic epidermal necrolysis. Arevalo-Lorido et al. (4) reported a case of DRESS following exposure to carbamazepine and recurring during treatment with valproate. They suggested that a reaction of circulating antibodies to anti-epileptic drugs was responsible for triggering a clinical cross-reactivity between carbamazepine and valproate. In our report, on the 10th day of admission with normalized liver function tests and improved symptoms, valproate was started again and it immediately triggered a recurrence of DRESS.
There is a strong possibility of cross-sensitivity between carbamazepine and valproate. Induction of DRESS to a previously tolerated anti-epileptic drug by a second anti-epileptic drug was reported between aromatic anticonvulsants (6, 7). The authors demonstrated that patients who experienced DRESS due to an anticonvulsant might have a pre-existing cross-reactivity to other anticonvulsants. In our reported case, it is peculiar that valproate which was previously well tolerated, induced DRESS after carbamazepine.
The complete pathogenesis of DRESS is unknown. Intermediate metabolites of aromatic anticonvulsants (e.g. arene oxides), graft-versus-host disease, human herpes virus (HHV)-6 infection, and immunological mechanism have all been implicated (3, 17–21). An association of auto-immune skin bullous diseases with carbamazepine, was first reported by Yoshimura et al. (22) who recognized increased antibody levels to desmogleins 1 and 3 in 3 out of 25 patients administered carbamazepine without skin rashes, but none in 8 patients with valproate intake. These 3 patients also showed intercellular antibodies to the cell surface of whole epidermis. Patterson & Davies (23) reported a case of carbamazepine-induced pemphigus in a 13-year-old girl showing on direct immunoflourescence an intercellular staining for IgG and C3, but IIF was negative and enzyme-linked immunosorbent assay (ELISA) of anti-desmoglein 1 and 3 was not performed. Clinical features revealed pemphigus foliaceus on the face and pemphigus vulgaris on the trunk and legs manifesting as flaccid blisters and erythema. In our patient, IIF test revealed the IgG deposited in the epidermal intercellular space and immunoblot analysis demonstrated reactivity to 190-kDa protein, which was compatible with the molecular weight of periplakin antibody and PNP serum. These findings suggest that a circulating auto-antibody against the 190-kDa antigen might be produced upon carbamazepine exposure, and that this may have triggered DRESS. Antibody to 190-kDa antigen is usually detected in patients of pemphigus foliaceus and PNP (24, 25). The novel finding in our patient of auto-antibody to 190-kDa in DRESS unrelated to PNP is of particular interest. It is still not clear whether the formation of circulating auto-antibodies targeted to epidermal molecules during DRESS is of primary pathogenic significance or has appeared by the mechanism of epitope spreading. Further studies are warranted to determine the role of the circulating auto-antibody in the pathomechanism of DRESS.
REFERENCES
1. Chaiken BH, Goldberg BI, Segal JP. Dilantin hypersensitivity: report of a case of hepatitis with jaundice, pyrexia, and exfoliative dermatitis. N Engl J Med 1950; 242: 897–898.
2. Tas S, Simonart T. Management of drug rash with eosinophilia and systemic symptoms (DRESS syndrome): an update. Dermatology 2003; 206: 353–356.
3. Knowles SR, Shapiro LE, Shear NH. Anticonvulsant hypersensitivity syndrome. Incidence, prevention and management. Drug Saf 1999; 21: 489–501.
4. Arevalo-Lorido JC, Carretero-Gomez J, Bureo-Dacal JC, Montero-Leal C, Bureo-Dacal P. Antiepileptic drug hypersensitivity syndrome in a patient treated with valproate. Br J Clin Pharmacol 2003; 55: 413–416.
5. Cogrel O, Beylot-Barry M, Vergier B, Dubus P, Doutre MS, Merlio JP, Beylot C. Sodium valproate-induced cutaneous pseudolymphoma followed by recurrence with cabamazepine. Br J Dermatol 2001; 144: 1235–1238.
6. Klassen BD, Sadler RM. Induction of hypersensitivity to a previously tolerated antiepileptic drug by a second antiepileptic drug. Epilepsia 2001; 42: 433–435.
7. Allam JP, Paus T, Reichel C, Bieber T, Novak N. DRESS syndrome associated with carbamazepine and phenytoin. Eur J Dermatol 2004; 14: 339–342.
8. Schlienger RG, Shear NH. Antiepileptic drug hypersensitivity syndrome. Epilepsia 1998; 39: S3–S7.
9. Colletti RB, Trainer TD, Krawisz BR. Reversible valproate fulminant hepatic failure. J Pediatr Gastroenterol Nutr 1986; 5: 990–994.
10. Picart N, Periole B, Mazereeuw J, Bonafe JL. Drug hypersensitivity syndrome due to valproic acid. Presse Med 2000; 29: 648–650.
11. Plantin P, Cartier H, Le Bihan G, Clouard P, Lellouche F, Leroy JP. Drug hypersensitivity syndrome during treatment with valproic acid. Presse Med 1995; 24: 1624.
12. Huang YL, Hong HS, Wang ZW, Kuo TT. Fatal sodium valproate-induced hypersensitivity syndrome with lichenoid dermatitis and fulminant hepatitis. J Am Acad Dermatol 2003; 49: 316–319.
13. Canilleau V, Dompmartin A, Verneuil L, Michel M, Leroy D. Hypersensitivity syndrome due to 2 anticonvulsant drugs. Contact Dermatitis 1999; 41: 141–144.
14. Li LM, Russo M, O’Donhoghue MF, Duncan JS, Sander JWAS. Allergic skin rash with lamotrigine and concomitant valproate therapy. Arq Neuropsiquiatr 1996; 54: 47–49.
15. Shear NH, Spielberg SP. Anticonvulsant hypersensitivity syndrome. In vitro assessment of risk. J Clin Invest 1988; 82: 1826–1832.
16. Hyson C, Sadler M. Cross sensitivity of skin rashes with antiepileptic drugs. Can J Neurol Sci 1997; 24: 245–249.
17. Gleichmann H. Studies on the mechanism of drug sensitization: T-cell dependent popliteal lymph node reaction to diphenylhydantoin. Clin Immunol Immunopathol 1981; 18: 203–211.
18. Leeder JS, Riley RJ, Cook VA, Spielberg SP. Human anti-cytochrome P450 antibodies in aromatic anticonvulsant-induced hypersensitivity reactions. J Pharmacol Exp Ther 1992; 263: 360–367.
19. Descamps V, Bouscarat F, Laglenne S, Aslangul E, Descamps D, Saraux JL. Human herpes virus 6 infection associated with anticonvulsant hypersensitivity syndrome and reactive haemophagocytic syndrome. Br J Dermatol 1997; 137: 605–608.
20. Kano Y, Inoaka M, Shiohara T. Association between anticonvulsant hypersensitivity syndrome and human herpesvirus 6 reactivation and hypogammaglobulinemia. Arch Dermatol 2004; 140: 183–188.
21. Scheuerman O, Nofech-Moses Y, Rachmel A, Ashkenazi S. Successful treatment of antiepileptic drug hypersensitivity syndrome with intravenous immune globulin. Pediatrics 2001; 107: 14–15.
22. Yoshimura T, Seishima M, Nakashima K, Yasuhara Y, Adachi S, Kawaguchi M. Increased antibody levels to desmogleins 1 and 3 after administration of carbamazepine. Clin Exp Dermatol 2001; 26: 441–445.
23. Patterson CR, Davies MG. Carbamazepine-induced pemphigus. Clin Exp Dermatol 2003; 28: 98–99.
24. Ghohestani R, Joly P, Gilbert D, Nicolas JF, Thomine E, Cozzani E. Autoantibody formation against a 190-kDa antigen of the desmosomal plaque in pemphigus foliaceus. Br J Dermatol 1997; 137: 774–779.
25. Kiyokawa C. Envoplakin and periplakin are the paraneoplastic pemphigus antigens. Kurume Med J 1999; 46: 71–78.

